





























Health Education and promotion-Dr Sudeep.pptx
- 1. HEALTH EDUCATION & PROMOTION DR SUDEEP DEPT OF PHD
- 2. CONTENTS INTRODUCTION HEALTH EDUCATION ● Definition ● Objectives ● Approaches To Achieve Health ● Models Of Health Education ● Principles Of Health Education ● Contents Of Health Education ● Health Education & Propoganda ● Communication ● Educational Aids Used ● Methods HEALTH PROMOTION ● Definition ● Logo ● Priority Action Areas ● Approaches CONCLUSION REFERENCE
- 3. INTRODUCTION Education Latin*Educare and *Educere:to bring out and to lead Health education is an active learning process, which aims at favorably changing attitudes and influencing behavior with respect to health practices. The same principles, which govern any learning situation, are inherent in the process of health education. For example, there must be motivation to learn, a value placed on the learning and participation of the learner. Education is a learning process or a series of learning experiences through which an Individual informs and orients himself to develop skills and intelligent action. Health education is vital to the practice of prevention. It is the channel for reaching the people and alerting them to the doctor's services and to all other community health resources. A "health- educated" person is well aware of his own responsibility and of the steps he himself must take to receive the full benefits of prevention at all levels.
- 4. DEFINITION “Health Education comprises consciously constructed opportunities for learning involving some form of communication designed to improve health, literacy, including improving knowledge and developing life skills which are conductive to individuals and community health.” -WHO Health Promotion Glossary,1998
- 5. OBJECTIVES ● Informing people( Cognitive objective) :People are informed about different diseases, etiology and how to prevent them. ● Motivating people (Affective objective): It is concerned with clarifying, forming or changing attitudes, beliefs, values or opinions. The mere presence of information does not improve health. Motivate them to alter their lifestyles so that it becomes favorable to promoting health and preventing disease. Motivation has been defined as "a combination of forces which initiate, direct and sustain behaviors". ● Guiding into action (Behavioral objective) :It is concerned with the development of skills and action. A person who has obtained health information might be motivated to change his behavior and lifestyle. However he might need professional help and guidance so as to bring about these changes and to sustain these altered lifestyles.
- 6. APPROACHES TO ACHIEVE HEALTH 1. Legal or regulatory approach 2. Administrative or service approach 3. Educational approach 4. Primary health care approach
- 7. 1. Legal or regulatory approach: This is the form of approach that makes use of the law. The government makes laws and regulations in order to safeguard the health of its people. Examples for this type of approaches include, • Epidemic Diseases Act,1897 • Pollution Act,1981 • Food Adulteration Act 1954 and • Environmental Act.1986 Drawbacks: • They are applicable only at certain times or in limited situations. • They may not alter the behavior of the individual. • These laws are not democratic since they interfere with an individual's personal choices.
- 8. 2. Administrative or service approach: This form of approach intends to provide all the health facilities to the people with the hope that they will use it. Drawbacks: *It becomes a failure if the service is not based on the felt needs of the people. Eg: A dental program using sophisticated equipment, providing all kinds of treatment free of charge might become a failure if *It is planned in an area where there is an epidemic of gastroenteritis. 3. Educational approach: This form of approach is found to be the most effective means for achievement of changes in the health practices and life- styles of the community. The components of this approach are motivation, communication and decision making. Another important factor in this approach is that sufficient time should be allowed for the individual to bring about the desired changes in his behavior. It may involve not only learning new "facts" but "unlearning" wrong information as well.
- 9. 4. Primary health care approach: This is an approach that involves full participation and active involvement of the people starting from the planning stage till the delivery of health services. This is based on the principles of primary health care, i.e., community participation. This can be achieved by providing the necessary guidance to help people identify their health problems and to find solutions to these problems. MODELS OF HEALTH EDUCATION 1. Medical model The medical model is concerned with the diagnosis and treatment of disease and technological advances to facilitate this process. Health Information was provided to people hoping that they would use this information to improve their health.
