







































































Group 1 PRESENTATION SLIDES 2016 FINAL
- 1. A Faith-based Community Health Needs Assessment Leah Fahey, Shavena Fife, Katherin Rehn, Stephanie Richardson Catherine Wurtzler, Amy Zoglauer Thesis Advisor: Bonnie Beezhold, PhD, MHS, CHES
- 2. Introduction 1WHO, 2016; 2Merzel & D’Afflitti, 2003; 3Ockene et al, 2012 Socioecological Model
- 3. Introduction • Faith-based health promotion is an emerging strategy. • A place of worship is considered a trusted community source.1 1Harmon et al, 2014
- 4. Introduction • Needs assessments reveal major health and lifestyle issues.1 • Community members provide the best insight.2 – Behavioral Risk Factor Surveillance System Survey (BRFSS) 1Kumar & Preetha, 2012; 2Levy et al, 2004
- 5. Study Goal and Research Question • To conduct a faith-based community needs assessment in partnership with Gloria Dei Lutheran church in order to identify and prioritize the congregation's health needs. • What are the major health needs and corresponding health behaviors of the congregation?
- 6. Study Objectives • Primary: To investigate the associations of diet and health outcomes within the church community. • Secondary: To investigate the associations of health, diet, or lifestyle factors within the church community.
- 7. Study Design • Correlational, cross-sectional • Paper survey, physical measurements • Voluntary sample • Eligibility requirements: – Member of the Gloria Dei community – At least 19 years old – Willing and able to complete a survey
- 8. Survey • Extensive exploration into validated and reliable questions and questionnaires • BRFSS 2013 and 2014; other validated questions on exercise, diet, spirituality, drug use, end of life treatment • Diet questions – 5 A Day Consumption and Evaluation Tool (FACET) – Daily and weekly major foods (breakfast cereal, F&V, fish, etc.)
- 9. Survey Validity and Reliability Validity • Incorporated validated questions – BFRSS, FACET – Godin Leisure-Time Exercise Q • Pilot testing and feedback • Paper delivery only was utilized Reliability • Potentially unclear questions were slightly adapted • FACET – Cronbach’s alpha .59 • Godin Leisure-Time Exercise Questionnaire – 0.44 Cronbach’s alpha • Core Dimensions of Spirituality Questionnaire - Cronbach’s alpha 0.77
- 10. Physical Measurements • Non-invasive physical measurements – height, weight, waist circumference – Stadiometer - Seca 213 portable unit – Research grade scale – Precision Personal Health Scale Model UC 321PL – Cloth measuring tape
- 12. Recruitment Protocol • Info tables, announcements, flyers, emails, social media posts • Recruitment days • Incentives – Benedictine logo gear – pens, window stickers, cutting boards – Survey completion – entry into $100 Visa gift card drawing – Physical measurements – daily $10 or $20 restaurant gift card drawings • Data collection days
- 13. Survey Protocol • 15-20 minutes • Paper survey • Topics included – Demographics, health perceptions, health status, health behaviors • Variables of interest - diet and exercise variables • Reliability Clarified the script of this and the measurement protocol a bit.
- 14. Measurement Protocol • 5 minutes • Separate room with divider for privacy • Height, weight, waist circumference • Handout to participants • Reliability
- 15. Statistical Analysis • Correlational, differential • Parametric • Descriptive statistics • Multivariate analyses: Chi-square tests, Pearson and Spearman correlations, logistic regression • Univariate analyses: independent t-tests, ANOVA, ANCOVA • SPSS version 24; p values < 0.05 significant
- 17. Population characteristics Variables N Females n=101 Males n=56 Test Stat* p value* Mean ± SD Mean ± SD Age 157 59.41±15.00 57.86±14.21 t = 0.63 0.592 Ethnicity (White/other) 157 95 / 6 51 / 5 X2 = 0.14 0.707 Education (N/Y college degree) 157 22 / 79 9 / 47 X2 = 0.43 0.515 Marital status (N/Y married) 157 71 / 30 45 / 11 X2 = 1.40 0.236 Work status (N/Y) 157 49 / 52 24 / 32 X2 = 0.26 0.607 Total physical activity times/wk 149 36.37±25.64 41.23±28.28 t = -1.08 0.282 BMI 123 27.02±6.57 29.89±5.22 t = -2.53 0.013 *p < 0.05 indicates significance; independent samples t-tests or Chi-square tests for independence.
