































![Psychiatric Association [APA], 2000). The mood disturbance may involve de- pression or elevated, expansive, or irritable mood, and
causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. Types of
physiological influences are included in the discussion of etiological implications for bipolar disorders.
SUBSTANCE-INDUCED BIPOLAR DISORDER: The disturbance of mood associated with this disorder is considered to be the
direct result of physiological effects of a substance (e.g., a drug of abuse, a medication, or toxin exposure). The mood disturbance may
involve depression or elevated, expansive, or irritable mood, and causes clinically significant distress or impairment in social,
occupational, or other important areas of functioning Mood disturbances are associated with intoxication from substances such as
alcohol, amphetamines, cocaine, hallucinogens, inhalants, opioids, phencyclidine, sedatives, hypnotics, and anxiolytics
CLINICAL MANIFESTATION
MANIC PHASE DEPRESSIVE PHASE
Expensive, grandiose, or hyperirritable mood √ Low self esteem -
Increased psychomotor activity such as agitation pacingor hand
wringing
- Overwhelming inertia -
Excessive social extroversion - Feeling of Hopelessness, Apathy, self reproach -
Rapid speech with frequent topic changes - Difficulty concentrating, intellectualimpairment -
Decreased need for sleep and food √ Psychomotor Retardation -
Impulsivity - Anhedonia -
Impaired judgement - Suicidal Ideation √](https://image.slidesharecdn.com/casepresentation1-250826105119-4033b372/85/CASE-PRESENTATION1-pdf-bipolar-disorder-in-which-both-mania-and-depression-happen-38-320.jpg)











CASE PRESENTATION1.pdf bipolar disorder in which both mania and depression happen.
- 1. MODERN NURSING COLLEGE ANNANDALE SHIMLA-03 MENTAL HEALTH (PSYCHIATRIC)NURSING CASE PRESENTATION- 1 ON BIPOLAR AFFECTIVE DISORDER WITH CLUSTER B TRAITS SUBMITTED TO: SUBMITTED BY: MRS. RITU RILTA SEEMRAN THAKUR ASSISTANT PROFESSOR M.Sc. NURSING 1ST YEAR MENTAL HEALTH (PSYCHIATRIC) NURSING ROLL NO, 06 SUBMITTED ON:16/08/2024
- 2. I. IDENTIFICATION DATA Name : Mrs. Chander Rekha Age (in years) : 26 years Sex : Female Bed no. : 28 Name of Ward : Psychiatry ward Date of admission (with time) : 23/ 02/ 24 CR. No. : 202111201454 Identification mark : not significant Language : Hindi, Pahadi Educational status : Graduation Urban/ Rural : Rural Dietary habits : Non- vegetarian (egg, meat etc.) Marital status : Married
- 3. Religion : Hindu Nationality : Indian Occupation : Unemployed Socio- economic status : 15,000/- per annum Informant : Patient herself : Father- Jay Dev, 50 year, 8th pass, occupation- field worker, currently staying with patient for 1 year Information : Adequate and reliable Address :Village Kothari, P.O. Ghasani Tehsil Rohru, District Shimla (H.P). MSE done on :2,3,4 march 2024 Final diagnose : F31.6 with cluster- B traits with Z63.0 with Vit. D3 deficiency II. PRESENTING CHIEF COMPLAINTS: According to patient: Mn udaas h.X 1 month
- 4. According to informant: Ghussa krti h X 1 month 7 days Ajeeb awajen nikalti h X 1 month 7 days Khana nahi khana chahti h X 1 month 7 days III. HISTORY OF PRESENT ILLNESS: Mode of onset: Chronic Course: Episodic Total duration of illness: 1 month 7 days for current episode Precipitating factor: Not known, IPR issues Predisposing factor: Not present. Facilitating factor: Not present DESCRIPTION OF PRESENT ILLNESS: Patient is a known case of F31.6 with cluster B- traits one episode of illness and admission in past with symptoms of irritability, disturbed sleep, decreased appetite, and was on medication Tab. Diva (750 mg), Tab. Olanzapine (5mg), Tab. Lorazepam (1.5 mg)till 19 August 2022 when she visited OPD in IGMC. After consultation on returning home she stopped all medication and when asked by her family members she would say that she will not take the medication because these medication will harm her body, and she would also refuse food sometimes. The client discontinued the medications till 15 January 2023 but her overall behavior was normal.
- 5. Suddenly on 15 January 2023 she started shouting on her family members and according to her father she would undress herself in his house, make weired noises loudly when her family members tried to stop her. She would become angry and she would start running to nearby houses and would enter others houses in villages, whenever her family tried to stop her she would say, “ Tum mere raaste se hut jao.”, “ Mujhe jahan jane ka man h jaane do.” She would make angry faces whenever family members tried to stop her from roaming purposelessly. She would refuse food whenever asked about her changing behavior, gradually over time in next 2 weeks her irritability and anger increased, even on small matters. In between these episodes the client would sometime remain sad for whole day and refuse food. This pattern of irritability, anger, loss of appetite, decreased sleep, abnormal talks continued for next 3 weeks, after which she was brought to IGMC- OPD and admitted in psychiatry ward. IV. HISTORY OF PAST ILLNESS: Past medical history: There is no past history of diabetes, hypertension, or any other medical condition. Past Surgical history: Patients does not have any history of surgical procedure done on her like appendectomy etc. Allergy: Not known Obstetric history: Information not available. V. FAMILY HISTORY OF ILLNESS: History of medical illness in family: There is no significant history of chronic illness in family like asthma, hypertension, or any hereditary disease. Surgery history: Patient’s family is not having history of any surgery like appendectomy, etc. Psychiatric history: There is history of psychiatric illness in mother, was on medication but no document are available. Alcohol/ drug dependence/ suicidal ideation: History of substance use- Tobacco, smoking in father.
- 6. FAMILY TREE: Jay Dev, 50 year, Male 8th pass Santosh Kumari, 47 year, Female No formal education Mukesh Bisht, 30 year, Male 10+2, Farmer Chander Rekha 26 year, Female Graduation Sunny Chauhan, 24 year, Male BA, LLB Hazel 11/2 year, Fch KEY USED: Male Female Patient on whom case is presented
- 7. SOCIO-ECONOMIC STATUS: Type of family: Nuclear family Income per month: 15,000 per annum VI. PERSONAL HISTORY: a) Prenatal history: 1. Antenatal period: Registered or not : Immunization : Antenatal checkups : Diet during pregnancy : Family environment : Wanted child or not : 2. Intranatal period: Delivery Birth Birth cry Birth defect APGAR score Breast feeding 3. Postnatal complications: In mother: No significant evidence available. Accurate information cannot be inquired. PPH (Post partum hemorrhage) Puerperal sepsis
- 8. In baby: Cyanosis Convulsions Jaundice Respiratory distress syndromes Any genetic defect b.) Infancy and early childhood (birth through age 3) Middle childhood (3 years- 11 years) Pre- school and school experience Play history: Relationship with playmates: No significant evidence available. Accurate information cannot be acquired. No significant evidence available. Accurate information cannot be inquired. Lochia Involution of uterus Anemia Postnatal depression Postnatal psychosis Bonding with child Late childhood (adolescent 12- 19 years) Emotional problems during adolescence : Puberty: Age at appearance of secondary sexual characteristics :
- 9. d Occupational history Activities/ household chores Attitude towards work Relationship with family members e) Premorbid personality Interpersonal relationship : Trusting Family & social relationships : Client was ambitious, adjustable, independent Use of leisure time/ Hobbies/ Interest : Dancing, Singing Usual reaction to stressful events : Adjustable and flexible Attitude to self and others : Works in harmony and had a good attitude towards self and others. Attitude to work & responsibilities : Welcomes responsibility, flexible, determined Religious beliefs & moral attitudes : Normal Fantasy life : Day dreaming was absent Anxiety related to puberty changes : Behavior and emotional problem )Young adulthood (19- 24 years) : No significant evidence available. Accurate information cannot be inquired.