- 10. 2. Motivation model When people did not use the information provided to them, it was felt that just providing information is not sufficient, the individual must be motivated to translate the health information into action. But the adoption of new behavior is not a simple act, it is a process consisting of several stages, Stages in the adoption of new ideas and practicel ● Unawareness ● Awareness ● Interest ● Evaluation ● Trial ● Adoption
- 11. a) Stage of unawareness: This is the stage in which the individual is not aware of the new idea or practice. b) Stage of awareness: some This is the stage in which the individual has general information about the new idea or practice, but he does not know much about it's usefulness, limitations etc. c) Stage of interest: This is the stage in which the individual shows interest in knowing more about the new idea or practice. The individual is keen to listen to or read about the new method. d) Stage of evaluation: This is the stage in which theindividual tries to find out the advantages and disadvantages of the new method. He evaluates whether the new practice will be beneficial to him and his family. After proper evaluation the individual takes a decision to accept or reject the new idea. e) Stage of trial: This is the stage in which the individual decides to put the new idea or method into practice. Additional information and proper guidance should be given at this stage to the individual to eliminate problems encountered in putting the new method into practice.
- 12. f) Stage of adoption: This is the stage in which the individual finally accepts the new idea or practice as beneficial to him and adopts it. The individual can also reject the idea or practice at any stage, either because he feels it is not of any benefit to him, or because of economic or cultural reasons or because adequate information was not made available to him. All these stages need not be followed in adopting a new idea or practice. Some stages may be skipped. The adoption of the practice as part of his own existing values is called internalization. These stages can also be summarized as: (given by Prochaska and DiClemente, 1992) 1. The pre-contemplation stage Here, the person is engaged in a certain type of behavior, which is unhealthy and he is continuing with this behavior 2. The contemplation stage Here, the person is thinking of changing his behavior and studying the pros and cons
- 13. 3. The preparation stage Here, the person has decided to make the change and is preparing himself by making plans 4. The action stage Here, the actual behavior change is done 5. The maintenance stage Here, the person is maintaining the changed behavior
- 14. 3. Social intervention model The motivation model ignored the fact that in a number of situations, it is not the individual alone who needs to be changed but also his social environment. It was also found that people will readily accept and try something new when it has been approved by the group to which they belong. This gave birth to the idea of social intervention model. Eg: When helping a person quit the habit of smoking, in addition to motivating him, there is also a need to change his social environment. Tobacco cessation is easier when a person is in an environment in which people don't smoke, when there is no cigarette exposure at home and when spouse or friends did not smoke. Therefore, a coherent strategy needs to be developed with a combination of approaches using all methods to change behavior promote health
- 15. PRINCIPLES OF HEALTH EDUCATION The principles of health education, can be categorized as follows: 1. Credibility 2. Interest 3. Participation 4. Motivation 5. Comprehension 6. Reinforcement 7. Learning by doing 8. Known to unknown 9. Setting an example 10. Good human relations 11. Feedback 12. Community leaders
- 16. 1. Credibility It is the degree to which the message is perceived as trustworthy by the receiver. It should be scientifically proven, based on facts and should be compatible with local culture and social goals 2. Interest If the health education topic is of interest to the people, they will listen to it. The health educator should identify the "felt needs" of the people and then prepare a program that they can actively participate in to make it successful. Felt needs is the, requirement of, or, care as determined by the patient or the public. 3. Participation The health educator should encourage people to participate in the program. Once the people are given a chance to take part in the program it leads to their acceptance of the program. Certain methods like group discussions, panel discussions etc. provide opportunities for people's participation. 4. Motivation Motivation can be defined as "the fundamental desire for learning in an Individual. Motives are of two types Primary motives and Secondary motives. The primary motives in life are inborn desires and/or forces, which drives an individual into action.
- 17. ● Food, clothing and housing are examples of primary motives The secondary motives are desires that are the results of outside forces. Examples for secondary motives are gifts, love, a word of praise, rewards etc. ● In health education, the need for incentives is a first step in learning to change. The incentives may be positive or negative. Praise, rewards and promise of health are examples of positive incentives whereas punishment or fear of death are negative incentives. ● Health education can also be facilitated by the motivation provided by the desire to achieve individual goals. For example, for a teenager, esthetics might be a motive to take care of his/her teeth whereas for an adult, the expenses of undergoing restorative care might be the motivating factor for taking care of his/her teeth.