- 18. High School Graduate, 3.8%, n=6 Some college, 15.9%, n=25 College Graduate, 40.8%, n=64 Postgraduate, 39.5%, n=62 Education
- 19. Married, n=116, 73.9% Divorced, n=14, 8.9% Widowed, n=16, 10.2% Never married, n=8, 5.1% Member of unmarried couple, n=3, 1.9% Marital Status
- 20. Employed for wages, n=75, 48.1% Self employed, n=9, 5.8% Out of work < 1 year, n=1, 0.6% Homemaker, n=7, 4.5% Student, n=4, 2.6% Retired, n=58, 37.2% Unable to work, n=2, 1.3% Work Status
- 21. Disease conditions and risk indicators Diagnoses / risk indicators N Females Males p value* Count Count Cancer 154 17 12 0.683 Cardiovascular disease 153 4 5 0.390 Diabetes 156 19 13 0.613 Depression 154 17 8 0.788 Musculoskeletal disorders 155 45 21 0.428 Obesity (per BMI) 123 59 26 0.024* High cholesterol 155 37 26 0.282 High blood pressure 156 38 30 0.087 *p < 0.05 indicates significance. Chi-square test for independence.
- 22. Background: Musculoskeletal Disorders • Musculoskeletal Disorders (MDs) affect 50% of American adults over age 181; aging increases risk.2 • Certain diet and lifestyle factors adversely affect joint health –inflammatory diet,3 inactivity,4 and obesity.5 1US Bone and Joint Initiative, 2013;2Gheno et al, 2012 3Oliviero et al, 2015; 4Ciolac, 2016; 5Anandacoomarasamy, 2008
- 23. Methods • Has a doctor, nurse or other health professional EVER told you that you had some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia? –1=Yes –2=No –3=Don't know / Not sure • Question taken from BRFSS 2013 Questionnaire
- 24. N No MD n=89 Yes MD n=66 p value* Gender (count M/F) 56 / 99 35 / 54 21 / 45 0.4281 Age (mean ± SE) 155 54.48 ± 1.69 64.68 ± 1.32 <0.0012 Musculoskeletal disorders by gender and age *p < 0.05 indicates significance. 1Chi-square test for independence. 2Independent samples t-test; t (152) = 4.76, ƞ2 = 0.13.
- 25. Significant correlates with MD status *p < 0.05 indicates significance; Pearson product moment and Spearman rank order correlations. Variables N MDs (N/Y) r or rho / p value* Age 155 0.342 / 0.000 Red meat intake frequency/wk 154 0.253 / 0.002 Breakfast cereal intake frequency/day 145 0.198 / 0.017 Resistance exercise times/wk 152 -0.186 / 0.022 Days of poor physical health 155 0.167 / 0.037 Days of poor concentration related to physical health 153 -0.158 / 0.049
- 26. B ± SE p value* Odds ratio 95% CI Red meat intake intake frequency/wk 0.31 ± 0.10 0.002 1.36 (1.12, 1.66) Age 0.59 ± 0.15 0.000 1.06 (1.03, 1.09) Resistance exercise times/wk -0.23 ± 0.11 0.039 0.79 (0.64, 0.99) Multivariate analysis – Predictors of reporting musculoskeletal disorders *p < 0.05 indicates significance; logistic regression, final model explained 20.6-27.7% of the variance in MD status.
- 27. Comparison of significant correlates by MD status N No MD Yes MD p value* 95% CIs of Difference Mean ±SE Mean ±SE Age 155 54.48 ± 1.69 64.68 ± 1.32 0.000 (-14.43, -5.97) Red meat intake frequency/wk 154 2.20 ± 0.20 3.18 ± 0.23 0.0021 (0.38, 1.58) Resistance exercise times/wk 152 2.97 ± 0.21 2.28 ± 0.20 0.0222 (-1.27, -0.10) *p < 0.05 indicates significance; independent samples t-tests. 1ANCOVA; Adj means: 2.17 ± 0.20 vs 3.23 ± 0.24, p = 0.001, pƞ2 = 0.065. 2ANCOVA; Adj means: 2.30 ± 0.23 vs 2.95 ± 0.20, p = 0.042, pƞ2 = 0.028.
- 28. Discussion • More intake of meat and resistance exercise was related to diagnosis of MDs. • High meat consumption can be inflammatory if n-6/n-3 ratio is unbalanced.1,2 • Resistance exercise can strengthen bones, muscles, and joints, which helps prevent MDs.3,4 1Pattison, 2004; 2Patterson, 2012; 3Ciolac, 2016; 4Moreira, 2014
- 29. Background: Mental Health • Major depressive disorder affects 6.7% of all US adults; anxiety disorders affect 19.1% of US adults.1,2 • Evidence demonstrates link between diet and mood and significance of nutritionally inadequate diets.3,4 • Exercise is an effective treatment for depression.5 1NIMH, 2014; 2Harvard Medical School, 2007; 3Payne et al, 2012; 4Blumenthal et al, 2012; 5Sharma et al, 2006
- 30. Methods • During the past 30 days, for about how many days have you felt sad, blue or depressed? • During the past 30 days, for about how many days have you felt worried, tense or anxious? – 1=No days – 2=1 or 2 days – 3=3 or 4 days – 4=5 or 6 days – 5=About a week – 6=A couple of weeks – 7=Most of the month – 8=Every day – 9=Don't know / Not sure • Questions taken from BRFSS 2014 Questionnaire
- 31. N Sadness No d/mo n=71 Sadness 1-2 d/mo n=50 Sadness 3+ d/mo n=33 p value* Gender (count M/F) 55 / 99 30 / 41 13 / 37 12 / 21 0.1841 Age (mean ± SE) 154 61.82 ± 1.74 56.32 ± 2.23 56.18 ± 2.21 0.0682 Sadness days by gender and age *p < 0.05 indicates significance. 1Chi-square test for independence. 2ANOVA.