- 10. Eating pattern : Client is vegetarian Bowel and bladder habit : Regular bowel Sleep : Good sleeping pattern before the illness (as said by the attendant.) Use of drugs, tobacco, alcohol : Client has no history of substance use. PROBLEMS IDENTIFIED: - Patient is having disturbed sleeping pattern. - Reduced food intake. - Self -initiation is absent. VII. MENTAL STATUS EXAMINATION GENERAL APPEARANCE AND BEHAVIOUR Appearance : looks apparent to her age Facial expression : Anxious, no facial expression change as evidenced on conversating with the client Level of grooming : Normal (Hair combed, brushed teeth and bathing done every day) Level of cleanliness : Adequate Level of consciousness : Fully consciousness Mode of entry : On OPD basis, by her family Co-cooperativeness : Cooperative (client performs activities on request or when asked to do so) Eye to eye contact : Maintained Psychomotor activity : Normal
- 11. Rapport : Only when conversating with others or asked by others/ self- initiation is not present Gesturing : Normal as evidenced when conversating with the client Posturing : Normal; attains comfortable position to self as observed when conversating with client Other movement : Normal INFERENCE: - In general appearance and behavior patient looks apparent to her age, level grooming is normal, and having adequate cleanliness and fully conscious, psychomotor activity, gesturing, posturing is normal but facial expression patient looks anxious, and not much change in facial expression is seen while conversating with the client, mode of entry was on OPD basis, brought in by her family members. Overall attitude of patient was co-operative, rapport established easily, eye- to- eye contact was maintained. MOTOR DISTURBANCE: OVERACTIVITY OR HYPERACTIVITY: patient was nor overactive neither hyperactive. She was involved in activities like prayer, playing games etc. when asked to do so. INFERENCE: overactivity is not present as evidenced by observation of the client during prayer and lunch. UNDERACTIVITY OR MOTOR RETARDATION: client does not show any underactivity or motor retardation. Patient didn’t show any sign of motor retardation, patient carrying her daily activities with normal way. INFERENCE: underactivity is not present as evidenced by observation of the client during prayer and lunch STUPOR: patient did not show any progressive and severe retardation and is not motionless. Patient was fully conscious and kept on changing position during interaction. INFERENCE: stupor is absent. STEREOTYPE: patient does not show constant repetition of speech, movements, nor was involved in writing a particular words phrase by own. INFERENCE: stereotype is absent. COMPULSIVE MOVEMENTS OR COMPULSION: patient did not have compulsive movements or repeated activities like hand washing, checking locks etc. INFERENCE: compulsion is not present as evidenced by observing the behavior of client during exercise and prayer ECHOPREXIA: patient did not have any pathological repetition by imitation of the movements of another person
- 12. INFERENCE: echopraxia is absent. NEGATIVISM: Patient was cooperative. She didn’t refuse any simple requests without apparent reasons. She obeyed my commands, as I said can I talk with you for sometime, patient accepted my request and maintained a conversation. INFERENCE: negativism is absent. AUTOMATIC OBEDIENCE: Automatic obedience was not present in the patient, as evidenced by patient did not show a pathological degree of compliance. INFERENCE: automatic obedience is absent. THERE ARE THREE ASPECTS OF DISORDER: Disorder of form of thought Disorder of content of thought Disorder in rate of speech DISORDER OF FORM OF THOUGHT a) CIRCUMSTATIALITY: patient was not including unnecessary details and explanations while giving answer to my question. Student nurse: Chander Rekha g, kese ho aap? Patient: Thik hun! Student nurse: Aaj apka mn kesa h? Patient: Mn thik h. INFERENCE: No circumstantiality was present as evidenced by conversation with patient. b) TANGENTIAL THINKING: patient did not give unnecessary detail and explanation and reached at the goal finally. Student nurse: Apne gaon k baare m btayenge? Patient: Mera gaon kuthari h, mei wahn ki rehne wali hun. Mere gaon k log ache h, mere aspass k log bhi ache h. mujhe apne gaon mei rehna bahot acha lgta h. INFERENCE: No tangential thinking was present as evidenced by conversation with patient. c) INCOHERENCE: patient’s speech was cleared and sense can be extracted from her speech. INFERENCE: No incoherence was present in patient as evidenced by above conversation with patient.
- 13. d) IRRELEVANT: patient was giving appropriately reply to questions being asked. No irrelevant talks were present. INFERENCE: No irrelevant talk was present in the patients speech as evidenced by conversation with client. e) NEOLOGISM: patient did not coin or invented own language and words which has special meaning to the patient. INFERENCE: neologism was not present in the patient evidenced by above conversation. a) Word salad Word salad and preservation was not present as observed during conversation b) Persevation Student nurse: Apne subh nashte mei kya khaya? Patient: Dudh, daliya, bread. INFERENCE: Persevation was not present in the patient as she was giving correct answer to asked question as evidenced by conversation with her. f) Ambivalence and ambivalence ideas Student nurse: Chander Rekha ji, apko kesa lag rha h? Patient: Thik hun INFERENCE: Ambivalence was not present as enquired during conversation with the patient, the attendants information, and doctors notes. EVALUATION OF SPEECH a) Intensity: Patient’s voice was normally audible as observed during conversation with patient.50-70 (decibels) but have to go a little closer to the client to hear clearly and appropriately. b) Pitch: Her voice is monotonous, she showing no variation in her speech as evidenced during conversation with the client. c) Speed: Rate of speech was slowed as evidenced by conversations with patient. (responding only to the asked question if she feels to respond) d) Spontaneous: Patient respond after a 5- 8 sec gap of when question was put to her as evident by conversation with her e) Manner: Patient’s manner is relaxed evident by conversation f) Reaction time: Reaction time of patient is increased as observed during the time of conversation with her.
- 14. DISORDER OF THE CONTENT OF THOUGHT a. Delusion i. Persecutory Delusion Student nurse: Chander Rekha ji, kya apko pka vishwaas h ki koi apko marna chahta h ya nuksaan pohchana chahta h? Patient: Nahi, esa toh kuch nhi h. Inference: Persecutory delusion was not present as evidenced by conversation with the patient. ii. Delusion of reference Student nurse: kya aapko aisa pka vishwaas hai ki aapke aas- paas k log hmesha aapke bare me hee baat krrhe hain ? Patient: Nhi, esa kyun hoga? Inference: Delusion of reference is not present as enquired during conversation with patient iii. Delusion of influence or passivity Student nurse: Kya aapko aisaa pka vishwaas hai ki jo aap bolrhe ho yakr rhe ho wo koi or aapse krwa rha hai? Patient: Nhi ji Inference: Delusion of influence / passivity was not present in patient as evidenced by enquiring during conversation with patient. iv. Delusion of sin and guilt Student nurse: kya apko pkaa vishwaas h ki jo kuch b galat ho rha h usme apki glti h? Patient: Nahi esa kuch b nhi h. Inference: Delusion of sin and guilt was not present in patient as enquired by asking question during conversation and on confirming with the attendant. v. Hypochondrical delusion Student nurse: Kya apko pka vishwaas h ki apko koi bohot badi bimari ho gyi hai jiski wajh se apko baar baar doctor k pass jana pdta h? Patient: Nhi Inference: Hypochondrial delusion was not present as inquired during conversation with client, family members. vi. Delusion of grandeur
- 15. Student nurse: Kya apko pka vishwaas h ki aap ek mahan insan ho or apme bohot si shaktiyaan h? Patient: Nhi. Inference: Delusion of grandeur was not present as evidenced by conversation with patient and on attendents information, doctors notes. vii. Nihlistic delusion Student nurse: kya apka pkaa vishwaas h ki apke aas paas ki saari cheezeisn khtm ho chuki hain ya khtm ho rhi h? Patient: Nahi, esa kuch nhi h Inference: Nihlistic delusion was not present as evidenced by on inquiring with the client, doctors notes, information given by the attendant. Derealization: Derealization not present in patient as evident by conversation with patient. Student nurse: Kya apka pka vishwas h ki apke aas- pass ki duniya badl gayi h ya nasht ho chuki h? Patient: Esa kyun hoga Inference: Derealization not present in the patient. Depersonalization: Depersonalization was not present in patient as evident during conversation. Student nurse: Kya apka pka vishwas h ki apke shareer ka koi ang nsht ho chuka h? Patient: Nhi esa nhi h ,pr paer m drd h. Inference: Depersonalization not present in the patient as per conversation and observation done. viii. Disorders of the possession of thought or control of thinking: Thought alienation Student nurse: Kya apko esa lgta h ki koi apke dimaag se khayal nikalata hai? Patient: Nhi Inference: Thought alienation not present in client as inquired by the client and on viewing the doctors notes. Thought insertion Student nurse: Kya apko esa lgta h ki koi apke dimaag mei khayal dalta h jo apke mn se na aye ho? Patient: Nhi, esa kyun hoga.