- 18. 5. Comprehension It refers to the level of understanding of the people who receive the health education. The health educator should first determine the level of literacy and understanding of the audience and act accordingly. Words that are strange or new to the people should not be used. Usage of technical or medical terms, which are not familiar to the common man should be avoided. Eg: A statement saying "Eat food items which are non cariogenic may not be comprehensive to the layman. A better way of explaining would be Avoid food stuffs which are sweet and which stick to your teeth like toffees and pastries. Eat food items like fruits and raw vegetables which in addition to being healthy, also help in keeping your teeth clean." 6. Reinforcement This is the principle that refers to the repetition needed in health education. It is not possible for the people to learn new things in a short period of time.Sorepetition is a good idea. This can be done at regular intervals and it helps people to understand new ideas or practices better This principle can be called as a "booster dose" in health education.
- 19. 7. Learning by doing Just by listening to new ideas or sering new things, it might be difficult to implement them. If the learning process is accompanied by doing the new things, it is better instilled in the minds of the people This principle is based on the famous Chinese proverb "if I hear, I forget, If I see. I remember; If I do, I know" Eg: It is difficult to even remember the method of tooth brushing if the procedure is only heard on the radio. It might be difficult to master the act of proper tooth brushing even by watching a demonstration. However, after the demonstration, if it is practiced under the guidance of an expert, the proper method of tooth brushing can be learnt. 8. Known to unknown Before the start of any health education program, the health educator should find out how much the people alre know and then give them the new knowledge The existing knowledge of the people can be used as the basic st upon which new knowledge can be placed. Eg: A health education program with the aim of introducing a toothbrush to a rural population will be better
- 20. 9. Setting an example The health educator should follow what he preaches. He should set an example for other people to follow. Eg A health educator who participates in a program highlighting the ill effects of tobacco should not be seen smoking since it sends a wrong signal and the seriousness of the situation is lost. 10. Good human relations This principle states that the health educator should have good personal qualities and should be able to maintain friendly relations with the people. The health educator should have a kind and sympathetic attitude towards the people and should always be helpful to them in clarifying their doubts or repeating what is not understood 11. Feedback For any program to be successful it is necessary to collect a feedback to find out if any modifications are needed to make the program more effective.
- 21. 12. Community leaders Community leaders can be used to reach the people of the community and to convince them about the need for health education. The leaders can also be used to educate the people, as they will have a rapport and will be familiar with the people of their community. The leader will have an understanding of the needs of the community and advise and guide them. Health education for rural people can be achieved through the head of the village, whereas school children can be approached through the headmaster or school teacher
- 22. CONTENTS OF HEALTH EDUCATION The contents of health education can be categorized into seven main divisions as follows: ● Human biology ● Nutrition ● Hygiene ● Family health care ● Control of communicable & non ● Communicable diseases ● Prevention of accidents ● Use of health services
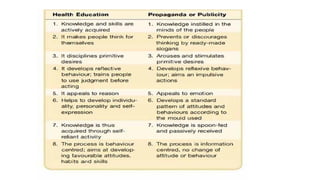
- 23. HEALTH EDUCATION AND PROPAGANDA Propaganda is merely a publicity campaign aimed at presenting a particular thing or concept in a favorable light in such a way that the public may accept it without thinking about it analytically. Health education on the other hand, promotes active thinking and assessment of the problem by the people and encourages them to decide for themselves whether they want to change and in what manner.
- 25. COMMUNICATION Communication is regarded as a two way process of exchanging or shaping ideas, feelings and information to bring about desired changes in human behavior. According to the "Soil, Seed and Sower" principle, the people to whom health education is given can be compared to the soil, the health facts to be given can be compared to the seeds and the media used to transmit the facts can be compared to the sower. Definition: Health communication is defined as "a key strategy to inform the public about health concerns and to maintain important health issues on the public agenda. The use of the mass and multimedia and other technological innovations to disseminate useful health information to the public, increases awareness of specific aspects of individual and collective health as well as importance of health in development. -WHO Health Promotion Glossary, 1998 Communication is essentially the transfer of ideas, messages or information from one person to another. Communicating is like a two-way street. which entails the relation between the sender and the receiver.