- 32. Anxiety days by gender and age *p < 0.05 indicates significance. 1Chi-square test for independence. 2ANOVA; F = 8.43, ƞ2 = 0.14. N Anxiety No d/mo n=40 Anxiety 1-2 d/mo n=41 Anxiety 3-6 d/mo n=37 Anxiety >6 d/mo n=38 p value* Gender (count M/F) 56 / 100 20 / 20 10 / 31 12 / 25 14 / 24 0.1101 Age (mean ± SE) 156 62.63 ± 2.26 65.29 ± 1.91 51.76 ± 2.55 54.66 ± 2.11 <0.0012
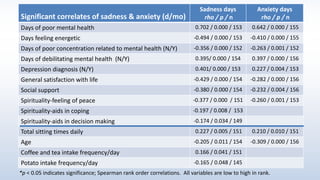
- 33. Significant correlates of sadness & anxiety (d/mo) Sadness days rho / p / n Anxiety days rho / p / n Days of poor mental health 0.702 / 0.000 / 153 0.642 / 0.000 / 155 Days feeling energetic -0.494 / 0.000 / 153 -0.410 / 0.000 / 155 Days of poor concentration related to mental health (N/Y) -0.356 / 0.000 / 152 -0.263 / 0.001 / 152 Days of debilitating mental health (N/Y) 0.395/ 0.000 / 154 0.397 / 0.000 / 156 Depression diagnosis (N/Y) 0.401/ 0.000 / 153 0.227 / 0.004 / 153 General satisfaction with life -0.429 / 0.000 / 154 -0.282 / 0.000 / 156 Social support -0.380 / 0.000 / 154 -0.232 / 0.004 / 156 Spirituality-feeling of peace -0.377 / 0.000 / 151 -0.260 / 0.001 / 153 Spirituality-aids in coping -0.197 / 0.008 / 153 Spirituality-aids in decision making -0.174 / 0.034 / 149 Total sitting times daily 0.227 / 0.005 / 151 0.210 / 0.010 / 151 Age -0.205 / 0.011 / 154 -0.309 / 0.000 / 156 Coffee and tea intake frequency/day 0.166 / 0.041 / 151 Potato intake frequency/day -0.165 / 0.048 / 145 *p < 0.05 indicates significance; Spearman rank order correlations. All variables are low to high in rank.
- 34. B ± SE p value* Odds ratio 95% CI SADNESS days Spirituality-aids in decision making 1.25 ± 0.55 0.023 3.47 (1.19, 10.18) Total sitting times daily 0.24 ± 0.10 0.017 1.28 (1.05, 1.56) ANXIETY days Depression diagnosis (N/Y) 1.08 ± 0.51 0.034 2.94 (1.09, 7.95) Total sitting times daily 0.25 ± 0.11 0.021 1.28 (1.04, 1.58) Age -0.05 ± 0.01 0.000 0.95 (0.93, 0.98) Multivariate analysis– Predictors of days of sadness and anxiety *p < 0.05 indicates significance; logistic regressions, final sadness days model explained 8.1-10.8% of the variance in sadness status, final anxiety days model explained 19.9-26.5% of the variance in anxiety status.
- 35. Comparison of sitting times daily by sadness and anxiety status N SADNESS No days/mo n=71 SADNESS 1+ d/mo n=83 p value* N ANXIETY 0-2 d/mo n=81 ANXIETY 3+ d/mo n=75 p value* Less than 4 h sitting/d 50 41.4% 25.9% 0.067 51 45.6% 20.8% <0.0011 5-8 h sitting/d 57 37.1% 38.3% 56 38.0% 36.1 % More than 8 h sitting/d 44 21.4% 35.8% 44 16.5% 43.1 % *p < 0.05 indicates significance. 1 Chi-square tests for independence; X2 (2, n = 151) = 16.01, phi = 0.326.