- 16. Inference: Thought insertion not present in the client as inquired during the conversation, and information received by the attendant. Thought deprivation (withdrawal) Student nurse: Kya apko esa lgta h ki koi apke dimag se khayal nikal leta h? Patient: Nahi Inference: Thought deprivation not present in the client as inquired by the client and doctors notes. Thought broadcasting Student nurse: Kya apko esa lgta h ki apke vichar or khayal apke bina btaye sbko pta lg jaten h? Patient: Nahi Inference: Thought broadcasting not present in patient as evidenced by doctors notes, information given by attendants and on inquiring the client. b. Obsession Student nurse: kya apke mn mei ek hi vichar baar- baar aaten h jiski vjh se aap kisi aur cheez pr dhyan nhi de pate? Patient: Nhi Inference: Obsession not present in client as seen after inquiring with the client and doctors’ notes in the file. c. Compulsion Student nurse: kya apke mnn mei ek hi kaam karne ka khayal baar-baar aata h? Patient: Nhi Inference: Compulsion was not present in the client as inquired during conversation and on observing the clients daily routine. d. Phobias Student nurse: kya apko bina kisi spsht karn ke kisi cheez se dar lgta hai? Patient: Nhi, dar toh nhi lgta. Inference: Phobia was not present in the client as inquired during conversation and on observing the clients daily routine.
- 17. e. Phantasy/fantasy Student nurse: yahan se jane k baad aap kya karoge? Patient: Kuch ni, ghr jake apni beti ka dhyan rakhungi.. Inference: Phantasy was not present in the patient as evidenced after inquiring with the client. i. Creative: Creative thinking was not present as enquired during conversation. ii. Day dreaming: Day dreaming was not present in patient as enquired during conversation. D) DISORDER OF RATE OF SPEECH a. Pressure of speech: Pressure of speech was normal as evidenced by conversation with patient. b. Flight of idea: Flight of idea was not present in patient as evidenced by conversation with patient. c. Retardation: Slowness in speech was absent as evidenced during conversation with patient. d. Mutism: Mutism was not present in patient as evident during conversation. e. Aphonia: Aphonia was not present as evident during conversation. f. Thought Block: Thought block was not present as evident during conversation. g. Clang association: Clang association was not present as evidenced during conversation with patient. E) DISORDER OF PERCEPTION a. Illusion Student nurse: Wo kya h (pointing towards exhaust fan) Patient: Pankha h Inference: Illusion was not present in patient as inquired by the client and observed the client activity. b. Hallucination
- 18. i. Auditory hallucination Student nurse: Kya jb aap akele hote ho tbh apko koi awazein sunayi deti h, aur apke aas paas koi ni hota? Patient: Nhi, esa kuch nhi sunai deta. Inference: Auditory hallucination was not present in patient as inquired during conversation and observed her activity. ii. Visual hallucination Student nurse: jb aap akele hote ho or apke aas- paas koi nhi hota to apko kuch dikhayi toh nhi deta jo asal m wahan maujud nhi hota? Patient: Nhi, esa kuch nhi h. Inference: Visual hallucinations were not present as inquired during the conversation and on observing the client and information taken from the attendant. iii. Olfactory hallucination Student nurse: Kya apko apnea as- pass se alag trh ki smell ati h jo kisi aur ko na aa rhi ho? Patient: Nhi Inference: Olfactory hallucination was not present as inquired from the client. iv. Gustatory hallucination Student nurse: Kya apko es alga ho ki jb aap khana kha rhe ho to khane ka swaad bdl rha ho ya sb khane se ek hi swaad aa rha ho? Patient: Nhi Inference: Gustatory hallucination was not present in the client as inquired during the conversation. v. Tactile hallucination Student nurse: Kya apko kbhi es alga ho ki apke sharer pr keede raing rhe h? Patient: Nhi, esa kuch nhi h Inference: Tactile hallucination was not present in the patient as inquired during conversation and no evidence present in doctors notes. vi. Hypnogogic hallucination Student nurse: jb aap sone lgte ho kya apko koi awaazein sunayi ya kuch dikhayi deta h?
- 19. Patient: Nhi, kuch b ni Inference: Hypnogogic hallucination was absent in the client as evidenced by inquiring the client and as per the information gathered through the attendant’s and doctors’ notes. vii. Hypnopepnic hallucination Student nurse: Kya jb aap soo k uthte ho toh apko koi awazen sunai deti h aur apke ass pass koi na ho? Patient: Nhi Inference: Hypnopepnic hallucination was absent in the client as evidenced through inquiring during conversation and as per doctors notes. viii. Lilliputian hallucination Student nurse: kya apko apke samne rakhi cheezien kbhi bohot hi choti dikh rhi ho ya apse duur ja rhi ho? Patient: Nhi Inference: Lilliputian hallucination not present in the patient as inquired during the conversation. ix. Kinesthetic hallucination Student nurse: Apko kbhi aisa lga ki shreer ka koi hissa, mood gya ho, ya apke shreer k hisse m koi hlchl ho rhi ho? Patient: Nhi aisaa nhi lgta. Inference: Kinesthetic hallucination was not present as inquired during conversation. x. Macropsia Student nurse: Kya apko kbhi esa laga ki apke samne rkhi cheez ya koi insaan bada ho gya h? Patient: Nhi Inference: It was not present as inquired during conversation. xi. Micropsia Student nurse: kya apko kbhi ais alga ki apke samne rkhi cheez, aakar m chota ho gya h?
- 20. Patient: Nhi Inference: Micropsia was not present in the client as inquired during conversation and doctors notes. F) DISTURBANCE IN AFFECT a. Inappropriate or incongruent affect The facial expression of the client was appropriate, not having incongruent affect. b. Pleasurable affect i. Euphoria Student nurse: apka mn abhi kesa h? Patient: Thik h. Inference: Euphoria was not present in the client as inquired during the conversation, and on observing the client’s daily activity, doctors notes. ii. Elation: Elation, exaltation, ecstacy was not present in patient as evidenced by above conversation iii. Exaltation: Exaltation and ecstacy was not present in patient as evidenced by above Conversation and by observing patient’s behavior. iv. Ecstacy c. Unpleasurable affect i. Depression – Depression was present in patient as evidenced by observation and inquired during conversation, the information gathered through the patients file and doctors notes. Student nurse: aj apka mn kesa h? Patient: Thik h Student nurse: mn m kese vichar aate h? Patient: mn m toh filhal kuch bhi vichar nahi h. Apni beti ko padhana likhana chahti hun. Jisse ki vo apne paon pr khade ho sake. Jb purani baaten yaad ati h toh marne k bhi vichar aate h. mene ekbaar marne ki koshish bhi ki thi, apne sasural mei, phir baache ka khayal aya, devi- devta ka khayal aya toh 2-3 dawayi ki patiyan toh pani m dho rakhi thi, wo aadha hi piya, baki fek di. Iske baad toh lagta h ki apne baccho k liye hi jeena chahiye.