- 26. In this process, a cycle of communicating messages is formed between the sender and the receiver. The sender is required to conceive the message he/she wishes to send, encode this message and then transmit. The receiver then is required to receive the message, decode is and clarify his/her understanding of the message. It is effective when it gets the desired action or response. From the sender's perspective one needs to have the following essential skills: • Skills to compose the message • Skills to send the message From the receiver's perspective one needs to have the following essential skills: The skill of receiving a message • Without assumptions • Placing biases aside • Actively listening
- 27. Components of communication The components of communication are: Sender, receiver, message, channels of communication and feedback. Sender: • He is the originator of the message • His objectives should be clearly defined • He should know the interests and needs of his audience • He should know the message • He should know the channels of communication Receiver: The audience may be a single person or a group. The 2 types of audience are • Controlled It is held together by a common interest. It is a homogenous group. Eg: A group of school children in a school • Uncontrolled:It is a group, which has gathered together because of curiosity. Eg: An audience of a street play in a busy area. People gather around out of curiosity. They are from different walks of life with differing literacy levels, different socio-economic status, sharing nothing in common
- 28. Message: It is the information transmitted by the communicator to the recipient. A good message must be, • In line with the objective • Based on felt needs • Clear and understandable • Specific and accurate • Timely and adequate • Interesting • Culturally and socially appropriate
- 29. Channels of communication: It is the media used for communication. The media selected should be capable of making the communication effective. The media chosen should be • Efficient in transmitting the message • Attractive to the audience • Easily understandable by the people Able to bring about good response and interaction by the people The most common channel of communication is interpersonal or face- to-face communication. The other methods are mass media like TV, radio and folk media like folk songs, dramas. Feedback: It is the flow of information from the audience to the sender. It provides an opportunity to modify the message and render it more acceptable. Eg: Opinion polls, interviews, questionnaire surveys
- 30. Types of communication 1. One way and two way communication ● One way communication (Didactic): It is a type of communication where the flow of information is one-way from the sender to the receiver. The drawbacks are, • Knowledge is imposed • Learning is authoritative There is little audience participation • No feedback ● .Two way communication (Socratic/ Dilectic): In this method there is participation from both the sender and the receiver. • Learning is active and democratic
- 31. 2. Verbal and non-verbal communication Verbal communication is the traditional way by word of mouth. Non-verbal communication involves a whole range of bodily movements and facial expressions like smile, raised eye brows, frowning. 3. Formal and informal communication Formal communication follows lines of authority, whereas informal communication is conversing with friends or colleagues. Keys to successful communication: ● Personal contact is important ● Always be courteous ● Be consistent and clear ● Listen to others and show interest
- 32. Barriers in communication They can be classified as, a. Psychological barriers: Emotional disturbances, depression, neurosis or any other psychosomatic disorder can cause psychological barriers in communication. When interacting with individuals with psychological problems, special methods and utmost care should be adopted in order to convey the message to them. b. Physiological barriers: They in- clude difficulties in self-expression, difficulties in hearing or seeing, dif- ficulties in understanding etc. When dealing with special groups, Eg: the deaf, dumb or blind, the channels of communication should be selected in such a way as to target that group ef- fectively. c. Environmental barriers: They are due to excessive noise, difficulties in vision and congestion. These can be overcome by making small groups and using appropriate channels of communication. d. Cultural barriers: Communication must take into consideration the cultural factors like patterns of behavior, habits, beliefs, customs, attitudes, religion etc.
