2. INTRODUCTION
Anemia is a deficiency in the number of erythrocytes (red blood cell),
the quantity or quality of hemoglobin. It is a prevalent condition with
many diverse causes, such as blood loss, impaired production of
erythrocytes, or increased destruction of erythrocytes. Because RBC’s
transport oxygen, erythrocytes disorders can lead to tissue hypoxia.
3. DEFINITION
Anemia (an- without, emia- blood) is a decrease in RBC count,
hemoglobin and or hematocrit values resulting in a lower ability for the
blood to carry oxygen to body tissues.
6. INCIDENCE
According to the World Health Organization (WHO), anemia affects about 1.62 billion
people worldwide, which is nearly 25% of the global population.
Around 42% of children under 5 years and 40% of pregnant women worldwide are
anemia.
About 30% of non-pregnant women (15–49 years) suffer from anemia, often due to iron
deficiency from menstruation.
Anemia is common in elderly populations due to nutritional deficiencies, chronic
diseases, and decreased red blood cell production.
Conditions like chronic kidney disease (CKD), cancer, and gastrointestinal disorders
contribute significantly to anemia rates.
8. PATHOPHYSIOLOGY
Decreased in RBC’s, Hb, level
Diminished oxygen carrying capacity
Hypoxia or hypoxia-induced effects on organ function
Signs and symptoms of anemia.
9. CAUSES OF ANEMIA
Anemia caused by blood loss
Acute –
Acute trauma
Ruptured aortic aneurysm
GI bleeding
Chronic –
Bleeding duodenal ulcer
Colorectal cancer
Liver disease
Decreased production of RBC
Deficient nutrients – iron, cobalamin,
folic acid
Decreased erythropoietin
Decreased iron available
Increased RBC destruction
Hemolysis –
Sickle cell anemia
Thalassemia
Incompatible blood
11. IRON DEFICIENCY ANEMIA
Iron-deficiency anemia is the most common nutritional disorder in the
world. Those most susceptible to iron-deficiency anemia are the very young,
those on poor diets, and women in their reproductive years.
12. CAUSES
Decreased intake of iron
o Poverty
o Lack of knowledge
o Vegetarian
Decreased absorption of iron
o Tannate (caffeine, tea)
o Wheat (phytate)
o Oxalate (tomato)
o Carbonate-cola
o Sulphate
Increase loss of iron
o Female monthly bleeding
o GI bleeding, ulcer
Increased demand of iron
o Pregnancy
o Lactation
o Child growing age
13. SIGNS AND SYMPTOMS
o Pallor
o Fatigue
o Weakness
o Pica
o Shortness of beath
o Tachycardia
o Koilonychia (brittle nails, spoon shape nails)
15. CBC FINDINGS IN IRON DEFICIENCY ANEMIA
CBC EXPECTED FINDINGS EXPLANATION
Hemoglobin
Hct
RBC count
MCV
MCH
MCHC
Reticulocyte
count
Low
Low
Low
Low (<80fL)
Low
Low
Low
Decreased oxygen carrying capacity
Reflects reduced RBC mass
Fewer RBC due to iron deficiency
Microcytic anemia (small RBC)
RBCs contain less hemoglobin.
Hypochromic pale RBC
Bone marrow lacks iron to produce new RBC.
16. Peripheral blood smear -
Microcytic – RBCs are smaller than normal.
Hypochromic – RBCs have increased central pallor due to reduced hemoglobin content.
Serum iron - decreased due to depleted iron stores and reduced availability for hemoglobin
synthesis.
Total iron binding capacity – increased as the body tries to bind and transport more iron.
Transferrin (a protein that carries iron) – low because iron level is low.
Serum ferritin – most specific marker. It reflects iron storage levels, which are depleted in
iron deficiency anemia.
17. MANAGEMENT
Oral: ferrous sulfate or ferrous
gluconate.
• The daily dose should provide
150-200 mg of elemental iron.
This can be ingested in three or
four daily doses, with each tablet
or capsule of the iron preparation
containing between 50 and 100
mg of iron (e.g., a 300-mg tablet
of ferrous sulfate contains 60 mg
of elemental iron).
IM or IV: iron dextran, sodium
ferrous gluconate, iron sucrose
• Parenteral use of iron is indicated
for malabsorption, intolerance of
oral iron, a need for iron beyond
oral limits, or poor patient
adherence in taking the oral
preparations of iron. Parenteral
iron can be given IM or IV.