- 21. Inference: Client was worried about her relationship with her husband, and seemed worried about her child and had ideas of self harm as per above conversation, information gathered from her father and as per the patients file ii. Grief or mourning – Not present in patient as evidenced by above conversation. d. Other affect i. Anxiety Student nurse: Kya apko bina kisi spsht karn ke choti si baat pe ghabrahat hoti h? Patient: Nhi Inference: Anxiety was not present in the patient as evidenced by conversation with patient. ii. Fear Student nurse: Kya apko kisi cheez se dar lgta h? Patient: Nhi Inference: Fear was not seen in patient. iii. Agitation: Patient was not agitated at the time of conversation. iv. Panic: Patient was not panic as observed during conversation. v. Free floating anxiety Student nurse: kya apko bina kisi karn k dar lgta h? Patient: Nhi Inference: Free floating anxiety not present in the client as per inquired during conversation, doctors notes, information gathered from attendant. vi. Apathy: Not present in patient. vii. Aggression: Aggression was absent in patient. viii. Mood swings: Mood swing was not present in patient. ix. Emotional liability: Emotional liability not present in the patient.
- 22. G) DISORDER OF MEMORY Memory a. Immediate memory Student nurse: main aapko abhi 5 cheezon k naam btaungi. 5 minute k baad aapse puchungi aapko jitna yaad hoga aap bol k bta skte ho ya agr likhna chaho to aap likh bhi skte ho. Pen, Scale, chappal, chashma, notebook. After 5 minute student nurse: Mainne aapko 5cheezon k naam btaaye the kya aap mujhe bta skte ho? Patient: Pen, scale, chappal, chasma, notebook Inference: Immediate memory was intact as enquired by asking question. b. Recent memory Student nurse: Chander Rekha ji aapne kl dinner me kya khaya tha? Patient: Dal, chappati, sbji Student nurse: Dal konsi thi? Patient: Rajma Inference: Recent memory was intact to some extent as enquired by asking question. c. Remote memory Student nurse: aap bta skte ho ki aapka janam din kb aata hai? Patient: 15 july Inference: Remote memory of patient was completely intact as confirmed with patient’s file. i. Amnesia Student nurse: aap ko apne bachapan k dosto k nam yad ha? Patient: Priyanka, Chandni Inference: Amnesia was not present as inquired and cross- checked with patient’s file. ii. Paramnesia Student nurse: aapki padaie kaha tak hue ha? Patient: Mene graduation kri h, uske baad shadi ho gyi
- 23. Inference: Patient not having paramnesia as evidenced after inquiring the client as cross- checked with patient’s file. iii. Anterograde amnesia (patient is able to recall the recent event) Student nurse: aapko hospital me aaye huye kitne din ho gye? Patient: hafta ho gya h Inference: Anterograde amnesia was not present in patient as inquired and confirmed from the attendant. iv. Retrograde amnesia: (patient is able to recall past event) Student nurse: Kya apko apne bchpn ke doston k naam yaad h? Patient: Nhi. Inference: Though the client was not able to remember the name of her childhood friends, the client is not having retrograde amnesia as per inquired during the conversation. v. Déjà vu Student Nurse: kya aapko kbhi aisaa lgta ya aisaa mehsoos hota hai ki jo aapke sath ho rha hai wo pehle bhi ho chuka hai ? Patient: Nhi esa kuch nahi h? Inferences: Déjà vu was not present in patient as evidenced by inquiring after conversation. vi. Jamaes vu Student nurse: Saapko kbhi aisaa lgta hai ki jinko pehle se jante ho, ya jo aapki life me pehle ho chukka hai wo pehli baar ho rha hai ? Patient: Nhi Inferences: Jamaes vu was not present in patient as inquired during conversation, patients file. vii. Hypermnesia Student nurse: aapko apane bachapan ki koe ghatana yad ho? Patient: Yaad ni Inferences: Hypersomnia was not present in patient as enquired by asking question. Orientation a. Time Student nurse: abhi kya time hua hai (pointing toward clock)?
- 24. Patient: 11 bj gye honge Student nurse: aaj kaun see taarik hai? Patient: 3 march Student nurse: abhi kaun sa maheena chl rha hai? Patient: march. Student nurse: abhi kaun sa saal chl rha hai ? Patient: 2023 Student nurse: kya aap bta skte ho kaun sa mosum chl rha hai ? Patient: grmiyan ane wali h Inferences: Patient completely oriented to time as evidenced after inquiring through conversation. b. Place Student nurse: ky aapko pta h aap abhi kahaan pr ho? Patient: Shimla Student nurse: kya aap bta skte ho ki baahr mausam kaisa hai ? Patient: Dhoop lagi h. Inferences: Patient was oriented to place. c. Person Student nurse: nmste m kon hun kya apko yaad h? Patient: Shivani Student nurse: aapke samne jo khade ha vo kon ha( pointing toward the father) Patient: Mere father h. Inferences: Patient was oriented to person. Insight Student nurse: aap hospital kis wajah se aaye ho? Patient: Pehle bhi ese bimar thi tbh bhi Hospital ayi thi. Student nurse: Aap apni bimari k bare me jante ho?
- 25. Patient: Choti choti baton p ghussa aajata tha, dwai bhi lena bnd kr liya tha Inferences: Insight (Grade 5 i.e., intellectual insight) ATTENTION & CONCENTRATION: CONCENTRATION: - Student nurse: abhi mai apko kuch number dungi, apko unhe minus karna hai 100-7 kitne hote hai? Patient: 93 Student nurse: 93-7 to kitne bchte h? Patient: 86 Student nurse: 86- 7 to kitne bchte h? Patient: 79 Inferences: Patient concentration is good. Student nurse: kya aap mujhe mahino k nam bata sokte ho, jiase January ,February Patient: January, February, March, April, May, June, July Inference: Client concentration is normally sustained. ATTENTION: Student nurse: me kuch bolugi aap phir aap bhi vasa hi repeat karna ? Patient: Thik h Series forward Student nurse Patient 1 Pen, scale, chappal pen, scale, chappal Student nurse: ab jasa me bolugi vase hi aapne use ulta bolana ha Patient: Thik ha ji Start karen Series backward student nurse patient 10-9-8-7-6-5 5- 6-7-8-9-10 Inference: Attention is present as evidence doing backward and forward counting client is able to do so.
- 26. Abstract thinking Student nurse: kya aap bta skte ho ball or orange me kya smanta hai ? Patient: Dono gol h Student nurse: kya aap bta skte ho ball or santre me kya frk hai? Patient: Santra khane k liye hota h. Proverb testing: nach na jane aagan tedha ka kya mtlb hota h? Patient: Inference: Abstract thinking is normal. Personal Student nurse: yhan se jane k baad aap kya kroge ? Patient: Ghr jaungi. Social Student nurse: jab aap kahi ghumane phiarane jaooge ya apni beti k sath jaooge to kase kapade pahan kar jaooge? Patient: tayar hoti hun, aur apni beti ko b tyar krungi Student nurse: agr aapko raaste me letter mil jata hai jo sealed h, jiss pr pta likha ho to aap kya kroge? Patient: Agr m pta janti hun toh unko de dungi Student nurse: agar aapko khana bnate bnate cut lag jaye to aap kaya karoge? Patient: Pani se saaf. Inferences: Patient judgement was good as evidenced by asking question during conversation. Intelligence Student nurse: hmare desh k pradhanmantri kaun hain? Patient: Sh. Narender Modi g Student nurse: Himachal ki rajdhani kya hai?