- 33. The verbal barriers are: • Attacking • Interrogating • Criticizing • Blaming • Ordering • Threatening • Shouting The non-verbal barriers are: • Flashing eyes • Rolling eyes • Gestures out of exasperation
- 34. EDUCATIONAL AIDS USED IN HEALTH EDUCATION 1)Auditory aids 2) Visual aids and 3) A combination of audio - visual aids. Auditary aids: The auditary aids are based on the principles of sound. The most commonly used audio aids in health education are, a) Megaphones b) Public addressing systems microphones or c) Gramophone records and discs d) Tape recorders e) Radios f) Sound amplifiers
- 35. Visual aids: The visual aids are based on the principles of projection. Visualization helps individu- als to understand better. The visual aids can be classified as projected and non-projected aids, a) Projected aids: These are visual aids, which needs projection from a source on to a screen. The various projected aids include, • Films or Cinemas • Film strips • Slides • Transparencies • Bioscopes • Video cassettes • Silent films
- 36. The advantages of using the above aids are that • Real life situations can be enacted in films • Complete process is self explanatory • Creates a special interest among the audience to watch a film • Situational effects can be shown in a film, which will leave a lasting impression in the viewer's mind b) Non-projected aids: These are visual aids, which do not require any projection. The commonly used aids without projection are, • Blackboard • Pictures, cartoons, photographs, • Charts, posters
- 37. Combination of audio-visual aids: These are the modern media available. The advantage of this type of media is that sound and sight can be combined together to create a better presentation. They include. (a) Televisions (b) Tape and slide combinations (c) Video players and recorders (d) Motion pictures or cinemas (e) Multimedia Computers These also include the traditional media, such as a) Folk dances b) Folk songs c) Puppet shows d) Dramas
- 38. Points to remember when using educational aids in health education: 1. They should be considered as educational tools only. The end product is not the result of the tools but depends upon the "teacher", his technical skills, and the elements of the learning process. 2. The selection and use of audio- visual material should be guided by program objectives. 3. They should be suitable for the groups who are targeted. 4. Educational aids will be more effective when they are used in a good environment with good lighting, ventilation, temperature and comfortable seating.
- 39. METHODS IN HEALTH EDUCATION Health education can be done targeting three main divisions, individuals, groups or the masses. Any one or a combination of these methods can be used depending upon the objectives to be achieved. 1) Individual approach When an individual comes to the dental clinic or a health centre because of illness, the opportunity should be used to educate him on matters of interest such as the cause and nature of his illness, its prevention, beneficial diet, oral hygiene etc. This approach can also be used by public health personnel, since they will be visiting homes and can interact with the individual and their families. Advantages: Can be done in a dentist's consultation room (two-way communication) Discussion, argument and persuasion of an individual to change his behavior is possible There is opportunity for the individual for asking questions and clearing doubts
- 40. Disadvantages: Only small number can benefit Health education is given only to those who come in contact with the dental surgeon or with public health personnel. 2) Group approach Group education is an effective way of educating the community. Suitable medium should be selected based on the group targeted a. Chalk and talk (Lectures) A lecture is defined as "a carefully prepared oral presentation of facts, organized thoughts and ideas by a qualified person The chalk lends the visual component. The characteristics of a lecture are: Should have an opening statement which gives the theme of the lecture Group should not be more than 30 people The duration of the talk should not exceed 15 to 20 minutes Should be based on topic of current interest
- 41. b. Symposium: • A series of speeches on a selected topic Each speaker presents a brief aspect of the topic • There is no discussion among speakers • In the end, the audience may ask questions • The chairman makes a summary at the end of the session
- 42. c. Group discussions: A group is an aggregation of people interacting in a face-to-face situation. Process of identifying problems & finding solutions collectively by members of group • An effective group should consist of 6-12 members The participants are seated in a circle There should be a group leader who initiates the subject, prevents side conversations, encourages everyone to participate and sums up the discussion. There slllhould be a recorder who prepares a report on issues discussed and agreements reached Disadvantages: There may be unequal participation. Some members may be shy and some may be dominating d. Panel discussion: Panel of 4 to 8 experts sit and discuss a topic in front of an audience.. Headed by a chairman who opens the session, introduces the speakers and keeps the discussion going Audience are allowed to ask questions Chairman sums up the different views presented
- 43. e. Workshop: It consists of a series of meetings with emphasis on individual work with the help of resource persons. • The total workshop is divided into small groups and each group will select a chairman and a recorder. • The individuals work, solve a part of the problem, contribute to group discussion and leave the workshop with a plan of action for the problem. f. Conferences or seminars: • Programs range from half day to one week Held on a regional, state or national level • They usually have a theme
- 44. g. Role playing/socio drama: The size of the group should be about 25. The audience should take active part by suggesting alternative solutions and even by taking part in the drama. The situation is dramatized to make communication more effective. It is followed by a discussion of the problem. Puppet shows used in villages is a type of socio drama Useful for children's health education h. Demonstrations: Procedure is carried out step-by-step in front of an audience. The method involves the audience in discussion and has a high motivational value. The audience can then carry out the procedure themselves with expert help
- 45. 3) Mass approach Health education for a large community or the general public can be given using the mass media of communication. Mass communication literally means communication that is given to a community where the people gathered together do not belong to one particular group. Advantages • Large number of people can be reached Disadvantage: One way communication Various mass media used are: a) Television Coverage to large number of people Can also reach illiterate people Can influence public opinion effectively Provides entertainment as well as education Disadvantage is the high cost
- 46. b) Radio • Has a broader audience than television • Can also reach illiterate people • Economical and easily accessible medium • Care should be taken to select the proper language and length of talk c) Documentary films Provide realism and motion Disadvantage is the high cost d) Newspapers / press • Widely disseminated form of literature • Disadvantage is the low readership in urban areas because of television /radios and in rural areas because of illiteracy.
