













































12452550.ppt
- 1. Splanchnic Artery Evaluation Lackawanna College Vascular Technology Program
- 2. Splanchnic Arteries Refers to the vessels that supply blood to the bowel Principally, the celiac axis, superior mesenteric artery (SMA) and the inferior mesenteric artery (IMA) Stenosis or occlusion can cause acute or chronic bowel ischemia; however, collaterals usually prevent ischemic bowel
- 3. Three Principal Collateral Paths The pancreaticoduodenal arcade – Links the celiac artery and SMA via branches around the duodenum and pancreas The arc of Riolan The marginal artery of Drummond – Both link the SMA and IMA via mesenteric arterial branches
- 7. Anatomical Variations Vessel I n ci d en ce Celiac Three branches (classic) 65-75% Four branches including dorsal pancreatic artery 5-10% Celiacomesenteric trunk <1% Hepatic Common hepatic from celiac artery 75.00% Common hepatic from SMA 2.50% Replaced right hepatic artery 17-18% From SMA 10-18% From Aorta <2% Replaced left hepatic artery 15-18% From left gastric 11-12% From SMA 0.025 Accessory right hepatic artery 0.078 Accessory left hepatic artery 0.025
- 8. Mesenteric Ischemia Interruption of blood to the small intestine or the right colon Diagnosis is frequently delayed, increasing mortality Aging population, mesenteric ischemia encountered more often Male and female effected equally Early diagnosis improves outcomes
- 9. Mesenteric Ischemia 50% are due to SMA occlusion from thrombus or embolus 25% are due to nonocclusive infarct Remainder are due to IMA occlussion, mesenteric venous thrombosis, or arteritis
- 10. Diagnosis must be suspected in older patients with pain or unexplained GI symptoms The conditions that put the patient at risk: – CHF – Cardiac arrhythmias, particularly a-fib – Recent MI – Atherosclerosis – Hypovolemia – The presence of digoxin may play a role by acting as a splanchnic vasoconstrictor – Patients with history of hypercoagulable state Causes of Mesenteric Ischemia
- 11. Incidence Symptomatic patients have obstructive lesions of celiac and SMA 98-99% of the time One half of those patients also have IMA disease One third have RAS One fourth have infrarenal AAA or occlusive disease
- 12. Frequency, Mortality/Morbidity AMI is involved in .1% of all hospital admits Death rates of 70-90% with traditional methods of diagnosis and therapy More aggressive approach may reduce the mortality rate to 45% Boley, et al, reported a survival rate of 90% if angio was obtained prior to onset of peritonitis
- 13. Acute Versus Chronic Acute Sudden occlusion prior to collateral formation Needs to be treated immediately Chronic Develops over vast time spans Abdominal bruit Allows for formation of collaterals Symptomatic when two of the three mesenteric arteries are effected
- 14. Clinical History Severe abdominal pain, poorly localized Sudden onset if embolic, however gradual onset is more common in mesenteric ischemia Pain is severe and refractory to narcotics Intestinal angina Nausea, vomiting and diarrhea may occur in 50% of patients with mesenteric ischemia Classic triad of SMA embolism: GI emptying, abdominal pain, underlying CAD
- 15. Collateralization Because of extensive collateralization, most splanchnic occlusions are asymptomatic When symptoms do occur, two or three of the splanchnic branches are diseased Autopsies show hemodynamic stenosis in 6-10% of the population There are always exceptions
- 16. Physical Normal abdominal exam in the face of severe abdominal pain Increased abdominal distension, ileus, peritoniti (noted in advanced ischemia)
- 18. Celiac artery is normally low resistive Pre- and post-prandial waveforms are similar Hepatic and Splenic arteries arise from the celiac axis and thus have a low resistive waveform as well Hepatic artery is hepatopedal Splenic artery is hepatofugal Normal Physiology
- 20. Supplies a changing vascular bed Preprandial signals exhibit: – Highly pulsatile signals – Are triphasic – And have somewhat of a reversal component below baseline SMA Pre-prandial