- 27. Patient: Shimla Student nurse: Aapke jila ka kaya nam ha? Patient: Solan Inference: Intelligence of patient is average as evidenced by asking question, doctors notes. Sleep a) Observe pattern of sleep i. Temporary insomnia Student nurse: jb aap sonne lgtte ho to neend aane me kitna samay lg jata hai? Patient: Pta nhi khane k baad so jati hun. Inference: Temporary insomnia was present as evidenced by attendents information and cross- checking the file. ii. Persistent insomnia Student nurse: hospital me aane se pehle bhi aapko neend aane me samay lg jata tha? Patient: Hmm.. (non- verbal response), on inquiring with the patient. Inferences: Persistent insomnia not present in the patient. iii. Temporary hypersomnia: Not present iv. Persistent hypersomnia: Not present v. Non organic sleep wake cycle disturbances Student nurse: kya aap raat ko neend se baar bar jagte ho? Patient: Hmm.. kabhi- kabhi Inference: There is slight disturbance in patient’s sleep wake cycle. E.M.A: Early morning awakening Student nurse: aap subah kitne bje uthte hain? Patient: 5 bje tk uth jati hun
- 28. Inference: Early morning awakening was present as confirmed by night duty staff and attendents. b) Episodic disturbances Any attack or fit of i. Epilepsy Any attack of epilepsy, hysterical, impulsive, destructive ii. Hysterical was not present in patient as confirmed by on duty staff, ward iii. Impulsive attendant and observed behavior during my shift. iv. Aggressive Client often gets angry on small things. v. Destructive PROBLEM IDENTIFIED AFTER MENTAL STATUS EXAMINATION Client is in mixed state of bipolar affective disorder. Replies to asked questions only. No initiation of talk or any activity. Has reduced appetite. Has decreased sleep. NEUROLOGICAL EXAMINATION A. Level of Consciousness B. Mental Status Examination C. Special cerebral functions Agnosia : absent in the patient i.e. lack of ability to identify people or objects. Patient is able to identify his attendants and objects. Aproxia : absent Aphasia : absent in the patient i.e. inability to communicate Optic nerve: Inspection of eye Visual acquity : Normal Visual field examination: Normal Color vision : Normal
- 29. Oculomotor trochlear and abducent nerves Pupillary reaction to light : Normal Pupillary size : Normal Eye movement in six direction: Normally done Nystagmus : Absent Diplopia : Absent Trigeminal nerve: Corneal reflex : Present Facial sensory response : Present Mandibular strength : Present/Normal Facial nerve: Facial expression : Appropriate to conversation Taste sensation : Normal Vestibulo cochlear nerve: Auditory acquity test : Normal Glossopharyngeal and Vagus nerve: Gag reflex : Present Swallowing reflex : Present Position and movement of uvula and palate : Normal Sensation of taste : Normal Spinal accessory nerve: Sternocleidomastoid muscle strength : A little weak but normal according to age Elevation of shoulder : Normal
- 30. Turning of head : Normal MOTOR FUNCTION ASSESSMENT Muscle size : normal Muscle strength : normal Muscle tone : normal Muscle co-ordination : present Gait : normal Gait : Normal Movement of all the joints: normal Deformities: Absent Abnormal movement : Absent SENSORY FUNCTION ASSESSMENT Pain sensation : Present Temperature sensation : Present Touch sensation : Present Vibration sensation : Present ASSESSMENT OF CEREBELLAR FUNCTION Finger to finger test : Normally done Finger to nose test : Normally done Romberg test : Not possible to assess in client Tandem walking test : Not assessible ASSESSMENT OF REFLEXES Superficial reflexes : Not assessed Deep tendon reflexes : Not assessed
- 31. Biceps : Not able to assess Triceps : Not able to assess Brachioradial : Not able to assessed Patellar : Not assessed Achilles : Not assessed Any abnormal reflexes : Absent PROBLEM IDENTIFIED IN PHYSICAL EXAMINATION AND NEUROLOGICAL EXAMINATION No such deformity or physical disturbances are present in the client but sometimes complains of stomachache the reason being as a occurrence of somatic symptoms in relation to the present psychiatric illness. No such medical condition has been ruled out for her stomachache .
- 32. MINI- MENTAL STATUS EXAMINATION S.NO. CONTENT POINTS PATIENT SCORE 1. ORIENTATION (Total Score= 10) What is the year? Season? Date? Day? Month? Which is our state? Country? Town or City? Hospital? Floor? (10) 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 2. ATTENTION AND CALCULATION (Total Score= 5) Spell “world” backwards D L R O W Ask to count backwards from 100 in blocks of 7 100-7= 93 93- 7= 86 86-7= 79 79- 7= 72 72- 7= 65 (5) 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
- 33. 3. REGISTRATION (Total Score=3) Name three objects - apple - table - pen Ask the patient to repeat the names of all three objects Repeat the objects names until all three are learned (3) 1 1 1 1 1 1 4. RECALL (Total Score= 3) Ask to repeat the three objects - apple - table - pen (3) 1 1 1 1 1 1 5. LANGUAGE (Total Score= 7) Point to any object and ask to name the object Do the same again with a different object Ask the patient to repeat any proverb. “No ‘ifs and/ or ‘buts’” Allow only one trial Give patient a blank paper and ask to follow a three-stage command Take a paper in your right hand Fold it in half Put it on the floor Write “CLOSE YOUR EYES” and show it to the patient. Ask him or her to read the message and do what it says. (7) 1 1 1 1 1 1 1 1 1 1 1 1 1 1
- 34. Ask the patient to write a sentence of their choice on a blank piece of paper, sentence should make sense. Show the patient a drawing of two pentagons which intersect to form a quadrangle. Ask to copy the design exactly as it is. 1 1 1 1 TOTAL SCORE 30 30 DESCRIPTION OF THE CASE BIPOLAR AFFECTIVE DISORDER Bipolar disorder, formerly manic depression, is a mental disorder with periods of depression and periods of elevated mood. The elevated mood is significant and is known as mania or hypomania, depending on its severity, or whether symptoms of psychosis are present. During mania an individual behaves or feels abnormally energetic, happy or irritable. During periods of depression there may be crying, a negative outlook on life, and poor eye contact with others.