- 47. e) Printed material • Health magazines, health information booklets and educational pamphlets are issued by Government and non - governmental agencies • g) Posters They should catch the eye and must be artistic • Message should be simple and short Should be placed in locations were people frequent like bus stands, hospitals • They should be changed frequently to maintain their effect h) Health museums / exhibitions • If properly organized, they can attract large numbers of people Museums with photographic panels and three dimensional models can be effective Exhibitions must be conducted during fairs or festivals Personal communication is possible in exhibitions where workers can explain each item on the exhibit.
- 48. i) Internet The internet, a fast growing computer based communication system has opened vast capability of transfer of knowledge. There are a number of internet sites, such as WHO, Ministry of Health and Family Welfare, Governm India, providing health information to the community. Disadvantages: • Although large numbers of people are using it, it is still not accessible in rural areas. • There are chances that internet might provide misleading informa- tion without any scientific basis. Therefore, p should be advised to seek information only from web- sites belonging to authorized bodies or associations.
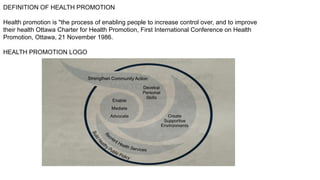
- 49. DEFINITION OF HEALTH PROMOTION Health promotion is "the process of enabling people to increase control over, and to improve their health Ottawa Charter for Health Promotion, First International Conference on Health Promotion, Ottawa, 21 November 1986. HEALTH PROMOTION LOGO
- 50. The main graphic elements of the HP logo are: one outside circle, one round spot within the circle, and three wings that originate from this inner spot, one of which is breaking the outside circle. a) The outside circle, originally in red colour, is representing the goal of "Building Healthy Public Policies", therefore symbolising the need for policies to hold things together This circle is encompassing the three wings, symbolising the need to address all five key action areas of health promotion identified in the Ottawa Charter in an integrated and complementary manner b) The round spot within the circle stands for the three basic strategies for health promotion, enabling mediating, and advocacy", which are needed and applied to all health promotion action areas. c) The three wings represent (and contain the words of the five key action areas for health promotion that were identified in the Ottawa Charter for Health Promotion in 1986. Overall, the logo visualises the idea that Health Promotion is a comprehensive, multi-strategy approach.
- 51. 1. Building healthy public policy Health promotion puts health on the agenda of policy makers in all sectors and at all levels, directing them to be aware of the health consequences of their decisions and to accept their responsibilities for health. Legislative policy can have a very powerful influence on health by creating a social environment, which protects or improves health. Fiscal policy is a part of health promotion, which seeks to influence the cost of items influential to health. Taxation of unhealthy products can increase their cost, making them less affordable However this concept is debatable, sinceit might inrese increase pressure on the most disadvantaged groups in society who are often heavily dependent on these unhealthy products.
- 52. . 2.Creating supportive environment for health Health promotion generates and working conditions that are safe, stimulating, satisfying and enjoyable. The protection of the natural and built environments and the conservation of natural resources must be addressed in any health promotion strategy. The way society organizes work should help create a healthy society. This is termed 'Organizational change Eg: Establishing smoke-free areas, healthy catering services. 3. Strengthening community action for health Health promotion works through concrete and effective community action in setting priorities, making decisions, planning strategies and implementing them to achieve better health. At the heart of this process is the empowerment of communities the ownership and control of their own endeavors and destinies.
