






















































![■ This volume increase results in a change of tensile stresses to
compressive stresses generated around the tip of the crack.
■ The compressive forces counter the external tensile forces and
stop the further advancement of the crack.
■ This characteristic accounts for the material’s low susceptibility
to stress fatigue and high flexural strength of 900 Mpa to 1200
MPa.
60
Hauptmann H, Suttor D, Frank S, Hoescheler H. Material properties of all-ceramic zirconia prosthesis
[abstract]. J Dent Res. 2000;79(suppl 1):S507.](https://image.slidesharecdn.com/drsamia3-250126115611-89797ba9/85/Dr-Samia-fmh-3-2-17-Dental-Ceramics-pptx-60-320.jpg)
















Dr. Samia fmh 3.2.17 Dental Ceramics.pptx
- 1. DENTAL CERAMICS Dr. Samia Shafiq Postgraduate Resident (FCPS II) Department of Prosthodontics FMH College of Medicine and Dentistry, Lahore. February 3, 2017.
- 4. Ceramics Ceramic comes from the Greek term Keramos and means potter, referring to one’s ability to heat clay to form pottery. Mclaren EA, Cao PT. Ceramics in dentistry—part I: classes of materials. Inside Dentistry. 2009;5(9): 94-105. 4
- 6. Uses in Dentistry ■ Artificial Denture Teeth ■ Crowns, Bridges and Veneers ■ Ceramic Posts ■ Abutments ■ Implants 6
- 7. Porcelain ■ Porcelain is a ceramic consisting of a glass matrix phase and one or more crystalline phases (eg, leucite). ■ All porcelains are ceramics, but not all ceramics are porcelains. 7
- 8. Porcelain is said to have been invented by Marco Polo in the 13th century from the Italian word Porcellana, or cowrie shell. He used the cowrie shell to describe Chinese porcelain because it was similarly strong and hard while remaining thin and translucent. 8
- 9. Types of Porcelain Opaque Porcelain Masks the color of alloy Responsible for metal ceramic bond Body Porcelain Provides translucency Aids shade matching Incisal Porcelain Most Translucent Displays perceived color of restoration 9
- 10. Composition of High-, Medium-, and Low-Fusing Body Porcelains (Weight Percentage) CONSTITUENTS HIGH-FUSING MEDIUM- FUSING LOW-FUSING (VACUUM FIRED) METAL- CERAMIC SiO2 72.9 63.1 66.5 59.2 Al2O3 15.9 19.8 13.5 18.5 Na2O 1.68 2.0 4.2 4.8 K2O 9.8 7.9 7.1 11.8 B2O3 — 6.8 6.6 4.6 ZnO — 0.25 — 0.58 ZrO2 — — — 0.39 10 Modified from Yamada HN, Grenoble PB: Dental porcelain: the state of the art 1977. Los Angeles, University of Southern California School of Dentistry, 1977.