- 36. Discussion • Reliance on spirituality was strongest predictor of fewer days of sadness. Sitting less was predictor of fewer days of sadness and anxiety. • Social isolation may explain link between faith and sadness.1,2 • Sedentary behavior is a category separate from physical activity that affects both metabolic and mental health.3,4 1Croezen et al, 2015; 2 Miller et al, 2014; 3Chomistek et al, 2013; 4Teychenne et al, 2010
- 37. Background: Obesity • Obesity epidemic – more than one-third (36.5%) of American adults are obese.1 • Excess weight increases risk for developing major disease conditions.1 • Strong relationship between an increased BMI and coronary artery disease.2 1CDC, 2016; 2Labounty et al, 2013
- 38. Methods
- 39. BMI N=123 Normal weight n=44 Overweight n=43 Obese n=36 p value* Gender (count M/F) 77 / 46 38 / 6 23 / 20 16 / 20 0.0001 Age (mean ± SE) 59.34 ± 2.19 60.56 ± 2.45 55.53 ± 2.47 0.3212 BMI and WC risk categories by gender and age *p < 0.05 indicates significance. 1Chi-square test for independence; X2 (2, n = 123) = 17.21, phi = 0.37. 2ANOVA Waist circumference N=123 Lower risk n=63 Higher risk n=60 p value* Gender (count M/F) 46 / 77 20 / 43 26 / 34 <0.001* Age – Males (mean ± SE) 58.61 ± 1.90 58.69 ± 4.92 0.986 Age – Females (mean ± SE) 60.67 ± 5.04 57.95 ± 2.38 0.769 *p < 0.05 indicates significance; independent samples t-tests; t (121) = -6.57, ƞ2 = 0.000. check
- 40. Variables N BMI r or rho / p value* Waist circumference 122 0.854 / 0.000 Perception of general health 123 -0.380 / 0.000 Diabetes diagnosis (N/Y) 122 0.296 / 0.001 High blood pressure diagnosis (N/Y) 122 0.294 / 0.001 Gender (M/F) 123 0.285 / 0.001 Days of pain affecting activities 119 0.215 / 0.019 Sugary drink intake frequency/day 117 0.201 / 0.030 High cholesterol (N/Y) 121 0.201 / 0.027 Days feeling energetic 122 -0.195 / 0.031 Work status (N/Y) 122 0.187 / 0.039 Days of debilitating mental health 123 0.186 / 0.039 *p < 0.05 indicates significance; Pearson product moment and Spearman rank order correlations. All variables are low to high in rank. Significant correlates with BMI
- 41. Variables Males Females N r or rho / p value* N r or rho / p value* BMI 46 0.868 / 0.000 76 0.869 / 0.000 Diabetes diagnosis (N/Y) 77 0.452 / 0.000 High cholesterol (N/Y) 45 0.393 / 0.008 Health professional visits 77 0.374 / 0.001 Perception of general health 77 -0.344 / 0.002 Days of poor concentration related to physical health 46 0.318 / 0.031 Days of pain affecting activities 73 0.299 / 0.010 Musculoskeletal disorders diagnosis (N/Y) 75 0.271 / 0.019 Days of debilitating mental health 77 0.271 / 0.017 Significant correlates with WC *p < 0.05 indicates significance; Pearson product moment and Spearman rank order correlations. All variables are low to high in rank.
- 42. Variables Males Females N r / p value* N r / p value* Veg-based meals frequency/wk 45 -0.423 / 0.004 Dark green leafy vegs frequency/day 37 -0.387 / 0.012 Sugary drink intake frequency/day 43 0.323 / 0.035 Breakfast cereal intake frequency/day 43 -0.318 / 0.038 Omega-3 fish frequency/wk 76 0.255 / 0.026 Significant diet correlates with WC *p < 0.05 indicates significance; Pearson product moment correlation coefficients.
- 43. Variables B ± SE p value* Odds ratio 95% CI High blood pressure diagnosis (N/Y) 1.81 ± 0.48 0.000 6.11 (2.37, 15.75) Work status (N/Y) 1.57 ± 0.49 0.001 4.79 (1.83, 12.57) Multivariate analysis – Predictors of obesity *p < 0.05 indicates significance; logistic regression, final model explained 17-24% of variance in BMI.
- 44. Discussion • Predictors of obesity (per BMI) were high blood pressure and being employed. • Diet correlates of a risky WC in males were intake of fewer vegetables and more sugary drinks. • Sitting time at work positively correlated with obesity.1 • Increased intake of sugary drinks related to increased BMI and WC.2, 3 • Vegetable-based diet related to smaller WC.4 1Chau et al, 2011; 2Malik et al, 2013; 3Odegaard et al, 2012; 4Rizzo et al, 2011
- 45. Background: Pain • Pain is a result of inflammation.1‚2 • 100 million Americans experience pain³; complication of chronic disease.² • Lifestyle factors can influence pain.⁴-⁶ ¹Dept of Pain Medicine & Palliative Care ; ²PubMed Health; ³American Academy of Pain Medicine; ⁴Van Hecke, 2013; ⁵Goldberg, 2007; ⁶John, 2006
- 46. Methods • During the past 30 days, for about how many days did pain make it hard for you to do your usual activities, such as self-care, work or recreation? – 1 = No days – 2 = 1 or 2 days – 3 = 3 or 4 days – 4 = 5 or 6 days – 5 = About a week – 6 = A couple of weeks – 7 = Most of the month – 8 = Every day – 9 = Don’t know / Not sure • Question taken from BRFSS 2014 Questionnaire
- 47. Pain by gender and age N No Pain n=106 Pain ≥ 1 d/mo n=46 p value* Gender (count M/F) 56 / 96 36 / 70 20 / 26 0.350¹ Age (mean ± SE) 152 58.82 ± 1.45 57.63 ± 2.11 0.648² *p < 0.05 indicates significance. ¹Chi-square test for independence. ²Independent samples t-test; t (152) = 0.458, ƞ2 = 0.001.