19. PERNICIOUS ANEMIA
Pernicious anemia is a decreased in red blood cell that occurs when the
body cannot properly absorb vitamin B12 from the gastrointestinal tract.
Vitamin B12 is necessary for the proper development of red blood cells.
It occurs mostly due to lack of intrinsic factor that helps in the
absorption of vitamin B12. Vitamin B12 is absorbed in terminal ileum.
20. CAUSES
Decreased intake of vitamin B12- vegans diet, poor nutritional intake
Decreased absorption – intrinsic factor deficiency, malabsorption disorder.
Increased loss – chronic alcoholism, chronic diarrhea
Increase demand – pregnancy
Gastrectomy – parietal cell in the stomach secretes intrinsic factor, which is
essential for vitamin B12 absorption. After gastrectomy the body can longer
produce adequate intrinsic factor.
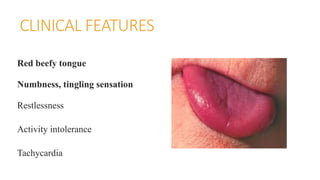
21. CLINICAL FEATURES
Red beefy tongue
Numbness, tingling sensation
Restlessness
Activity intolerance
Tachycardia
22. DIAGNOSTC STUDY
CBC EXPECTED
FINDINGS
EXPLANATION
Hemoglobin
Hematocrit
RBC count
MCV
MCH
MCHC
Reticulocyte
Low
Low
Low
High (>100fL)
High
Normal
Low
Reduced oxygen carrying capacity
Due to anemia
Fewer RBC produced due to impaired DNA synthesis
Macrocytic anemia due to defective RBC maturation.
RBC are large and may have more hemoglobin
Color remains normal (normochromic)
Bone marrow suppression from defective production.
23. Contd.
Peripheral blood smear –
Macrocytic: the hallmark of pernicious anemia is the presence of macrocytes which are larger than
normal red blood cell.
Normochromic – even though the RBC are larger they typically contain normal level of
hemoglobin. Therefore, they retain normal color.
Schilling test - Purpose: To assess whether the vitamin B12 deficiency is due to impaired absorption
in the ileum.
Normal Result: If the B12 is absorbed properly, the urine will contain a high amount of radiolabeled
B12.
Abnormal Result: If B12 absorption is impaired, less B12 will appear in the urine.
24. MANAGEMENT
If absorption of vitamin B12 occur then enteral therapy is given. Oral
Vitamin B12 (Methyl cobalamin).
If absorption of vitamin B12 does not occur then parenteral therapy is
given. IV or IM Cyanocobalamin (lifelong treatment).
25. MEGALOBLASTIC ANEMIA
It is a type of anemia in which there is deficiency of Vitamin B12
(cyanocobalamin) and Vitamin B9 (folic acid).
These vitamins are responsible for the maturation of the immature RBC
(reticulocyte).
So, in absence of these vitamin the cells are unable to divide and increase in
size so it is called megaloblastic anemia.
It mainly occurs due to deficiency of Folic acid, Vitamin B9.
26. CAUSES
Decreased intake of folic acid - Poor dietary intake, common in malnourished
individuals, alcoholics, and the elderly, can lead to folic acid deficiency.
Decreased absorption of folic acid - Gastrointestinal surgeries, such as gastric
bypass or small bowel resection. Medications, such as phenytoin, methotrexate, and
sulfasalazine, which interfere with folate absorption
Increase loss - Excessive alcohol consumption, which impairs folate metabolism and
increases its excretion in urine. Kidney disease and dialysis, as folic acid is lost
during hemodialysis
Increase demand - Pregnancy, due to rapid fetal growth and increased red blood cell
production. Lactation, where folate is required for milk production.
27. DIAGNOSTIC STUDY
CBC EXPECTED FINDINGS EXPLANATIONS
Hemoglobin
Hct
RBC count
MCV
MCH
MCHC
Reticulocyte count
Low
Low
Low
High (>100fL)
High
Normal
Low
Reduced oxygen carrying capacity.
Due to anemia
Fewer RBC’s due to defective DNA synthesis
Macrocytic anemia due to large RBC
Large RBC hold more hemoglobin
RBC were well fitted with hemoglobin
Ineffective erythropoiesis due to defective
maturation
28. CONTD.
Peripheral blood smear –
Macrocytic – RBC larger than normal red blood cell.