- 35. DEFINITION: Affective disorders are characterized by a sever disturbance of mood manifested as elation or excitement and depression. These are accompanied by one or both of the following: - Delusions Perplexity (a form of confusion in which the patient is bewildered and uncertain about his thoughts) Disturbed attitude towards self Disorder of perception and behavior These symptoms appear according to the mood of the patient. In DSM III these disorders include major affective disorders (manic episodes, major depressive episode, bipolar disorders). So it can be defined as- “affective disorders are illness in which mood change is primary and dominant feature. Mood change is relatively persistent and is associated with characteristics changes in thinking, attitude and behavior. INCIDENCE :- the incidence of bipolar disorder is roughly equal, with a ratio of women to men of about 1.2 to 1. The average age of onset for bipolar disorder is the early twenties, and following the first manic episode, the disorder tends to be recurrent. As with depression, bipolar disorder appears to be more common in unmarried than in married person. COURSE: Bipolar mood disorder has an earlier age of onset (third decade) than recurrent depressive (uni polar) disorder. Unipolar depression, on the other hand, is common in two age groups: late third decade and fifth to sixth decades. An average manic episode lasts for 3-4 months while a depressive episode lasts from 4-6 months. Unipolar depression usually lastslonger than bipolar depression. With rapid institution of treatment, the major symptoms of mania are controlled within 2 weeks and of depression within 6-8 weeks. CLASSIFICATIONAcc. To ICD 10- F31.0 Bipolar affective disorder current episode mania F31.1 Bipolar affective disorder current episode mania without psychotic symptom F31.2 Bipolar affective disorder current episode mania with psychotic symptom F31.3 Bipolar affective disorder current episode mild or moderate depression
- 36. F31.4 Bipolar affective disorder current episode severe depression without psychotic symptoms. F31.5 Bipolar affective disorder current episode Severe depression with psychotic symptoms. Acc. To DSM IV – Bipolar 1 Bipolar 11 ETIOLOGICAL FACTORS: BOOK PICTURE PATIENT PICTURE Genetic predisposition: - There is increasing evidence that genetic plays a strong role in predisposition. Approximately 15% of the brothers, sisters, parents and children of BPAD were also suffering from these ailments. Not present Neurophysiological factors: - Researchers have found the possibility that imbalance in excitatory and inhibitory processes may predispose BPAD. Present Biochemical factors: - findings reveal the possibility of metabolic changes in the brain pathology with these disorders, particularly the catecholamine imbalance. Increased or decreased catecholamine may cause mania or depression respectively. Present Psychological or interpersonal / predisposing family and personality factors: - Mood swings in the parents will leads to maladaptive learning in the children. These children may develop a typical premorbid personality pattern. Not present Severe stress: - Patients who have experienced severe stress in their life-time may be more prone. present
- 37. PHYSIOLOGICAL INFLUENCES Right-sided lesions in the limbic system, temporo- basal areas, basal ganglia, and thalamus have been show to induce secondary mania. Magnetic resonance imaging studies have revealed enlarged third ventricles an subcortical white matter and periventricular hyperintensities in clients with bipolar disorder Not present TYPES OF BIPOLAR DISORDER BIPOLAR I DISORDER: - Bipolar I disorder is the diagnosis given to an individual who is experiencing, or has experienced, a full syndrome of manic or mixed symptoms. The client may also have experienced episodes of depression. This diagnosis is further specified by the current or most recent behavioral episode experienced. For example, the specifier might be “single manic episode” (to describe individuals having a first episode of mania). For individuals who have had recurrent mood episodes, the current (or most recent) episode may be identified as manic, hypomanic, mixed, or depressed. BIPOLAR II DISORDER: - The bipolar II disorder diagnostic category is characterized by recurrent bouts of major depression with episodic occurrence of hypomania. The individual who is assigned this diagnosis may present with symptoms (or history) of depression or hypomania. The client has never experienced an episode that meets the full criteria for mania or mixed symptomatology. OTHER BIPOLAR DISORDERS BIPOLAR DISORDER DUE TO A GENERAL MEDICAL CONDITION: This disorder is characterized by a prominent and persistent disturbance in mood that is judged to be the result of direct physiological effects of a general medical condition (American
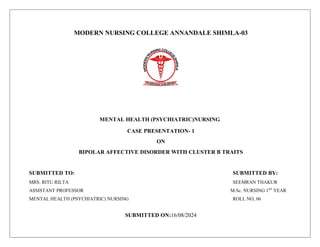
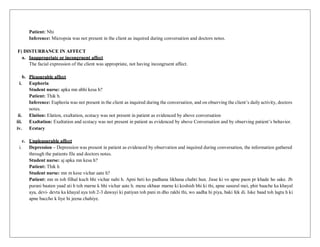
- 38. Psychiatric Association [APA], 2000). The mood disturbance may involve de- pression or elevated, expansive, or irritable mood, and causes clinically significant distress or impairment in social, occupational, or other important areas of functioning. Types of physiological influences are included in the discussion of etiological implications for bipolar disorders. SUBSTANCE-INDUCED BIPOLAR DISORDER: The disturbance of mood associated with this disorder is considered to be the direct result of physiological effects of a substance (e.g., a drug of abuse, a medication, or toxin exposure). The mood disturbance may involve depression or elevated, expansive, or irritable mood, and causes clinically significant distress or impairment in social, occupational, or other important areas of functioning Mood disturbances are associated with intoxication from substances such as alcohol, amphetamines, cocaine, hallucinogens, inhalants, opioids, phencyclidine, sedatives, hypnotics, and anxiolytics CLINICAL MANIFESTATION MANIC PHASE DEPRESSIVE PHASE Expensive, grandiose, or hyperirritable mood √ Low self esteem - Increased psychomotor activity such as agitation pacingor hand wringing - Overwhelming inertia - Excessive social extroversion - Feeling of Hopelessness, Apathy, self reproach - Rapid speech with frequent topic changes - Difficulty concentrating, intellectualimpairment - Decreased need for sleep and food √ Psychomotor Retardation - Impulsivity - Anhedonia - Impaired judgement - Suicidal Ideation √
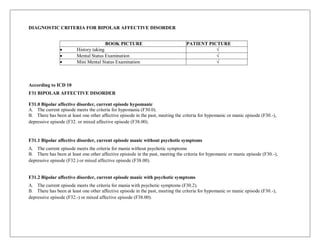
- 39. DIAGNOSTIC CRITERIA FOR BIPOLAR AFFECTIVE DISORDER BOOK PICTURE PATIENT PICTURE History taking √ Mental Status Examination √ Mini Mental Status Examination √ According to ICD 10 F31 BIPOLAR AFFECTIVE DISORDER F31.0 Bipolar affective disorder, current episode hypomanic A. The current episode meets the criteria for hypomania (F30.0). B. There has been at least one other affective episode in the past, meeting the criteria for hypomanic or manic episode (F30.-), depressive episode (F32. or mixed affective episode (F38.00). F31.1 Bipolar affective disorder, current episode manic without psychotic symptoms A. The current episode meets the criteria for mania without psychotic symptoms B. There has been at least one other affective episiode in the past, meeting the criteria for hypomanic or manic episode (F30.-), depressive episode (F32.) or mixed affective episode (F38.00). F31.2 Bipolar affective disorder, current episode manic with psychotic symptoms A. The current episode meets the criteria for mania with psychotic symptoms (F30.2). B. There has been at least one other affective episode in the past, meeting the criteria for hypomanic or manic episode (F30.-), depressive episode (F32.-) or mixed affective episode (F38.00).