- 48. Significant correlates with pain status Variables N Pain (low to high) rho / p value* Days of poor physical health 152 0.455 / 0.000 Days of debilitating physical health 152 0.385 / 0.000 Perception of general health 152 -0.357 / 0.000 Days feeling energetic 151 -0.321 / 0.000 BMI 119 0.215 / 0.019 Waist circumference 119 0.215 / 0.019 Sugary drink intake frequency/day 144 0.200 / 0.016 High blood pressure diagnosis (N/Y) 151 0.194 / 0.017 Days of debilitating mental health 152 0.182 / 0.025 Diabetes diagnosis (N/Y) 151 0.162 / 0.047 *p < 0.05 indicates significance; Spearman rank order correlations. All variables are low to high in rank.
- 49. B ± SE p value* Odds ratio 95% CI BMI 0.81 ± 0.04 0.027 1.08 (1.01, 1.17) Multivariate analysis - Predictors of reporting pain *p < 0.05 indicates significance; logistic regression, final model explained 4.1- 5.9% of the variance in pain status. Reminder: this model only explains at most 6% of the variance in BMI
- 50. Comparison of BMI by pain status N No Pain n=106 Pain n=46 p value* 95% CIs of difference Mean ± SE Mean ± SE BMI 119 26.99 ± 0.58 29.56 ± 1.00 0.023¹ (-4.79, -0.36) *p < 0.05 indicates significance. ¹Independent samples t-test; t (119) = -2.298 , ƞ2 = 0.04.
- 51. Discussion • BMI predicted the likelihood of reporting pain. • Increasing BMI can cause excess weight > pressure on joints > inflammation > pain.¹-³ • High BMI and physical inactivity are associated with chronic pain.⁴ Modest weight reductions decrease pain.⁵ ¹NIDDK, 2012; ²Zdziarski, 2015; ³Nijuis, 2009; ⁴ Nilsen, 2011; ⁵Anandacoomarasamy, 2008
- 52. Background: Sleep • 30% of adults are reporting an average of <6 hours of sleep.1 • Sleep restriction increases risk for cardiovascular diseases and diabetes.2 • National Institutes of Health suggests that adults get 7-8 hours of sleep a night.1 1CDC, 2016; 2Jackson, 2015 Image reference: https://www.cdc.gov/features/dssleep/
- 53. Methods • On average, how many hours of sleep do you get in a 24-hour period? – 4 or less hours – 5-6 hours – 7-8 hours –9-10 hours –More than 10 hours –Don’t know/Not sure • Question taken from BRFSS 2014 Questionnaire
- 54. Hours of sleep by gender and age N Sleeps 5-6 hrs n=57 Sleeps ≥7 hrs n=100 p value* Gender (count M/F) 56 / 101 25 / 32 31 / 69 0.1491 Age (mean ± SE) 157 54.68 ± 2.39 61.23 ± 1.46 0.0072 *p < 0.05 indicates significance. 1Chi-square test for independence. 2Independent samples t-test; t (157) = 2.09, ƞ2 = -0.13.
- 55. Significant correlates with sleep hrs/night Variables N Sleep hrs/night rho / p value* Work status (N/Y employed) 157 -0.307/0.000 Age 157 0.229 / 0.004 Coffee and tea intake frequency/day 154 -0.194 / 0.016 BMI 124 -0.160 / 0.077 Fish intake frequency/wk 154 0.159 / 0.049 Sugary drink intake frequency/day 148 -0.059 / 0.472 *p < 0.05 indicates significance; Spearman rank order correlations.
- 56. B ± SE p value* Odds ratio 95% CI Fish intake frequency/wk 0.38 ± 0.19 0.042 1.47 (1.01, 2.12) Coffee and tea intake frequency/day -0.26 ± 0.10 0.013 0.77 (0.63, 0.95) Multivariate analysis – Predictors of reporting adequate amount of sleep *p < 0.05 indicates significance; logistic regression, final model explained 15.8-21.5% of variance in sleep status.
- 57. Comparison of significant correlates by different sleep levels N 7 or more hrs of sleep 5-6 hrs of sleep/night p value* 95% CIs of Difference Mean ±SE Mean ±SE Fish intake frequency/wk 154 1.38 ± 1.16 0.98 ± 0.94 0.0321 (-0.76, -0.06) Coffee and tea intake frequency/day 154 1.40 ± 0.14 2.30 ± 0.29 0.0072 (0.25, 1.56) *p < 0.05 indicates significance, independent samples t-tests. 1ANCOVA; Adj means: 2.31 ± 0.28 vs 1.54 ± 0.21, p = 0.033, pƞ2 = 0.04. 2ANCOVA; Adj means: 1.10 ± 0.17 vs 1.30 ± 0.13, p = 0.346, pƞ2 = 0.01.
