Heart failure
Download as PPTX, PDF369 likes158,772 views

The document provides a comprehensive overview of heart failure, including its definitions, classifications based on ejection fraction, cardiac output, and associated symptoms. It outlines risk factors, clinical features, and physical examination findings relevant to heart failure, emphasizing the implications of left and right-sided failures. Additionally, it addresses the epidemiology, etiology, and potential comorbidities affecting patients with heart failure.


























Heart failure
- 1. HEART FAILURE CLASSIFICATION, RISK FACTORS AND CLINICAL FEATURES GUIDE – Dr. L. S. PATIL PRESENTER – Dr DEEPAK R. CHINAGI
- 2. DEFNITION • 2013 ACC/ AHA DEFNITION- – Heart Failure is defined as “ a complex clinical syndrome that results from any structural or functional impairment of ventricular filling(diastole) or ejection of blood. (systole) ”
- 3. CLASSIFICATION BY DEFNITION • SYSTOLIC HEART FAILURE – Characterized by reduced ejection fraction and enlarged ventricle size. Clinically present with left ventricular failure and marked cardiomegaly. • DIASTOLIC HEART FAILURE – Characterized by increased resistance to filling due to increased filling pressures. Clinically present with pulmonary congestion with normal or slightly enlarged ventricles .
- 4. CLASSIFICATION BASED ON EJECTION FRACTION • Heart Failure with reserved Ejection Fraction HFrEF – Ejection fraction ≤ 40% . – These patients will have systolic dysfunction and concomitant diastolic dysfunction. Coronary artery disease is the major cause. • Heart Failure with Preserved Ejection Fraction HFpEF – Ejection Fraction 40 – 50%. – These patients can be diagnosed by 1)clinical signs and symptoms and 2)evidence of pEF or normal EF or previously rEF 3)evidence of abnormal LV diastolic dysfunction (echo / LV catheterisation)
- 5. CLASSIFICATION BASED ON CARDIAC OUTPUT • HIGH OUTPUT FAILURE- – The normal heart fails to maintain normal or increased output in conditions like anemia, hyperthyroidism, pregnancy. – Usually right sided failure occurs followed by left sided failure with presence of shortened circulatory time. • LOW OUTPUT FAILURE- – Heart fails to generate adequate output in conditions like cardiomyopathy, valvular heart disease, tamponade and bradycardia.
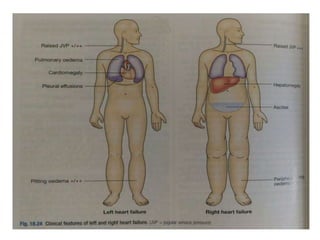
- 6. RIGHT AND LEFT SIDED HEART FAILURE • Right sided heart failure is characterised by the presence of peripheral edema, raised JVP and hypotension and congestive hepatomegaly. • Left sided heart failure – pulmonary edema is the striking feature. Other signs are tachypnea, tachycardia, third heart sound, pulsus alternans, cardiomegaly. • Congestive Cardiac Failure – Characterised by combination of both left and right sided heart failure.
- 8. FORWARD AND BACKWARD HEART FAILURE • FORWARD HEART FAILURE- – This results from inadequate discharge of blood into arterial system leading to poor tissue perfusion and excess Na+ reabsorption through RAAS. • BACKWARD HEART FAILURE- – This results from failure of one or both ventricles to fill normally and discharge its contents, causing back pressure on the atria and venous system.
- 9. ACCF/AHA FUNCTIONAL CLASSIFICATION • Stage A – At high risk of HF but witout structural hear disease. • Stage B – Structural heart disease without signs or symptoms of HF. • Stage C – Structural heart disease with prior HF or current HF. • Stage D – Refractory HF requiring special interventions.
- 10. NYHA FUNCTIONAL CLASSIFICATION • Stage 1 – no limitation of ordinary physical activity. • Stage 2 – slight limitation of ordinary physical activity. • Stage 3 – marked limitation of ordinary physical activity, but comfortable at rest. • Stage 4 – unable to carry out physical activity, symptomatic at rest.