- 11. Sintering ■ Sintering is the consolidation process of ceramic powder particles through heating at high temperatures which results in atomic motion. ■ Sintering of porcelain promotes physical-chemical reactions responsible for the final properties of the ceramic products. ■ The amount of porosity decreases in the last stage of sintering. ■ The amount of porosity is mainly influenced by the sintering temperature, time, and viscosity of the melt. 11
- 12. Devitrification ■ It is the process of crystallization in a formerly crystal-free (amorphous) glass. ■ The term is derived from the Latin Vitreus, meaning glassy and transparent. 12
- 14. 14 Alexis Duchateau 1774 • First attempt to use ceramics for fabrication of denture teeth Charles H. Land 1887 • Fabrication of first ceramic crown and inlay with Platinum Foil Matrix Technique Dr. Abraham Weinstein Late 1950s • Introduction of porcelain-fused-to-metal crown Weinstein and Weinstein 1962 • Fabrication of PFM crown using Leucite-containing Porcelain Frit
- 15. McLean and Hughes 1965 • Resurgence of all-ceramic restorations with the addition of industrial aluminous porcelain(> 50%) to the feldspathic porcelain 1980s • The castable glass-ceramic crown system • “Shrink Free” (Cerastore, coores Biomedical) Ceramic Systems Late 1980s • Introduction of Heat-pressed Ceramic Fabrication Technique 15
- 16. 1990s • Introduction of Slip-casting Fabrication Method • Introduction of 100% polycrystalline substructure ceramics Dr. Andersson, Nobel Biocare™ Mid 1990s • Introduction of the first All-ceramic product with a CAD/CAM substructure 2006 • Lithium Disilicate became the second generation of materials to be used as hot press ceramic 16
- 18. 18 Classification Based on Composition Based on Processing Method Based on Fusing Temperature Based on Microstructure Based on Translucency Based on Fracture Resistance Based on Abrasiveness
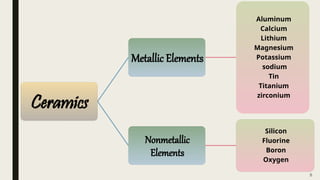
- 20. ■ Conventional dental ceramics are based on: – A Silica (SiO2) Network – Potash Feldspar (K2O-Al2O3-6SiO2) – Soda Feldspar (Na2O-Al2O3-6SiO2), or both.7 ■ Different elements are added to control the coefficient of thermal expansion, solubility, and fusing and sintering temperatures ■ These include: – Pigments (to produce the different hues) – Opacifiers (white-colored oxide to decrease translucency) – Glasses 20 Anusavice KJ. Phillips’ Science of Dental Materials.10th ed. Philadelphia, PA: WB Saunders; 1996.
- 21. ■ Ceramics can be divided into three categories by composition: 21 Ceramics Predominantly composed of Glass Consisting of Particle- filled Glass Consisting of Polycrystalline Aluminum Oxide Matrix Zirconium Oxide Matrix Fillers for Polycrystalline are not Particles but elements that alter optical properties. These added elements are referred to as Dopants. Kelly JR. Dental ceramics: what is this stuff anyway? J Am Dent Assoc. 2008;139(suppl):S4-S7.
- 22. 22
- 24. 24 Processi ng Methods Powder/Liquid Building Slip Casting Hot-ceramic Pressing Additive and Subtractive Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM)
- 25. Powder/Liquid Building ■ Conventional processing method ■ Incorporates building on a ceramic or metal core with a powder/liquid ceramic slurry with a brush or spatula by hand ■ The slurry is condensed by vibration to remove excess liquid, which rises to the surface and is blotted away by an absorbent tissue. 25
- 26. 26
- 27. 27
- 28. Common Reasons for Failure of Metal-Ceramic Restorations 28 Fracture during bisque bake • Inadequate condensation • Inadequate moisture control • Poor framework design • Incompatible metal-porcelain combination Bubbles • Too many firings • Air entrapment during buildup of restoration • Inadequate moisture control • Poor metal preparation • Poor casting technique
- 29. Unsatisfactory Appearance • Poor communication with technician • Inadequate tooth reduction • Excessive thickness of opaque porcelain • Excessive firing Clinical Fracture • Poor framework design • Centric stops too close to metal-ceramic interface • Inadequate metal preparation 29
- 30. Slip-casting ■ Introduced in the 1990s. ■ Restorations produced through this method tend to have fewer defects from processing and have greater strength than conventional feldspathic porcelain 30
- 31. 31 Processing Technique Creation of a porous core by slip casting (heated at 120°C for 2 hours) Core is sintered (1120°C for 10 hours) and then infiltrated with lanthanum-based glass( fire at 1100°C for 4 hours ) Producing two interpenetrating continuous networks: 1. A Glassy Phase 2. A Crystalline infrastructure.