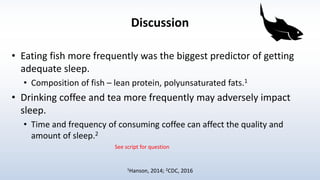
- 58. Discussion • Eating fish more frequently was the biggest predictor of getting adequate sleep. • Composition of fish – lean protein, polyunsaturated fats.1 • Drinking coffee and tea more frequently may adversely impact sleep. • Time and frequency of consuming coffee can affect the quality and amount of sleep.2 1Hanson, 2014; 2CDC, 2016 See script for question
- 59. Background: High Blood Pressure 1American Heart Association, 2014; 2American Heart Association, 2013; 3Ettehad et al, 2016 • Goal blood pressure (BP) reading for an adult age 20 or overis < 120/80 mm Hg.1 • 69% of people who have a first heart attack, 77% who have a first stroke, and 74% who have congestive heart failure have BP > 140/90 mm Hg.2 • Lowering BP reduces vascular risk across various baseline BP levels and comorbidities.3
- 60. Methods • Have you ever been told by a doctor, nurse, or other licensed health professional that you have high blood pressure? –1=Yes –2=Yes, during pregnancy only (female) –3=No –4=Told borderline high or pre-hypertensive –5=Don't know/ Not sure • Question taken from BRFSS 2013 Questionnaire
- 61. N No High BP n= 88 Yes High BP n= 68 p value* Gender (count M/F) 56 / 100 26 / 62 30 / 38 0.0871 Age (mean ± SE) 156 55.14 ± 1.62 63.38 ± 1.53 0.0002 *p < 0.05 indicates significance. 1Chi-square test for independence. 2Independent samples t-test; t (154) = 3.62, ƞ2 = 0.08. High blood pressure by gender and age
- 62. Significant correlates with BP status Variables N High BP (N/Y) r or rho / p value* Waist circumference 122 0.349 / 0.000 Age 156 0.280 / 0.000 BMI 123 0.225 / 0.012 Days of debilitating mental health 156 0.223 / 0.005 Perception of general health 156 -0.209 / 0.009 Health professional visits 155 0.206 / 0.010 Days of pain affecting activities 151 0.194 / 0.017 Days of poor physical health 156 0.167 / 0.037 Tilapia/catfish intake frequency/wk 153 0.161 / 0.047 *p < 0.05 indicates significance; Pearson product moment and Spearman rank order correlations. All variables are low to high in rank.
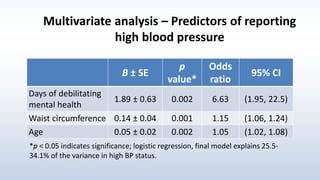
- 63. Multivariate analysis – Predictors of reporting high blood pressure B ± SE p value* Odds ratio 95% CI Days of debilitating mental health 1.89 ± 0.63 0.002 6.63 (1.95, 22.5) Waist circumference 0.14 ± 0.04 0.001 1.15 (1.06, 1.24) Age 0.05 ± 0.02 0.002 1.05 (1.02, 1.08) *p < 0.05 indicates significance; logistic regression, final model explains 25.5- 34.1% of the variance in high BP status.
- 64. Comparison of tilapia/catfish intake frequency by BP status N No BP diagnosis n=88 BP diagnosis n=68 p value* No tilapia/catfish intake/wk 114 62.3% 37.7% 0.0331 1-3 servings of tilapia/catfish/wk 39 41.0% 59.0% *p < 0.05 indicates significance. 1Chi-square test for independence; X2 (1, n = 153) = 4.52, phi = -0.19.
- 65. Discussion • Days of debilitating mental health was the biggest predictor of high BP diagnosis. – Spirituality may serve as coping mechanism for negative emotions.1 • Eating tilapia/catfish frequently may raise BP. – Tilapia/catfish are major sources of long chain n-6 fatty acid, arachidonic acid (AA)2; low eicosapentaenoic acid (EPA) to AA ratio may increase CAD risk.2,3 1Kretchy, 2014; 2Weaver, 2008; 3Nagahara, 2016
- 66. Key Findings • Reduced physical activity musculoskeletal disorders, sadness, anxiety • Higher BMI/WC high blood pressure, pain • Western diet musculoskeletal disorders, inadequate sleep, increased BMI/WC, blood pressure
- 67. Strengths and Limitations Strengths • Validated questions utilized • Wide variety of questions • Large sample size • Consistency of student roles • Physical measurements obtained at data collection • Exploration of topic with limited research Limitations • Cross-sectional correlational study • Self-reported retrospective survey data • Length and personal questions • Food frequency only • Low generalizability
- 68. Conclusion • Health behaviors and predisposing demographic factors were associated with various physical and mental health conditions in church participants. • Future interventions: physical activity, BMI/WC, dietary habits.
- 69. Future Research • Health education intervention studies aimed at reducing risk of or helping manage identified conditions. • More faith-based community health needs assessments.