- 11. RISK FACTORS • Epidemiology – – Worldwide 2 crore people are affected by heart failure. Approximate 2 % prevalence in developed countries. Women have better survival than men. – Coronary artery disease is the major cause for heart failure. (60 – 75%) • Etiology and Risk Factors – – Any condition that leads to alteration of LV structure and function can lead to heart failure
- 12. Etiologies of Heart Failure • HFrEF (EF < 40%) – – Coronary Artery Disease (Infarction/Ischemia) – Chronic Pressure Overload (Hypertension/ Valvular Heart Disease - Stenotic) – Chronic Volume Oveload(Valvular Heart Disease- Regurgitant/ Intracardiac shunting) – Non ischemic DCM (Familial/ Infiltrative/ Endocrine/ Toxic/ Inflammatory/ Peripartum/ Stress)
- 13. Etiologies of Heart Failure • HFpEF (EF 40 – 50%)- – Hypertrophic Cardiomyopathy – Hypertensive heart disease – Restrictive Cardiomyopathy(Amyloidosis / Sarcoidosis / Hemochromatosis) – Fibrosis / Endomyocardial Disorders / Aging • Right Heart diseases- – Cor pulmonale – Pulmonary Vascular disorders
- 14. Etiologies of Heart Failure • High output states – Thyrotoxicosis – Nutritional – Beriberi – Anemia
- 15. LV Remodeling • DEFNITION – It refers to change in LV Mass , Volume or Shape or the Composition of the heart after Cardiac injury or index event. • Progress of HF associated with changes in geometry of remodeled LV • Changes that occur include – – LV dilatation – LV thinning – Increase in LV end diastolic volume – Decrease in stroke volume
- 16. LV Remodeling – Subendocardial hypoperfusion – Increased oxidative stress and free radical generation – Stress activated hypertrophic signaling pathways – Incompitence of mitral valve apparatus and functional MR
- 17. CLINICAL FEATURES • Important symptoms – – Fatigue – Exertional Breathlessness • Cause of breathlessness is multifactorial – Pulmonary congestion due to LVF – Accumulation of interstitial and intra alveolar fluid , stimulating juxta capillary J receptors, causing Rapid Shallow breathing – Decreased pulmonary compliance – Increased airway resistance – Respiratory fatigue and Anemia
- 18. CLINICAL FEATURES • Orthopnea – – Dyspnea in recumbent position – Occurs due to redistribution of fluid from splanchnic circulation and lower extremities – Causes increase in pulmonary capillary pressure. – Nocturnal cough is usually asociated with this symptom – Relieved by sitting upright . – This symtom is more common in patients with co morbid obesity or ascites
- 19. CLINICAL FEATURES • Paroxysmal Nocturnal Dyspnea- – Defnition – it refers to acute episode of shortness of breath and coughing that generally occur at night and awken patient from sleep usually 1 – 3 hours after recline. – Associated with coughing or wheeze – Mechanism – increased pressure in bronchial arteries leading to airway compression (+) interstitial pulmonary edema = increased airway resistance. – Orthopnea symptoms resolve after upright posture, but symptoms of PND persist even after upright posture.
- 20. CLINICAL FEATURES • Cheyne stokes respiration – Also called periodic / cyclic respiration – It is present in nearly 40 % cases of HF – It is caused by decreased sensitivity of RESPIRATORY CENTRE to PaCO2. – Due to transient fall in PaO2 , rise in PaCO2 there is an apneustic phase. PaCO2 rises steadily till it stimulates depressed respiratory centre and causes hyperventilation and hypocapnia (low PaCO2).
- 21. CLINICAL FEATURES • Other symptoms like – Anorexia – Nausea – Early satiety – Abdominal pain – Abdominal fullness – Congestive hepatomegaly – Confusion , disorientation, sleep disturbances, – Nocturia
- 22. PHYSICAL EXAMINATION • Patient will present with laboured breathing in an acute LVF. He/she may not be able to finish the sentence due to shortness of breath. He / she may have difficulty to talk due to shortness of breath. • Blood pressure may be normal or high in early HF , may decrease consequently and is usually low. • Low pulse pressure (reduced stroke volume) • Sinus tachycardia (increased sympathetic activity) cool peripheries, cyanosis of tips of fingers and nail bed.
- 23. PHYSICAL EXAMINATION • Jugular venous pressure – – Indicates right atrial pressure – It is measured in terms of (cm of H2O) – Normal < 8 cm of H2O – Method – measure highest point of JVP vertically from sternal angle and add 5 cm of H2O – Positive Abdomino- Jugular reflex
- 24. PHYSICAL EXAMINATION • Respiratory system – Bilateral rales/crepitations may be present as a result of transudate of fluid from intravascular space to intraalveolar space. – May be accompanied by expiratory wheeze (cardiac asthma). – Pleural effusion may/may not be present. (common in CCF)
- 25. PHYSICAL EXAMINATION • Cardiovascular system – Apical impulse may shift inferiorly / laterally. – Sustained apical impulse is felt in severe LVH. – S3 gallop (protodiastolic gallop) can be heard. – Left parasternal impulse in cases if severe RVH – S4 gallop is usually present in diastolic dysfunction. – MR or TR may be present additionally.
- 26. PHYSICAL EXAMINATION • Per abdomen – Hepatomegaly is present (tender / pulsatile) – Pulsations in liver indicate tricuspid regurgitation – Ascites , Jaundice , raised liver enzymes – Peripheral edema can be pre tibial or pre sacral edema • Cardiac cachexia – Cause for cachexia is multifactorial • Elevation of BMR • Elevated circulating cytokines like TNF • Congestion of intestinal veins
- 27. Other Important Comorbidities in HF • Atrial Fibrillation • Anemia • Depression • Others – Diabetes – Arthritis – CKD – COPD
- 28. THANK YOU