- 32. 32
- 33. ■ The crystalline infrastructure could be: 1. Inceram Alumina (Al2O3) 2. Inceram Spinel (MgAl2O4) 3. Inceram Zirconia-alumina (12 Ce-TZP- Al2O3) ■ Flexural strength of inceram-zirconia is very high compared to the other slip casted ceramics. ■ However, these inceram-zirconia ceramics are highly opaque compared to others. 33 Denry I, Holloway JA. Ceramics for dental applications: a review. Materials. 2010;3(1):351-368.
- 34. Hot-Pressed Ceramic ■ Introduced in the late 1980s ■ Allows the dental technician to create the wax pattern. ■ Using the lost-wax technique, the technician is able to press a plasticized ceramic ingot into a heated investment mold. 34 Helvey GA. Classification of Dental Ceramics. Inside Dentistry 2013: 62-80
- 35. ■ Ceramics containing high amounts of Leucite Glass or optimal pressable ceramics were initially used for this process. ■ Lithium Disilicate became the second generation of materials to use this method in 2006. 35 Powers JM, Sakaguichi RL. Craig’s Restorative Dental Materials. 12th ed. St. Louis, MO: Mosby Elsevier; 2006:454.
- 36. 36
- 37. 37
- 38. CAD/CAM ■ Introduced in mid 1990s ■ The fabricated core consisted of 99.9% alumina on which a Feldspathic ceramic was layered ■ Two different CAD/CAM methods are used. – Additive Method – Subtractive Method 38
- 39. 39
- 40. Additive Method ■ This method is an additive version in which an electrodeposition of powdered material is applied layer by layer to a conductive die through an electrical current. ■ This technique is also referred to as rapid prototyping. 40 Beuer F, Schweiger J, Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. Br Dent J. 2008;204(9):505-11.
- 41. Subtractive Method ■ More common method ■ Using this method, a substructure or full-contour restoration is milled from a solid block of ceramic material. 41
- 42. ■ The available materials for the subtractive CAD/CAM processing include: – Silica-based Ceramics – Infiltration Ceramics – Lithium-disilicate Ceramics – Oxide High-performance Ceramics 42 Mclaren EA, Cao PT. Ceramics in dentistry—part I: classes of materials. Inside Dentistry. 2009;5(9): 94-105.
- 43. 43 Preoperative view of a gold crown requiring replacement as a result of secondary decay. The previous gold crown was digitally scanned before removal. The tooth was prepared, rescanned, and then a lithium-metasilicate restoration was milled.
- 44. 44 After finishing, external staining was applied. Postoperative view. Before the crown was cemented, it had been placed in a ceramic oven that reached a temperature of 850°C. At this temperature, crystallization of the ceramic occurs, resulting in a change of Lithium Metasilicate to Disilicate.
- 46. ■ The categories are described as: 1. High-fusing (1,300°C) 2. Medium-fusing (1,101°C to 1,300°C) 3. Low-fusing (850°C to 1,100°C) 4. Ultra-low-fusing (< 850°C) 46 Anusavice KJ. Phillips’ Science of Dental Materials. 10th ed. Philadelphia, PA: WB Saunders; 1996.
- 47. Clinical Application 47 Leinfelder KL. Porcelain esthetics for the 21st century. J Am Dent Assoc. 2000; 131(suppl 1): S47-S51. •Denture teeth High-fusing Porcelain •Crown and bridge Either Medium- or Low-fusing •Porcelain glazes Ultra-low-fusing Porcelain
- 50. Feldspathic or Leucite- reinforced Porcelain ■ Porcelains have two different phases: – Glass Phase (responsible for the Esthetics) – Crystalline Phase (associated with Mechanical Strength) ■ A crystalline mineral called Leucite (Potassium-aluminum-silicate) forms when Feldspar is incongruently melted between 1,150°C to 1,530°C. 50
- 51. ■ Incongruent melting is a process in which one material does not uniformly melt and forms a different material. ◙ ■ Leucite crystalline phase has a diffraction index similar to the glassy matrix that contributes to the overall esthetics of the porcelain. ◘ ■ Greater the Leucite content lesser the crack propagation will be. 51 ◙ Anusavice KJ. Phillips’ Science of Dental Materials. 10th ed. Philadelphia, PA: WB Saunders; 1996. ◘ Martinez Rus F, Pradies Ramiro G, Suarez Garcia MaJ, Rivera Gomez B. Dental ceramics: classification and selection criteria. RCOE. 2007;12(4):253-263.