Hypochromic – RBSs have a lower-than-normal amount of hemoglobin.
Schilling test.
29. MANAGAMENT
Vitamin B12 and folic acid diet like green leafy vegetable (e.g.
spinach).
Folic acid supplementation - the usual dose is 1mg/day by mouth. In
malabsorption state up to 5mg/day may be required.
30. APLASTIC ANEMIA
Aplastic anemia is a disease in which the patient has peripheral blood
pancytopenia (decreased of all blood cell types – RBCs, WBCs and
platelets) and hypocellular bone marrow.
Anemia is due to bone marrow failure or bone marrow depression in
which bone marrow stops making enough new blood cells.
31. CAUSES
Causes have to do with damage to the stem cells in the bone marrow
that are responsible for blood cell production.
Exposure to toxic substances such as arsenic, benzene or pesticides.
Cancer therapy
Viral infection , hepatitis, HIV
Autoimmune disorders (cytotoxic cells, T killer cells)
Red bone marrow replaces by fat cell.
32. CLINICAL MANISTATION
Reduced RBC – Anemia (pallor, tachycardia, fatigue, weakness)
Reduced WBC – increased infection risk, neutrophilia (low grade
fever should ne consider as a medical emergency)
Reduced platelets – thrombocytopenia, increased bleeding risk (nose
bleeding, gum bleeding, pinpoint red bleeding spot on the skin, blood
in the stool, petechiae, ecchymosis)
33. DIAGNOSTIC STUDY
CBC EXPECTED
FINDINGS
EXPLANATION
Hemoglobin
Hematocrit
RBC count
MCV
WBC count
Platelet count
Reticulocyte count
Low
Low
Low
Normal or
slightly
increased
Low
Low
Low
Due to reduced RBC production
Reflect the severity of anemia
Bone marrow cannot produce enough RBC’s
RBC may be normal size or maybe slightly
macrocytic
Increased risk for infection due to low
neutrophil
Thrombocytopenia. Increased bleeding risk
Bone marrow failure (no new RBC
production)
34. CONTD.
Confirmatory test – Bone marrow biopsy
It will show an overall decreased in the number of blood cells, and is
hypocellular with increased yellow marrow (fat content).
Serum iron, total iron binding capacity – may be elevated as initial
sign of erythropoiesis suppression.
35. MANAGEMENT
Bone marrow transplantation
Infections due to immunosuppression – immunosuppression drugs are
given for lifetime e.g. steroids, cyclosporin etc.
PRBC transfusion – are given to maintain hemoglobin level and reduce
symptoms like fatigue, breathlessness.
Iron overload prevention: Frequent transfusions can cause iron overload,
requiring iron chelation therapy (deferoxamine, deferasirox).
RDP and SDP transfusion – Given if platelet count <10,000/µL or if there
is active bleeding.
36. Precaution to be taken for infection
Strict hygiene and aseptic
precautions.
Prophylactic antibiotics in patients
with severe neutropenia.
Avoidance of crowded places and
live vaccines.
Early treatment of infections with
broad-spectrum antibiotics.
Precaution for bleeding –
Use soft-bristled toothbrushes to prevent
gum bleeding.
Avoid sharp objects like razors (use electric
shavers instead).
Wear protective clothing and shoes to
prevent cuts and bruises.
Be cautious with physical activities; avoid
contact sports.
37. SICKLE CELL ANEMIA
It is a serious disorder in which the body makes sickle – shape red blood cells. Sickle
shape means that the red blood cell are shape like a crescent. It is a group of
inherited, autosomal recessive disorders characterized by an abnormal form of
hemoglobin in the RBC. If both parents are carrier and disease may occur in child.
RBC contain abnormal hemoglobin, which in absence of oxygen convert to
sickle shape, cells become rigid and clump together, so obstructing blood
capillaries.
Precipitating factors for sickling are fever, dehydration, stress, high altitude.