- 40. F31.3 Bipolar affective disorder, current episode moderate or mild depression A. The current episode meets the criteria for a depressive episode of either mild (F32.0) or moderate severity (F32.1). B. There has been at least one other affective episode in the past, meeting the criteria for hypomanic or manic episode (F30.-), ormixed affective episode (F38.00). F31.4 Bipolar affective disorder, current episode severe depression without psychotic symptoms A. The current episode meets the criteria for a severe depressive episode without psychotic symptoms (F32.2). B. There has been at least one well authenticated hypomanic or manic episode (F30.-) or mixed affective episode (F38.00) in the past. F31.5 Bipolar affective disorder, current episode severe depression with psychotic symptoms A. The current episode meets the criteria for a severe depressive episode with psychotic symptoms (F32.3) B. There has been at least one well authenticated hypomanic or manic episode (F30.-) or mixed affective episode (F38.00) in the past. F31.6 Bipolar affective disorder, current episode mixed A. The current episode is characterized by either a mixture or a rapid alternation (i.e. within a few hours) of hypomanic, manic and depressive symptoms. B. Both manic and depressive symptoms must be prominent most of the time during a period of at least two weeks. C. There has been at least one well authenticated hypomanic or manic episode (F30.-), depressive (F32.-) or mixed affective episode (F38.00) in the past. My client is suffering from F31.6 Bipolar affective disorder, current episode mixed with cluster B- traits
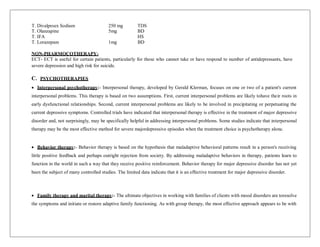
- 41. MANAGEMENT: TREATMENT MODALITIES: - The specific goals of treatment are to decrease the frequency, severity & psychosocialconsequences of episodes & to improve psychosocial functioning between episodes. A. Psychiatric Management: - The general goals of management are to assess & treat acute exacerbation prevent recurrence improve inter episode functioning &provide assistance, insight & support to patient & family. The specific goals of psychiatric management include establishing & maintaining a therapeutic alliances, monitoring the patient’s psychiatric status, providing education regarding their illness, prognosis & treatment, enhancing treatment compliance. Promoting regular patterns of activity & wakefulness, promoting understanding of an adaptaion to the psychosocial effects of bipolar disorder, identifying new episodes early & reducing the morbidity & sequelae of bipolar disorder. B. Pharmacological Treatment:- Three mood stabilizer currently available are lithium, valproate & carbamazepine; lithium has been the primary pharmacological treatment of patient with bipolar disorder. The combination of cabamazepine & lithium may be particularly effective for some patients, although it appears to increase their riskof developing an acute, confusional state -T. lithium: 900 – 2100mg/day -Carbamazepine: 600 – 1800 mg/day -Sodium Valproate: 600 -2600 mg/day -Clonazepam. In My Patient:-
- 42. T. Divalproex Sodium T. Olanzapine 250 mg 5mg TDS BD T. IFA HS T. Lorazepam 1mg BD NON-PHARMOCOTHERAPY- ECT- ECT is useful for certain patients, particularly for those who cannot take or have respond to number of antidepressants, have severe depression and high risk for suicide. C. PSYCHOTHERAPIES Interpersonal psychotherapy:- Interpersonal therapy, developed by Gerald Klerman, focuses on one or two of a patient's current interpersonal problems. This therapy is based on two assumptions. First, current interpersonal problems are likely tohave their roots in early dysfunctional relationships. Second, current interpersonal problems are likely to be involved in precipitating or perpetuating the current depressive symptoms. Controlled trials have indicated that interpersonal therapy is effective in the treatment of major depressive disorder and, not surprisingly, may be specifically helpful in addressing interpersonal problems. Some studies indicate that interpersonal therapy may be the most effective method for severe majordepressive episodes when the treatment choice is psychotherapy alone. Behavior therapy:- Behavior therapy is based on the hypothesis that maladaptive behavioral patterns result in a person's receiving little positive feedback and perhaps outright rejection from society. By addressing maladaptive behaviors in therapy, patients learn to function in the world in such a way that they receive positive reinforcement. Behavior therapy for major depressive disorder has not yet been the subject of many controlled studies. The limited data indicate that it is an effective treatment for major depressive disorder. Family therapy and marital therapy:- The ultimate objectives in working with families of clients with mood disorders are toresolve the symptoms and initiate or restore adaptive family functioning. As with group therapy, the most effective approach appears to be with
- 43. a combination of psychotherapeutic and pharmacotherapeutic treatments. Some studies with bipolar disorder have shown that behavioral family treatment combined with medication substantially reduces relapse rate compared with medication therapy alone. Group therapy:- Once an acute phase of the illness is passed, groups can provide an atmosphere in which individuals may discuss issues in their lives that cause, maintain, or arise out of having a serious affective disorder. The element of peer supportmay provide a feeling of security as troublesome or embarrassing issues are discussed and resolved. Some groups have other specific purposes, such as helping to monitor medication-related issues or serving as an avenue for promoting education relatedto the affective disorder and its treatment. Cognitive behavior therapy:- In cognitive therapy, the individual is taught to control thought distortions that are considered to be a factor in the development and maintenance of mood disorders. In the cognitive model, depression is characterized by atriad of negative distortions related to expectations of the environment, self, and future. The environment and activities withinit are viewed as unsatisfying, the self is unrealistically devalued, and the future is perceived as hopeless. Supportive psychotherapy Psychodynamic psychotherapy.
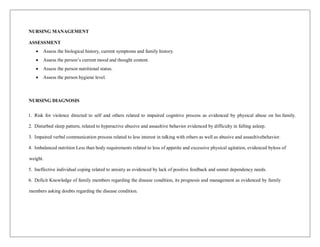
- 44. NURSING MANAGEMENT ASSESSMENT Assess the biological history, current symptoms and family history. Assess the person’s current mood and thought content. Assess the person nutritional status. Assess the person hygiene level. NURSING DIAGNOSIS 1. Risk for violence directed to self and others related to impaired cognitive process as evidenced by physical abuse on his family. 2. Disturbed sleep pattern, related to hyperactive abusive and assaultive behavior evidenced by difficulty in falling asleep. 3. Impaired verbal communication process related to less interest in talking with others as well as abusive and assaultivebehavior. 4. Imbalanced nutrition Less than body requirements related to loss of appetite and excessive physical agitation, evidenced byloss of weight. 5. Ineffective individual coping related to anxiety as evidenced by lack of positive feedback and unmet dependency needs. 6. Deficit Knowledge of family members regarding the disease condition, its prognosis and management as evidenced by family members asking doubts regarding the disease condition.
- 45. NURSING DIAGNOSIS ASSESSMENT NURSING DIAGNOSIS GOAL PLANNING IMPLEMENTATION RATIONALE EVALUATION Subjectivedata: Clients says that she use to feel anger and gets irritated easily and is having self harming behaviour. Objective data: Her father said that she gets irritable on smallest of matter and have previously attempted to harm self. Risk for violence directed to self and others related to impaired cognitive process as evidenced by physical abuse on his family. Short-Term Goal: Client will not harm self or others during hospitalization. Long-Term Goal: Agitation and hyperactivity will be maintained by administrationof tranquilizing medication. -Assess the client’srisk for harming self. -Closely monitor the client’s behavior. -ensure that all sharp objects, glass or mirrored Items, belts, ties, have been removed from clientenvironment. -redirect violent behavior with physical outlets. -offer transquilizing medication as per treating physician’s prescription. -Assessed the client’slevel of anger and the reason for anger which isat risk for harming others. -Closely monitored the client for any violent behaviors like hurting others and the using abusive language. -Ensured that all sharp objects, glass or mirrored items, belts, ties,smoking materials have been removed from client’s environment. -Involved client in exercise and other activities like relaxationand diversion therapy. -Administered Tab lorazepam wheneverthe patient got agitated as prescribed by physician. -To preventing the client and the otherfamily members from getting injury. -To Risk for hurting family is being reduced by monitoring client. -To Prevent the client injury whichcan also leads to suicide. -To help in divertingthe mind and help the client for relaxation. -To help the clientfor controlling his aggressive behaviour when client got agitated Client remained free from the risk for violence directed to others.Her irritability andanger outburst is reduced to some extent.
- 46. ASSESSMENT NURSING DIAGNOSIS GOAL PLANNING IMPLEMENTATION RATIONALE EVALUATION Subjective data: Patient says, “She is feeling restlessness.’ Objective data: Her father said that she didn’t sleep properly at last night and client looks dull. Disturb sleep pattern, related to hyperactive abusive and assaultive behavior evidenced by difficulty in falling asleep. Short term goal: To provide adequate resting hours to the patient. Long term goal: Get adequate sleep at night -Assess the level of sleeping pattern of the client. -Planning daytime activities according to the patient’s interests. -Ensure a quiet and peaceful environment when the patient is preparing for sleep. -Do not allow the patient to sleep for long time during the day. -Assessed the sleeping pattern of the client. The client is not able to sleep he use to sleep for 1-2 hours in a day. -A time schedule was prepared for the patient. And in that schedule, some activities are given to the patient according to his interest like- drawing, playing games. -Provided him quiet and peaceful environment when he want to sleep by keeping distracting thing away from client like mobile phone. -Avoided his excessive day time sleep by engaging the client in doing some task like drawing and playing ludoo -To improve the sleeping pattern of the client. -To engaging the client in daily activities and diverting the mind as client gets frustrated and shows anger. -To help the client to have adequate resting time and sleeping hours when needed. -To help the client to engaged in some task which is provided to client which will avoid the clients day time sleep. The sleeping pattern of the client was improved as theclient is now taking adequate rest i.e upto 8 hours sleep. -Teach the family to give some hot drink to client. -Mother is taught to give hot drink to client like milk for drinking. Which can induce sleep. -To induce the sleep of the client.
