



















































Urinary System Student Notes
- 27. Cortical vs. Juxtamedullary Nephrons Cortical (more than 4/5 of your nephrons): Of little use for significant water retention; mainly contributes to reabsorption and secretion of substances above and beyond those initially separated from blood by filtration. Juxtamedullary (less than 1/5): Besides the same as Cortical , also plays a major role in water retention – regulating whether you’ll produce a dilute or concentrated urine – by creating the Salt gradient through the depths of the medulla region and enabling the reabsorption of water in the Collecting tubule, and with the Vasa recta , being able to reconstitute the blood with this recovered water.
- 28. Cortical vs. Juxtamedullary Nephrons Because of this paucity of Juxtamedulary Nephrons in humans, we are ill-adapted to live in an arid climate. You will die if you’re stranded: in a desert (no water to drink) or at sea (left to drink only sea water) whereas other mammals thrive in this places. Why?
- 29. Adaptations to sea/desert Both marine (sea water) and desert environments will dessicate the body: All mammals adapted to these habitats have an abundance of Juxtamedullary nephrons, and can produce highly concentrated urine, thus eliminating wastes (and also excess salts absorbed by drinking sea water to replenish lost water) using minimum amounts of water in the urine (i.e., more conc. than sea water).
- 30. Interesting factoids: The Kangaroo Rat, Dipodomys sp. , of the american S.W. deserts, never drinks water. It meets its total need for water from just “metabolic water” (a byproduct of carbohydrate metabolism – the last step, combining sugars’ hydrogen and the oxygen you breathe into new water molecules. And it produces a saturated urine, so concentrated that it crystalizes immediately. Sea reptiles and birds, which must drink sea water, do not have such effective kidneys. Despite having to drink sea water, they can eliminate the excess salts with glands (e.g., sea turtles, crocodiles, etc. , use their lacrimal glands; birds use a nasal gland) that produce an extremely salty secretion.
- 34. Cortex-Medulla edge ___ Bowman’s capsule Calyces Shading indicates salt gradient: darker = more concentrated Proximal and Distal Convoluted Tubules Collecting Duct Loop of Henle Ascending Limb Descending Limb The walls of this descending limb are freely permeable to water, but not to salt.
- 35. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 Loss of water by osmosis increases concen. Filtrate stays isosmotic with surrounding tissues: ~1,200 by this point Iso-osmotic, ~320 Water, by osmosis
- 36. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 With this very concentrated ( i.e. , salty) filtrate, the walls of ascending limb (impermeable to water) pump out salt by active transport, eventually diluting the filtrate to very dilute levels, even hypo-osmotic to blood; while leaving lots of salt in the medulla’s interstitial tissue. ~100 Iso-osmotic, ~320 1,200 Salt, by Active Transport
- 37. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 With this very concentrated ( i.e. , salty) filtrate, the walls of ascending limb (impermeable to water) pump out salt by active transport, eventually diluting the filtrate to very dilute levels, even hypo-osmotic to blood; while leaving lots of salt in the medulla’s interstitial tissue. In fact, within limits, this can be thought of as a positive feed back loop: as more salt is pumped out here, the salt gradient increases in the interstitial tissue, and this makes the fluid in the descending limb become more concentrated – this facilitates even more active transport pumping of salt out of this ascending limb.
- 38. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 300 100 Three seemingly obvious questions: What did we accomplish? We started with a filtrate at 300, and ended with a filtrate at 100. Clearly we went in the wrong direction if we’re trying to make a more concentrated urine! After all, “1,200” would be a nice end product concentration. Why didn’t we just stop at the bottom of the loop, at 1,200, and excrete that as our final urine? How do we have a salt gradient from this? Doesn’t the amount of water and salt lost cancel each out? 1,200
- 39. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 Vasa recta flows from the efferent arteriole of the glomerulus Remember that this is the Renal Portal Vein system! This Vasa recta consists of capillaries, and follows immediately the capillaries of the glomerulus. And blood from the glomerulus has a high protein concentration, osmotically unsuitable to be released into general circulation – the lost water must first be reconstituted into the blood!
- 40. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 This region contains large amounts of salt (which should be retained to produce the salt gradient) plus copious amounts of water which must be removed (1) to avoid diluting this salt gradient, and (2) to reconstitute the blood which has, until now, lost ~180 liters of water per day. Thus, the Countercurrent Exchanger! This has to address the problem of having the blood extract large amounts of water from the tissues (from the descending limb of the Loop of Henle and the Collecting Ducts) while not also taking away the salt that is accumulating – and thus protecting the established salt gradient.