39. Due to chromosomal or genetic defect in beta chain of haemoglobin
At the position of chromosome 6
Substitution of glutamic acid by valine
Abnormal formation of haemoglobin (HbS)
Resulting in sickle cell shape (sensitive to hypoxia)
Due to trigger factor
haemoglobin interacts with each other (clump) due to sickle shape
40. occlusion of vessels, Vaso occlusion (decreased blood flow, ischemia, necrosis)
Trigger removes Repeated exposure to trigger
Resolve hypoxia by oxygen therapy RBC membrane destroy
RBC becomes normal shape (biconcave shape) Haemolysis
Anemia jaundice
42. CLINICAL MANIFESTATION
Yellowing of eyes and skin (jaundice, due to RBC break down)
Sickle cell crisis: It is a very severe, painful, acute exacerbation of RBC
sickling, causing a Vaso occlusive crisis. As blood flow is impaired by
sickled cells, vasospasm occurs, further restricting blood flow. Tissue
ischemia, infarction, and necrosis eventually occur from lack of O2.
Vaso-Occlusive Crisis (Pain Crisis): Most common complication due to
sickled RBCs blocking blood flow.
Severe pain episodes, often in the bones, chest, abdomen, and joints.
43. CONTD.
Sequestration crisis: it occurs when spleen pull the sickled cell from
body. Spleen become massively large (splenomegaly). Clinical
manifestation includes hypotension, hypovolemia, shock.
Strokes: Blockage of cerebral blood vessels can cause ischemic stroke
(paralysis, seizures, altered consciousness).
Acute Chest Syndrome (ACS) - Medical Emergency: Sickling in lung
blood vessels leads to chest pain, cough, difficulty breathing, and hypoxia.
44. DIAGNOSTIC STUDY
Sickling Test (Sodium Metabisulfite Test)
A drop of sodium metabisulfite is added to the blood sample to induce sickling of RBCs.
Positive result: Sickled red blood cells appear under the microscope.
Used as a preliminary screening test.
Sickle Dex Test
Blood is mixed with a reducing agent; HbS precipitates, making the solution turbid
(Cloudy). If negative clear solution.
Used in newborn screening and carrier detection.
46. Contd.
DNAAnalysis (Genetic Testing)
Identifies mutations in the Hb gene responsible for sickle cell disease.
Used in prenatal diagnosis (amniocentesis, chorionic villus sampling).
Complete Blood Count (CBC) with Peripheral Smear
Low hemoglobin (6-10 g/dL) due to chronic hemolysis.
Increased reticulocyte count (bone marrow compensation).
Peripheral smear findings: Sickle-shaped RBCs, elongated crescent shape RBC’s
47. Symptomatic Management
Oxygen Therapy: Improves oxygen delivery to tissues.
Reduces RBC sickling by increasing oxygen saturation.
Fluid Therapy (Hydration )- Dehydration increases blood viscosity,
promoting RBC sickling.
Avoid Stress
Joint Pain Management (Due to Vaso-Occlusive Crisis)
Avoid Cold Temperature: Cold-induced vasoconstriction reduces blood
flow, increasing the risk of sickling and pain crises.
48. Definitive Management
Bone Marrow Transplantation (BMT) – Only Curative Treatment
Management of Splenomegaly
Splenic sequestration crisis: Sudden trapping of RBCs in the spleen → shock & severe
anemia.
Splenectomy (Surgical Removal of Spleen)
Hydroxyurea – First-Line Drug Therapy
Mechanism: replaces beta chain to gamma chain, fewer sickle RBCs. Reduces sickling.
Decreases pain crises, acute chest syndrome, and transfusion need.
49. THALASSEMIA
It is an inherited autosomal recessive disorder.
It occurs due to problem in chromosome 11 (beta) and 16 (alpha).
Thalassemia is characterized by hypochromic (an abnormal decrease in the
hemoglobin content of erythrocytes), extreme microcytosis (smaller than normal
erythrocyte), hemolysis.
Thalassemia is classified into two major groups according to which hemoglobin chain
is diminished: alpha and beta
50. Alpha thalassemia
• mainly occur in people from Asia
and the Middle East. It is due to
problem in chromosome 16. It is
milder than the beta thalassemia
and often occur without
symptoms, the erythrocytes are
extremely microcytic but anemia if
present is mild.
Beta thalassemia
• are most prevalent in people from
Mediterranean regions. It is due to
problem in chromosome 11.
• Beta thalassemia is divided into
three types:
oBeta thalassemia minor – it is
asymptomatic
oBeta thalassemia intermediate –
intermittent symptoms
oBeta thalassemia major –
symptomatic. It is also known as
Cooley’s anemia.