- 52. ■ Hot-pressed ceramics have high amounts of leucite crystals and are considered leucite-reinforcedmglass ceramics. ■ Sintering process is avoided during the heated injection molding cycle, and the Leucite crystals act as barriers that counteract the increase in tensile stresses that can lead to the formation of microcracks. ■ This type of ceramic can be used to press as an all-ceramic restoration or to a metal coping. 52 Sorensen JA, Choi C, Fanuscu MI, Mito WT. IPS Empress crown system: three-year clinical trial results. J Calif Dent Assoc. 1998;26(2):130-6.
- 53. Aluminous Porcelain ■ Aluminous porcelain contains 40% to 50% Alumina crystals. ■ Alumina increases the strength of Feldspathic porcelain more than Leucite, which increases the fracture resistance( due to high elastic Modulus) 53 Kelly JR, Nishimura I, Campbell SD. Ceramics in dentistry: historical roots and current perspectives. J Prosth Dent. 1996;75(1):18-32.
- 54. 54 ■ The particle size of the alumina may be responsible for the increase in the mechanical properties by decreasing Agglomeration. ■ Finer powder yields a greater reduction in surface area when sintered. ■ Also, Fine powders tend to form clusters of irregular shape and uncontrolled size and are referred to as “agglomerates,” which hinder flow properties
- 55. Lithium Disilicate Reinforced Glass Ceramics ■ This ceramic material contains 70% lithium-disilicate crystals, resulting in an increased flexural strength of approximately 360 MPa (Milled version) to 400 MPa (Hot-pressed version). ■ The increase in strength is found in the unique microstructure of lithium disilicate, which consists of small interlocking platelike crystals that are randomly oriented. 55 Shenoy A, Shenoy N. Dental ceramics: an update. J Conserv Dent. 2010;13(4):195-203.
- 56. ■ Lithium disilicate is milled as Lithium Metasilicate and then heated to 820°C in a two-stage oven. ■ During this firing cycle, there is a controlled growth of the grain size (0.5 μm to 5 μm) and a conversion of Metasilicate crystals to Disilicate crystals. ■ Lithium-disilicate crystals cause cracks to deflect, branch, or blunt, which arrests the propagation of cracks. 56 Helvey GA. Chairside CAD/CAM: lithium disilicate restoration for anterior teeth made simple. Inside Dentistry. 2009; 5(10); 58-67.
- 57. Zirconia ■ Scientifically termed as Zirconia Dioxide. ■ Also known as “Ceramic Steel.” ■ Widely used in medicine and dentistry because of: – Mechanical Strength – Chemical and Dimensional Stability – Elastic Modulus similar to stainless steel 57 Piconi C, Maccauro G. Zirconia as a ceramic biomaterial. Biomaterials. 1999; 20(1): 1-25.
- 58. ■ A unique characteristic of zirconia is its ability to stop crack growth, which is termed “Transformation Toughening”. 58
- 59. ■ An ensuing crack generates tensile stresses that induce a change from a tetragonal configuration to a monoclinic configuration and a localized volume increase of 3% to 5% 59
- 60. ■ This volume increase results in a change of tensile stresses to compressive stresses generated around the tip of the crack. ■ The compressive forces counter the external tensile forces and stop the further advancement of the crack. ■ This characteristic accounts for the material’s low susceptibility to stress fatigue and high flexural strength of 900 Mpa to 1200 MPa. 60 Hauptmann H, Suttor D, Frank S, Hoescheler H. Material properties of all-ceramic zirconia prosthesis [abstract]. J Dent Res. 2000;79(suppl 1):S507.
- 61. 61
- 63. ■ There are several factors that affect the translucency of dental ceramics. ■ Thickness of the material has the greatest effect. ■ Translucency can also be affected by: – Number of firings, 41 – Shade of the substrate – Type of light source or illuminant.43, 63 Yu B, Lee YK. Color difference of all-ceramic materials by the change of illuminants. Am J Dent. 2009;22(2):73-8.