- 21. SMA (post prandial) Changes dramatically post prandial Becomes hyperemic Should remain above baseline Exhibit antegrade flow throughout the cardiac cycle
- 23. Abnormal Physiology Mesenteric stenosis is difficult to detect below 50 % When over 50% waveform characteristics begin to change – Velocity increase – Downstream turbulence – Loss of downstream phasicity – Decreased downstream velocities
- 24. Celiac Artery: Abnormal Velocities >200cm/s suggest a stenosis > or = 70 % Downstream HA & SA exhibit decreased pulsatility and increase in acceleration time In the presence of severe disease the Hepatic artery may be retrograde, and the splenic artery damped
- 25. Example of Decreased AT
- 26. Velocities > 275 cm/s signifies a stenosis >= 70% Doppler bruit at stenotic site Downstream turbulence Decreased downstream velocity Broadened waveform Loss of phasicity downstream SMA Stenosis
- 27. Loss of waveforms reverse component Waveform becomes monophasic and continuous Velocities will drop Pulsatility will decrease SMA Critical Stenosis/Occlusion
- 28. The Median Arcuate Ligament Formed by the fibers of the diaphram Fibers from all origins converge to form a central tendon, which is shaped like a clover leaf – Medial arcuate – over psoas major – Lateral arcuate – over quadratus lumborum – Median arcuate – formed by the union of
- 29. The Median Arcuate Ligament
- 31. Median arcuate ligament can extrinsically compress celiac axis Compression varies with respiration as the ligament slides up and down Expiration impinges, inspiration releases Important to differentiate extrinsic compression from atherosclerotic stenosis The celiac should be interrogated with inspiration and expiration Most are asymptomatic; psychosocial disorder Extrinsic Compression
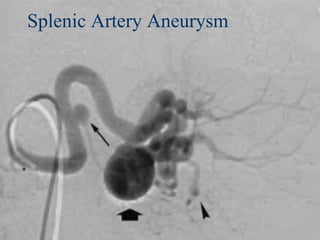
- 32. Splanchnic Aneurysms Not very common Most common, splenic (60%) Hepatic artery (20%) Superior mesenteric artery (5.5%) Celiac artery (4%)
- 34. Splenic Artery Aneurysm 3D
- 35. Splanchnic Aneurysms Ultrasound Appearance Dilated segment of the vessel Swirling effect with color flow analysis Multi-directional, low velocity spectral analysis
- 37. History & Physical History – Post prandial abdominal pain – Onset, and duration of symptoms – Fear of food – Recent weight loss – Risk factors: CAD, Diabetes, Smoker, PVD, CVA/TIA
- 38. Physical Auscultation – Bruit: strength, duration, changes with respiration – Bowel sounds
- 40. Longitudinal and cross sectional images of proximal, mid, and distal aorta
- 41. Proximal Celiac Artery (Doppler angle 60 degrees or less)
- 42. Hepatic Artery (Doppler angle 60 degrees or less)
- 43. Splenic artery (Doppler angle 60 degrees or less) This is a bad example
- 44. SMA (Doppler angle 60 degrees or less)
- 45. Inferior Mesenteric Artery Difficult to visualize with ultrasound Can be a collateral pathway
- 46. Scanning Considerations Casual investigation may miss occlusions when normal flow direction is noted – Celiac occlusion, flow may be reversed in the gastroduodenal and common hepatic arteries
- 48. Celiac Axis Diagnostic Criteria Normal Flow No focal velocity increase No spectral broadening distal turbulence Stenosis >= 70% PSV>200 cm/sec, EDV >=100 cm/sec Doppler bruit, distal turbulence and spectral broadening Dampened waveform in the hepatic and splenic arteries Occlusion of Celiac Axis No flow detected in the celiac artery Retrograde flow in the common hepatic artery Flow in the splenic artery is dampened
- 49. SMA Diagnostic Criteria Normal Flow No focal velocity increase No spectral broadening or distal turbulence SMA stenosis <50% is difficult to detect accurately Stenosis >= 70% Peak systolic velocity >= 275 cm/sec End diatolic velocity >= 70 cm/sec Downstream bruit, turbulence and velocity decrease Spectral broadening Impending Occlusion Total loss of phasicity with low downstream velocity and low pulsatility Collateral flow detected Occlusion No flow noted through the SMA Collateral flow detected