51. Due to problem in globin chain of hemoglobin
Decreased beta chain and increased alpha chain
Leading to defective hemoglobin, can damage RBC membrane
Due to early destruction of RBC in circulation
Hemolysis
Microcytic hypochromic
52. Thalassemia Major severe symptoms
o Severe anemia (Hb: <7 g/dL)
o Growth retardation & delayed puberty → Due to chronic hypoxia.
o Severe jaundice → Due to increased RBC destruction.
o Hepatosplenomegaly (enlarged liver & spleen) → Due to excessive RBC destruction and
extramedullary hematopoiesis.
Skeletal abnormalities:
o Frontal bossing (prominent forehead).
o Chipmunk facies (maxillary overgrowth).
o Thinning of long bones, increasing fracture risk.
o Thin upper lip, low nasal bridge
54. Iron overload symptoms (from repeated transfusions):
o Bronze skin pigmentation.
o Cardiac failure (due to iron deposition in the heart).
o Liver damage (cirrhosis, hepatomegaly).
55. Diagnostic study (hemoglobin electrophoresis)
Condition HbA HbA2 HbF Key
features
Normal 95-98% 1.5-3.5% <2% Normal
hemoglobin
pattern
Beta
thalassemi
a major
0% Increased
(4-8%)
Increased
(50-90%)
Severe
anemia
56. CBC
CBC EXPECTED FINDINGS EXPLANATION
Hemoglobin
Hematocrit
RBC count
MCV
MCH
Reticulocyte count
Low
Low
High
Low
Low
High
Reduced hemoglobin synthesis
Reduced RBC volume
Increased RBC production to
compensate
Severe microcytosis
Hypochromic
Bone marrow compensation.
58. MANAGEMENT
Thalassemia Minor (Trait) –
No Treatment Needed
o Usually asymptomatic or mild
anemia.
o Advice: Normal diet, folic
acid if needed, genetic
counseling for future
pregnancies.
Thalassemia Intermedia – Symptomatic
Treatment
o Occasional Blood Transfusions → For
symptomatic anemia or growth retardation.
o Iron Chelation (if transfused regularly) → To
prevent iron overload.
o Hydroxyurea → Can increase fetal hemoglobin
(HbF) and reduce symptoms.
o Splenectomy (if needed) → For severe
splenomegaly causing excessive RBC destruction.
59. Thalassemia Major (Cooley’s
Anemia) – Intensive Treatment
o Regular Blood Transfusions
(Lifelong Treatment)
o Every 2-4 weeks to maintain Hb >
9-10 g/dL.
o Prevents growth failure, bone
deformities, and cardiac
complications.
Bone Marrow Transplant (Only
Curative Treatment)
Iron Chelation Therapy (Prevents Iron
Overload)
Chronic transfusions cause iron overload,
leading to organ damage.
Chelation removes excess iron:
o Deferasirox (Oral) – First-line drug.
o Deferoxamine (Injection) – Used in severe
cases.
60. HEMORRHAGIC ANEMIA
ACUTE BLOOD LOSS
• Acute blood loss occurs as a result of
sudden hemorrhage.
• There are two clinical concerns in such
situations. First, a sudden reduction in
the total blood volume can lead to
hypovolemic shock. Second, if the acute
loss is more gradual, the body maintains
its blood volume by slowly increasing
the plasma volume. Although the
circulating fluid volume is preserved,
the number of RBCs available to carry
O₂ is significantly diminished.
CHRONIC BLOOD LOSS
• The effects of chronic blood loss are
usually related to the depletion of iron
stores and considered as iron-deficiency
anemia. Management of chronic blood
loss anemia involves identifying the
source and stopping the bleeding.
Supplemental iron may be required.
62. NURSING DIAGNOSIS
o Activity Intolerance related to decreased oxygen-carrying capacity of the blood as evidenced by fatigue,
weakness, shortness of breath on exertion, increased heart rate.
o Impaired Gas Exchange related to decreased hemoglobin levels and reduced oxygen transport as
evidenced by dyspnea, pallor, cyanosis, low oxygen saturation levels.
o Imbalanced Nutrition less than Body Requirements related to inadequate intake or absorption of iron,
vitamin B12, or folic acid as evidence by weight loss, pale mucous membranes, brittle nails, glossitis
(inflamed tongue).
o Risk for Bleeding Related to decreased platelet function or severe anemia as evidenced by bruising,
petechiae, prolonged bleeding time, hematuria.
o Risk for Infection Related to impaired immune function due to chronic anemia and possible bone marrow
suppression as evidenced by frequent infections, delayed wound healing, leukopenia (in some cases).
o Ineffective Tissue Perfusion Related to reduced oxygen supply to tissues due to low hemoglobin levels as
evidenced by cold extremities, delayed capillary refill, dizziness, confusion in severe cases.