- 64. ■ Specimens should be compared at the recommended minimum thickness to be classified by translucency because clinical settings can vary so widely. ■ The greater the number of crystals in the glassy matrix, the less translucent the ceramic. 64 Unfilled Glassy Matrix (Feldspathic Porcelains) Zirconia Dioxide Translucen cy
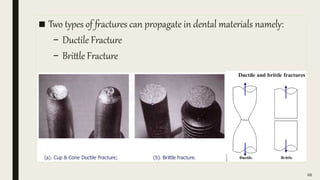
- 66. ■ Two types of fractures can propagate in dental materials namely: – Ductile Fracture – Brittle Fracture 66
- 67. Ductile Fracture ■ Most metals (not too cold). ■ Extensive plastic deformation ahead of crack ■ Crack is “stable”: resists further extension unless applied stress is increased 67
- 68. Brittle Fracture ■ Ceramics, ice, cold metals. ■ Relatively little plastic deformation ■ Crack is “unstable”: propagates rapidly without increase in applied stress 68
- 69. 69
- 70. ■ A material having a large value of fracture toughness will probably undergo ductile fracture ■ Brittle fracture is very characteristic of materials with a low fracture toughness value 70
- 71. 1 • YZ® Zirconia (Vident™) 2 • In-ceram® Zirconia (Vident) 3 • Procera® Alumina (Nobel Biocare) 4 • In-ceram Alumina (Vident) 5 • Lithium Disilicate 6 • In-ceram Spinell (Vident) 7 • Empress® 1 (Ivoclar Vivadent) 8 • Vita Omega 900 (Vita Zahnfabrik) 9 • Vita VM®9 (Vident) 10 • Conventional Feldspathic 71 Rekow ED, Silva NR, Coelbo PG, et al. Performance of dental ceramics. J Dent Res. 2011;90(8):937-952.
- 73. ■ The abrasiveness of a dental ceramic is mainly determined by the smoothness of the material.54 ■ Low-fusing porcelains were developed to incorporate finer-sized Leucite particles in lower concentrations to decrease the abrasiveness of the ceramic surface. 73
- 74. ■ Elmaria and colleagues compared the wear on opposing enamel by various restorative materials. ■ These included: 1. Gold, Glazed, and Polished Or Glazed-only Finesse® (Dentsply International) (A Low-leucite–containing ceramic) 2. Procera AllCeram™ (Nobel Biocare) 3. IPS Empress (Ivoclar Vivadent) 74 Elmaria A, Goldstein G, Vijayaraghavan T, et al. An evaluation of wear when enamel is opposed by various ceramic materials and gold. J Prosthet Dent. 2006; 96(5): 345-353.
- 75. ■ They found that gold, glazed-and-polished Finesse, and glazed- and-polished AllCeram were the least abrasive ■ Glazed-only IPS Empress was the most abrasive. 75
- 76. ■ Heintze and colleagues evaluated 20 in vitro studies in which a material and the antagonist wear of the same material were studied. ■ They found that the results were inconsistent, mainly because of the fact that the test parameters differed widely in: – Amount of force – Number of cycles – frequency of cycles – Number of specimens ■ They concluded, as far as consistency and correlation with clinical studies is concerned, the most appropriate method to evaluate a ceramic material with regards to antagonist wear is assessment of the unprepared enamel of molar cusps against glazed crowns. 76 Heintze SD, Cavalleri A, Forjanic M, et al. Wear of ceramic and antagonist-a systematic evaluation of influencing factors in vitro. Dent Mater. 2008;24 4):433-449.
- 77. 77 CONCLUSION
- 78. ■ There are a variety of ways to classify ceramic materials. ■ Classifications can change or new categories can be introduced as manufacturers continue to introduce new materials and formulations, ■ Clinicians should be cognizant of changes in material selection and continue to base their choices on the clinical needs of the patient in terms of esthetics and strength. 78
- 79. 79
- 80. 80