- 70. Acknowledgements • Gloria Dei Lutheran Church Wellness Cabinet • Gift cards, BU gear • MPH students • Dr. Beezhold
- 71. References AAPM facts and figures on pain. The American Academy of Pain Medicine Web site. http://www.painmed.org/patientcenter/facts_on_pain.aspx. Accessed August 30, 2016. Adult Obesity Facts. Centers for Disease Control and Prevention Web site. https://www.cdc.gov/obesity/data/adult.html. Published September 1, 2016. Accessed October 7, 2016. American Heart Association. High blood pressure. American Heart Association Web site. http://www.heart.org/HEARTORG/Conditions/HighBloodPressure/High- Blood-Pressure-or-Hypertension_UCM_002020_SubHomePage.jsp. Updated 2014. Accessed 2016. American Heart Association/American Stroke Association. Statistical fact sheet 2013 update - high blood pressure. American Heart Association Web site. http://www.heart.org/idc/groups/heart-public/@wcm/@sop/@smd/documents/downloadable/ucm_319587.pdf. Updated 2013. Accessed 2016. Anandacoomarasamy, A, Caterson I, Sambrook P, Fransen M, March L. The impact of obesity of musculoskeletal system. Int J Obesity. 2008; 32: doi:10.1038/sj.ijo.0803715. Ashfield-Watt PAL, Welch AA, Godward S, Bingham SA. Effect of a pilot community intervention on fruit and vegetable intakes: use of FACET (Five-a-day Community Evaluation Tool). Public Health Nutr. 2007;10(7):671-680. doi:10.1017/S1368980007382517. Ball JW, Bice MR, Parry T. Adults' motivation for physical activity: Differentiating motives for exercise, sport, and recreation. RSJ. 2014;38:130-142. Bhaskaran K, Douglas I, Forbes H, dos-Santos-Silva I, Leon DA, Smeeth L. Body-mass index and risk of 22 specific cancers: a population-based cohort study of 5·24 million UK adults. Lancet. 2014; 384: 755–765. Blumenthal JA, Smith PJ, Hoffman BM. Is Exercise a Viable Treatment for Depression? ACSM’s health & fitness journal. 2012;16(4):14-21. doi:10.1249/01.FIT.0000416000.09526.eb.3. Sharma A, Madaan V, Petty FD. Exercise for Mental Health. Primary Care Companion to J Clin Psych. 2006;8(2):106. Calder PC. The role of marine omega-3 (n-3) fatty acids in inflammatory processes, atherosclerosis and plaque stability. Mol Nutr Food Res. 2012;56(7):1073-1080. Centers for Disease Control and Prevention. High blood pressure fact sheet. CDC Division for Heart Disease and Stroke Prevention Web site. http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_bloodpressure.htm. Updated 2016. Accessed 2016.
- 72. References Chau JY, van der Ploeg HP, Merom D, Chey T, Bauman AE. Cross-sectional associations between occupational and leisure-time sitting, physical activity and obesity in working adults. Prev Med. 2012; 54: 195-200. Ciolac EG, Rodrigues-da-Silva JM. Resistance training as a tool for preventing and treating musculoskeletal disorders. Sports Med. 2016; doi: 10.1007/s40279-016-0507-z Croezen S, Avendano M, Burdorf A, van Lenthe F. Social participation and depression in old age: a fixed-effects analysis in 10 European coutnries. Am. J. Epidemiol. (2015) 182 (2): 168-176. doi: 10.1093/aje/kwv015 Definitions and types of pain. Department of Pain Medicine & Palliative Care Web site. http://www.healingchronicpain.org/introduction/definitions. Accessed August 30, 2016. Ettehad D, Emdin CA, Kiran A, et al. Blood pressure lowering for prevention of cardiovascular disease and death: A systematic review and meta-analysis. Lancet. 2016;387(10022):957-967. Gheno R, Cepparo JM, Rosca CE, Cotten A. Musculoskeletal disorders in the elderly. J Clin Imaging Sci. 2012; 2: 39. Godin G, Shephard RJ. Godin Leisure-Time Exercise Questionnaire. Med Sci Sports Exerc. 1997;S36-S38. Goldberg RJ, Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain. 2007; 129(1-2): 210-23. doi: 10.1016/j.pain.2007.01.020. Harris W, et al. Omega-6 fatty acids and risk for cardiovascular disease: A science advisory from the American heart association nutrition subcommittee of the council on nutrition, physical activity, and metabolism; council on cardiovascular nursing; and council on epidemiology and prevention. Circulation. 2009;119(6). Harvard Medical School (2007) Department of Health Care Policy, National Comorbidity Survey, “NSC-R Twelve-Month Prevalence Estimates” http://www.hcp.med.harvard.edu/ncs/ftpdir/NCS-R_12-month_Prevalence_Estimates.pdf (Accessed 7th December 2015). Health risks of being overweight. National Institute of Diabetes and Digestive and Kidney Services Web site. https://www.niddk.nih.gov/health- information/health-topics/weightcontrol/health_risks_being_overweight/Pages/health-risks-being-overweight.aspx. Published December 2012. Accessed August 30, 2016. Helmerhorst HHJF, Brage S, Warren J, Besson H, Ekelund U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int J Behav Nutr Phys Act. 2012; 9(103):1-55. doi: 10.1186/1479-5868-9-103.