63. NURSING MANAGEMENT
Activity Intolerance
Encourage frequent rest periods between
activities.
Monitor vital signs (heart rate, oxygen
saturation) before and after activity.
Assist with ADLs (Activities of Daily Living)
as needed.
Educate about gradual activity progression to
improve endurance.
Promote balanced diet and hydration to support
energy levels.
Impaired Gas Exchange
Monitor oxygen saturation (SpO2) and
provide oxygen therapy as needed.
Position patient in semi-Fowler’s to
improve lung expansion.
Assess for dyspnea, cyanosis, and
respiratory distress.
Administer blood transfusions if indicated.
Encourage deep breathing exercises to
improve oxygenation.
64. Imbalanced Nutrition: Less Than Body
Requirements
Encourage a diet rich in iron, folic acid, and
vitamin B12 (e.g., leafy greens, red meat,
eggs, dairy).
Administer iron supplements (oral or IV) as
prescribed.
Provide vitamin B12 injections for pernicious
anemia.
Educate on iron absorption (e.g., take iron
with vitamin C, avoid tea/coffee with meals).
Monitor weight, appetite, and dietary intake.
Risk for Bleeding
Monitor platelet count and coagulation
studies.
Avoid IM injections, invasive procedures,
and blood thinners unless necessary.
Educate on safety measures (soft
toothbrush, electric razor, fall precautions).
Assess for signs of bleeding (petechiae,
bruising, nosebleeds, hematuria).
Administer blood products (platelets,
clotting factors) if needed.
65. Risk for Infection
Monitor WBC count and signs of
infection (fever, chills, sore throat).
Maintain strict hand hygiene and
encourage infection control measures.
Administer prophylactic antibiotics or
vaccinations if prescribed.
Encourage good oral hygiene to
prevent infections.
Educate on avoiding crowded places
and sick individuals.
Ineffective Tissue Perfusion
Monitor capillary refill, skin color, and
temperature.
Assess for dizziness, confusion, and syncope.
Encourage hydration to maintain blood
volume.
Administer blood transfusions or IV fluids if
ordered.
Educate on avoiding extreme temperatures
that may worsen symptoms.
66. CONCLUSION
Anemia is a common hematologic condition that results from a decrease in the number of red blood
cells or hemoglobin, impairing the body's ability to deliver oxygen to tissues. It can be caused by
various factors, including nutritional deficiencies (iron, vitamin B12, folate), chronic diseases, genetic
disorders, and blood loss.
Early diagnosis and intervention are crucial in preventing complications such as organ damage, growth
retardation, or exacerbation of underlying conditions. Effective nursing care, including monitoring,
nutritional support, and patient education, plays a vital role in improving outcomes for individuals with
anemia.
With appropriate management, most individuals with anemia can experience a significant improvement
in quality of life and avoid long-term complications.
67. BIBLIOGRAPHY
Lewis’s, Heitkemper, Harding, Kwong, Roberts, Bucher. 4th edition, Medical Surgical
Nursing Assessment and Management of Clinical Problems, Volume 2, 4th South Asia ed.
Elsevier, page no.602-614.
Javed Ansari, Davinder Kaur, PV A textbook of medical surgical nursing 1, S.Vikas and
company (medical publisher) India, page no.872-892.
Suresh K. Sharma, S. Madhavi, Brunner and Suddath’s Textbook of medical surgical nursing,
volume 1, South Asian Edition, Wolters Kluwar (India) Pvt.Ltd. New Delhi. page no. 721-
736.
PR Yadav, Competitive handbook of nursing, Aravali publication, 4th edition, volume 1,
page no. 21-24.
https://www.slideshare.net/sabisiddh/anemia-25085879
https://www.slideshare.net/slideshow/anemia-33264247/33264247
https://medicine.missouri.edu/sites/default/files/Anemia-Lecture-for-M3-class.ppt