- 53. Community development draws on existing human and material resources in the community to enhance self-help and social support. It also develops flexible systems for developing and strengthening public participation in health matters. This requires full and continuous access to information, learning opportunities for health, as well as funding support. Eg: Establishing self-help groups, where people affected by particular oral health problems share their experiences and identify solutions. 4. Developing personal skills Health promotion supports personal and social development through providing in- formation, education for health, and en- hancing life skills. By doing so, it increases the options available to people to exercise more control over their own health and over their environments and to make choic es conducive to health. Enabling people to learn, throughout life, to prepare them- selves for all of its stages and to cope with chronic illness and injuries can be facilitat- ed in school, home, work and community settings by educational, professional, com- mercial and voluntary bodies. Eg: Increasing patient's knowledge about the role of sugar and plaque in the etiology of dental diseases and to develop tooth brushing skills and promote self care
- 54. 5. Re-orienting health services Reorienting health services requires a stronger attention to health research as well as to changes in professional education and training. There must be a change of attitude and organization of health services, with the health sect moving increasingly in a health promotion direction, beyond its responsibility for providing clinical and curative services. The focus must be on development of appropriate high quality oral health care which places greater emphasis on preventive care and on ways of supporting and maintaining oral health. Eg: Dentists can be encouraged and rewarded for effective prevention and research activities. The responsibility for health promotion in health services is shared among individuals, community groups, health pro- fessionals, health service institutions and governments. They must work together towards a health care system, which contributes to the pursuit of health.
- 55. APPROACHES TO HEALTH 1.Educational This approach uses a range of methods to help individuals make informed choices about their health related behavior. Although this approach is largely led by the expert, it does not persuade a person to change, but provides individuals with choices, which they can select on their own. 2. Behavior change It is an expert led approach based upon the assumption that the provision of information will lead to a sustained change in behavior. This approach aims to encourage individuals to take responsibility for their health and adopt healthier lifestyles. It persuades a person to change in a particular direction. 3. Preventive This approach aims at reductionin disease levels in which health professionals act as experts and the patients are passive recipients of preventive care. This is called 'top down' authoritative style of working Eg: Screening program for oral cancer
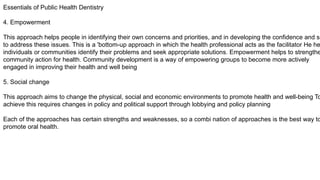
- 56. Essentials of Public Health Dentistry 4. Empowerment This approach helps people in identifying their own concerns and priorities, and in developing the confidence and sk to address these issues. This is a 'bottom-up approach in which the health professional acts as the facilitator He he individuals or communities identify their problems and seek appropriate solutions. Empowerment helps to strengthe community action for health. Community development is a way of empowering groups to become more actively engaged in improving their health and well being 5. Social change This approach aims to change the physical, social and economic environments to promote health and well-being To achieve this requires changes in policy and political support through lobbying and policy planning Each of the approaches has certain strengths and weaknesses, so a combi nation of approaches is the best way to promote oral health.
- 57. CONCLUSION ● Health education and health promotion have the potential to tackle the underlying determinants of oral health and thereby improve the oral health of all sections of society. The success largely depends upon developing partnerships across agencies and actively involving local people in the whole process. ● Health education seldom has an immediate direct impact on behavior. It predisposes behavior through changes in knowledge, attitude, beliefs, values and perceptions. Health education is vital to the practice of prevention. It is the channel for reaching the people and alerting them to health services and resources. ● The focus of health education is on people & their actions through planning and teamwork Its goal is to make realistic improvement in the basic quality of life.
- 59. The classic answer is the ‘babies in the water’ analogy: You’re walking by a river when you see a baby float by. Naturally, you jump in and pull the baby to safety. Then you turn around and see another, and you jump in and do the same. This happens a third time, and a fourth. A downstream approach to the problem is stationing a man there permanently to pull babies out of the water. An upstream approach is finding out how they get into the water in the first place, and preventing it.
- 60. ESSAY 1.Define dental health education. Discuss its principles and classify its barriers.Add a note on audio visual aids. 2.Define health education.Discuss in detail about various methods used. 3.Define health education. Explain its principles and barriers.How do you overcome these barriers? SHORT ESSAY 1.Barriers of health communication .2.Classify various audio-visual aids used in health education. 3.Principles of health education SHORT NOTES 1.Mass media 2.Barriers in communication 3.Audio visual aids 4.Health promotion 5.Seed -soil - sower concept
- 61. Reference: Textbook of Public Health Dentistry ( 7 th Edition)- Soben Peter