- 48. ASSESSMENT NURSING DIAGNOSIS GOAL PLANNING IMPLEMENTATION RATIONALE EVALUATION Subjective data:- patient family member verbalize that patient is not taking food at proper time and adequately. Objective data:- I observed this by doing physical examination. Imbalanced nutrition Less than body requirements related to lack of appetite and excessive physical agitation, evidenced by loss of weight. Short-Term Goal: Client will consume sufficient foods and meal snacks to meet recommended daily allowances of nutrients. Long-Term Goal: Client will begin to regain weight and exhibit no signs or symptoms of malnutrition. -Consult dietitian to determine appropriate diet for Client to restore nutrition and gain weight. -Ensure that his diet includes foods that he particularly likes. -Maintain an accurate record of intake, output, and calorie count. Obtain daily weights. -Administer vitamin supplement, as ordered by physician. Sit with Client during mealtime -Diet chart of the patient was prepared by the nurse to improve the nutrition level and maintain the weight of the client. -Diet chart was prepared particularly according to patient likes and dislikes. -Recording and reporting of the client intake, output, and about calorie count is recorded timely. -Medicine like vitamin A and D supplement is given to the client to maintain vitamin level and during meal time checked the client for proper food and medicine. -To help the client to restore nutrition and gain weight. -To help the client to take food in time with interest. -To maintain and check the client input and output and to obtain calorie level and revised the diet plan for the client. -To help to increase the clients vitamin level. The client nutrition level is being maintainedto some extent and the clients weight is gained i.e. 54 previouslythat was 52.
- 49. PSYCHOEDUCATION SEMI- STRUCTURED SCHEDULE: A semi- structured schedule was given and explained to the client as well as the family members to be followed at home to maintain the routine day activities. MEDICATION: I advised patient to take medicine as prescribed by Psychiatrist. I also advised the patient to not skip any medicine and complete the course. Patient has been advised related to the safe use of medicine as per patient’s level of understanding. I advised the patient to report any side effect of medicine like constipation, GI upset, Nausea, photosensitivity etc. Patient has been advised to take plenty of water as patient was complaining for constipation and advised to take prescribed medication for constipation. I advised the patient related to the ill effect of medicine left in between the course. DIET: Unfortunately, there's no specific diet that's been proven to relieve depression. Still, while certain eating plans or foods may not ease symptoms or put client instantly in a better mood, a healthy diet may help as part of overall treatment. Antioxidants Prevent Cell Damage Beta-carotene: apricots, broccoli, cantaloupe, carrots, collards, peaches, pumpkin, spinach, sweet potato Vitamin C: blueberries, broccoli, grapefruit, kiwi, oranges, peppers, potatoes, strawberries, tomato Vitamin E: margarine, nuts and seeds, vegetable oils, wheat germ "Smart" Carbs Can Have a Calming Effect Carbohydrates are linked to the mood-boosting brain chemical, serotonin. Experts aren't sure, but carb cravings sometimes may be related to low serotonin activity. Limit sugary foods and opt for smart or “complex” carbs (such as whole grains) rather than simple carbs (such as cakes and cookies). Fruits, vegetables, and legumes also have healthy carbs and fiber. Protein-Rich Foods Boost Alertness Foods like turkey, tuna, and chicken have an amino acid called tryptophan, which may help you make serotonin. Try to eat something with protein several times a day, especially when you need to clear your mind and boost your energy. Good sources of healthy proteins include beans and peas, lean beef, low-fat cheese, fish, milk, poultry, soy products, and yogurt.
- 50. EXERCISES: Depression symptoms often improve with exercise. Regular exercise may help ease depression by: Releasing feel-good endorphins, natural cannabis-like brain chemicals (endogenous cannabinoids) and other natural brain chemicals that can enhance your sense of well-being Taking your mind off worries so you can get away from the cycle of negative thoughts that feed depression and anxiety Regular exercise has many psychological and emotional benefits, too. It can help: Gain confidence. Meeting exercise goals or challenges, even small ones, can boost your self-confidence. Getting in shape can also make you feel better about your appearance. Get more social interaction. Exercise and physical activity may give you the chance to meet or socialize with others. Just exchanging a friendly smile or greeting as you walk around your neighbourhood can help your mood. Cope in a healthy way. Doing something positive to manage depression is a healthy coping strategy. Trying to feel better by drinking alcohol, dwelling on how you feel, or hoping depression or anxiety will go away on its own can lead to worsening symptoms. Doing 30 minutes or more of exercise a day for three to five days a week may significantly improve depression symptoms. But smaller amounts of physical activity — as little as 10 to 15 minutes at a time — may make a difference. It may take less time exercising to improve mood when one does more-vigorous activities, such as running or bicycling. FOLLOW- UP: I advised the patient for the regular follow up after discharge. Patient has been Educated about the importance of regular follow up whenever she will be discharged. I advised the patient related to any symptom that may relapse after hospital discharge and advised her to come immediately to hospital if any relapsing symptom will reoccur. I gave her instruction and education related to her doctor in charge Dr. Ravi Sharma that she can any time contact to her doctor if any problem will occur after discharge. Information is provided to the family member about the OPD days of Dr. Ravi Sharma. I advised client’s family to look for the client patiently and closely observe her as there were chances for suicidal risk in the client. Prognosis: Improved (good prognosis). Social worker: Mrs. Payal Chauhan Voluntary organizations: Moksha, Sunrise Rebirth Foundation, New born foundation.
- 51. S.no. Drugs Dose Frequency Route Action Side- effects 1. Tab. Pan- D 40mg OD P/O Antacid Watery stools, Nausea or Vomiting, Unusual tiredness and weakness, Skin rash, Loss of appetite, Muscle pain, Dizziness 2. Tab. Olanzapine 5mg BD P/O Atypical antipsychotics Drowsiness, dizziness, lightheadedness, stomach upset, dry mouth, constipation, increased appetite, or weight gain Rarely cause a condition known as tardive dyskinesia develop unusual/uncontrolled movements (especially of the face, lips, mouth, tongue, arms or legs). For females, this increase in prolactin may result in unwanted breast milk, missed/stopped periods, or difficulty becoming pregnant. For males, it may result in decreased sexual ability, inability to produce sperm, or enlarged breasts. Serious side effects, including: difficulty swallowing, shaking (tremor), slow heartbeat, fainting, mental/mood changes (such as confusion, restlessness), numbness/tingling of arms/legs, yellowing eyes/skin, Severe stomach/abdominal pain, trouble urinating, interrupted breathing during sleep, blood sugar rise, which can cause or worsen diabetes, seizures, neuroleptic malignant syndrome (NMS) following symptoms: fever, muscle stiffness/pain/tenderness/weakness, severe tiredness, severe confusion, sweating, fast/irregular heartbeat, dark urine, signs of kidney problems (such as change in the amount of urine). Allergic reaction including: fever, swollen lymph nodes, rash, itching/swelling (especially of the face/tongue/throat), severe dizziness, trouble breathing.
- 52. 3. Tab. Diva- OD 250mg TDS P/O Anticonvulsant (or anti- epileptic) Headache, Dizziness, Blurred vision, Weakness, Abdominal pain, Infection, Nausea, Vomiting, Sleepiness, Hair loss, Weight gain, Double vision, Diarrhea, Tremors, Weight loss, Flu-like symptoms 4. Tab. Lorazepam 1mg BD P/O Benzodiazepin es Drowsiness, dizziness, tiredness, weakness, dry mouth, diarrhea, nausea, changes in appetite, restlessness or excitement, constipation, difficulty urinating, frequent urination, blurred vision 5. Tab. IFA - BD P/O Iron Supplement Constipation, diarrhea, stomach cramps, or upset stomach allergic reaction, including: rash, itching/swelling (especially of the face/tongue/throat), severe dizziness, trouble breathing.