- 73. John U, Hanke M, Meyer C, Volzke H, Baumeister SE, Alte D. Tobacco smoking in relation to pain in a national general population survey. Prev Med. 2006; 43(6): 477-81. doi: 10.1016/j.ypmed.2006.07.005. Kretchy IA, Owusu-Daaku FT, Danquah SA. Mental health in hypertension: Assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int J Ment Health Syst. 2014;8:25-4458-8-25. eCollection 2014. Labounty TM, Gomez MJ, Achenbach S, et al. Body mass index and the prevalence, severity, and risk of coronary artery disease: an international multicentre study of 13 874 patients. Eur Heart J Cardiovasc Imaging. 2013; 14: 456-463. Malik VS, Pan A, Willett WC, Hu FB. Sugar-sweetened beverages and weight gain in children and adults: a systematic review and meta-analysis. Am J Clin Nutr. 2013; 98: 1084-1102. Miller L, Bansal R, Wickramaratne P, Hao X, Tenke C, Weissman M, Peterson B. Neuroanatomical Correlates of Religiosity and Spirituality. JAMA Psychiatry, 2013; 1 DOI: 10.1001/jamapsychiatry.2013.3067. Moreira LDF, de Oliveira ML, Lirani-Galvao AP, Marin-Mio RV, dos Santos RN, Lazaretti-Castro M. Physical exercise and osteoporosis: Effects of different types of exercises on bone and physical function of postmenopausal women. Arq Bras Endocrinol Metabol. 2014; 58: 514–522. doi: 10.1590/0004-2730000003374. Musculoskeletal diseases and the burden they cause in the United States. http://www.boneandjointburden.org/. Published 2013. Accessed August 30, 2016. Nagahara Y, Motoyama S, Sarai M, et al. Eicosapentaenoic acid to arachidonic acid (EPA/AA) ratio as an associated factor of high risk plaque on coronary computed tomography in patients without coronary artery disease. Atherosclerosis. 2016;250:30-37. Nelson DE, Holtzman D, Bolen J, Stanwyck CA, Mack KA. Reliability and validity of measures from the Behavioral Risk Factor Surveillance System (BRFSS). Präventivmed. 2001; 46(Suppl 1): S03-S42. Nijhius J, Rensen SS, Slaats Y, Van Dielen FM, Buur,am WA, Greve JW. Neutrophil activation in morbid obesity, chronic activation of acute inflammation. Obesity. 2009; 17(11): 2014-8. doi: 10.1038/oby.2009.113. Nilsen TIL, Holtermann A, Mork PJ. Physical exercise, body mass index, and risk of chornic pain in the low back and neck/shoulders: longitudinal data from the Nord- Trondelag Health Study. Am J Epidemiol. 2011; 1-7. doi:10.1093/aje/kwr087. References
- 74. References NIMH. Major depression among adults. 2014. http://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adults.shtml Odegaard AO, Choh AC, Czerwinski SA, Towne B, Demerath EW. Sugar-sweetened and diet beverages in relation to visceral adipose tissue. Obesity. 2012; 20(3): 689-691. Oliviero F, Spinella P, Fiocco U, Ramonda R, Sfriso P, Punzi L. How the Mediterranean diet and some of its components modulate inflammatory pathways in arthritis. Swiss Med Wkly. 2015; 145:w14190 Patterson E, Wall R, Fitzgerald GF, Ross RP, Stanton C. Health implications of high dietary omega-6 polyunsaturated fatty acids. J Nutr Metab. 2012; doi: 10.1155/2012/539426. Pattison DJ, Symmons DPM, Lunt M, et al. Dietary risk factors for the development of inflammatory polyarthritis: Evidence for a role of high level red meat consumption. Arthritis Rheum. 2004; 50: 3804-3812. Payne ME, Steck SE, George RR, Steffens DC. Fruit, Vegetable and Antioxidant Intakes are Lower in Older Adults with Depression. Journal of the Academy of Nutrition and Dietetics. 2012;112(12):2022-2027. doi:10.1016/j.jand.2012.08.026. Rizzo NS, Sabate J, Jaceldo-Siegl K, Fraser GE. Vegetarian dietary patterns are associated with a lower risk of metabolic syndrome. Diabetes Care. 2011; 34: 1225-1227. Sharma A, Madaan V, Petty FD. Exercise for Mental Health. Primary Care Companion to J Clin Psych. 2006;8(2):106. Spears B, Ricordi C. Anti-inflammatory nutrition as a pharmacological approach to treat obesity. J Obes. 2011; 1-14. doi: 10.1155/2011/431985. Teychenne M, Costigan SA, Parker K. The association between sedentary behaviour and risk of anxiety: a systematic review. BMC Public Health. 2015;15:513. doi:10.1186/s12889-015-184 U.S. world and population clock. United States Census Bureau Web site. http://www.census.gov/popclock/. Accessed August 30, 2016. Van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology- where do lifestyle factors fit in? Br J Pain. 2013; 7(4): 209-17. doi: 10.1177/2049463713493264. Weaver KL, Ivester P, Chilton JA, Wilson MD, Pandey P, Chilton FH. The content of favorable and unfavorable polyunsaturated fatty acids found in commonly eaten fish. J Am Diet Assoc. 2008;108(7):1178-1185. What is an inflammation. PubMed Health Web site. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072482/. Accessed August 30, 2016. Young SN. How to increase serotonin in the human brain without drugs. Journal of Psychiatry & Neuroscience : JPN. 2007;32(6):394-399. Zdziarski LA, Wasser JG, Vincent HK. Chronic pain management in the obese patient: a focused review of key challenges and potential exercise solutions. J Pain Res. 2015; 8: 63-77. doi: 10.2147/JPR.S55360.
- 75. Questions?