- 41. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 Important Note: An ideal countercurrent exchanger is one that will exchange one substance for another on each limb of the loop. E.g., salt would be absorbed into, while water would be lost from, the blood on the first limb; and salt would be lost, while water would be absorbed, in the second limb – and each would counterbalance the other. Perhaps this is what you were taught in General Biology, or in H.S. A.P. Bio? But in reality, fortunately, this is not the case here – it doesn’t work as perfectly as that – otherwise, nothing useful would be accomplished. In reality, proteins in the blood, made more concentrated because they were left in the blood as filtration removed a lot of everything else in the glomerulus, plays an important role in biasing water’s movement in each limb, as I’ll explain subsequently….
- 42. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 Blood first flows down into the depths of the salt gradient – as it passes through saltier tissue, more salt diffuses into the vessel, increasing its salinity while staying iso-osmotic at every level. 300 1,200 salt While salt enters the blood vessel, some water does osmotically move from the blood to the interstitial tissue, but not as much as it otherwise should – the blood proteins (highly concentrated) “hold” much of the water back from such movement, and there’s more salt diffusion into the blood than osmosis of water out of the blood.
- 43. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 However, as the blood rises up the opposite limb of the Vasa recta, it passes through progressively less concentrated tissue and thus salt begins to diffuse out of the blood, again keeping the blood iso-osmotic every step of the way. 300 1,200 salt And likewise, as salt diffuses out of the blood, much more water will actually flow, osmotically, into the blood (as we’ll shortly discuss).
- 44. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 And most of that salt that left that limb, together with any more salt pumped from the ascending limb of the Loop of Henle, winds up diffusing back into the first limb of the Vasa recta. Most of the salt is caught in a “vicious cycle” or “endless loop” – i.e., it just goes in the descending blood and comes out of the ascending blood – and thus trapped here, it creates the salt gradient in the medulla. 300 1,200 salt
- 45. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 Meanwhile, water accumulating in the tissues from the descending limb of the Loop of Henle as well as the Collecting duct (to be discussed next) also enters this limb – its osmotic flow is promoted by the blood proteins (made more concentrated by the loss of water from the blood – i.e. , Filtration – in the glomerulus). 300 1,200 water
- 46. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 300 1,200 So, remember that the concentrated blood proteins bias the movement of water, inhibiting its loss in the downward flow, and yet facilitating its absorption in the upward, return flow. Thus, while salt is captured in a “recycling loop” in this interstitial tissue, more water is absorbed than lost in this “down-then-up” flow, and this net gain of water into the blood enables the recovery of the water needed to fully reconstitute the blood to its original osmotic concentration. Bottom line: we carry away a lot of water and very little salt!
- 47. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 One important note: Although the filtrate entered the distal convoluted tubule at ~100, the surrounding tissue in the cortex is at about 300, so in fact this portion of the tubule will allow an osmotic draw of water from the filtrate, increasing its concentration back up to ~300 again, where it will enter the top of the Collecting Duct. 100 300 water
- 48. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 And as a result, the urea (like salt) also becomes concentrated in the lower portions of the medulla by becoming trapped in a recycling loop – as shown below: There are only two areas that are freely permeable to urea: the lower portions of both the descending Loop (where it isn’t concentrated), and also the Collecting Duct (where it is concentrated, because the urine is concentrated)….
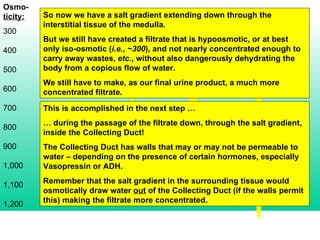
- 49. Osmo- ticity: 300 400 500 600 700 800 900 1,000 1,100 1,200 So now we have a salt gradient extending down through the interstitial tissue of the medulla. But we still have created a filtrate that is hypoosmotic, or at best only iso-osmotic ( i.e., ~300 ), and not nearly concentrated enough to carry away wastes, etc. , without also dangerously dehydrating the body from a copious flow of water. We still have to make, as our final urine product, a much more concentrated filtrate. This is accomplished in the next step … … during the passage of the filtrate down, through the salt gradient, inside the Collecting Duct! The Collecting Duct has walls that may or may not be permeable to water – depending on the presence of certain hormones, especially Vasopressin or ADH. Remember that the salt gradient in the surrounding tissue would osmotically draw water out of the Collecting Duct (if the walls permit this) making the filtrate more concentrated.
- 51. Remember: With more ADH… Not only is more water reabsorbed in the Collecting Duct as well as in the DCT but also … the medulla’s tissues develop a steeper concentration gradient (to facilitate that final water reabsorption), because: more salt is pumped out of the ascending limb of the Loop of Henle, and thus recycled; more urea is recycled and concentrated in the deeper zone of the medulla