



























IPSG.ppt
- 1. Ms.Nikethana R Nair, M.Sc (OBG), MBA (HA), M.Ṣc (Psy)M.Phil (HHSM), Nursing Superintendent, Meenakshi Mission Hospital & Research Center - Madurai
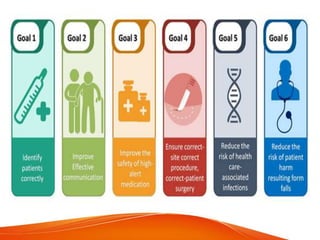
- 3. Goal 1 Identify the Patient Correctly
- 6. Goal 2 Improve Effective Communication
- 10. Other Documents.... • Adverse event data are tracked and used to identify improvements for hand over communications. • Handover between patients and families
- 11. Goal 3 Improve the Safety of High-Alert Medication
- 12. High alert medications are those medications involved in a high percentage of errors/sentinel events, medications that carry a higher risk for adverse outcomes as well as look- alike / sound alike medications. •Chemotherapeutics •All Narcotic Drugs – Fentanyl patches & Injections, Inj. Pethidine, Morphine injections & Tablets, Pentazocine injection •Concentrated electrolytes – I.V. KCL 2mEq/ml or more concentrated, I.V. Potassium Phosphate, I.V. Nacl (more than 0.9%), I.V. Mg Sulphate (50% or more concentrated) •Mg sulfate is stored in 3 to 10 ampules for managing pre eclampsia •Look Alike/ Sound Alike drugs – Staff should know all drugs in LASA •Narrow Therapeutic Index drugs – I.V. Phenytoin, I.V. Aminophylline, Inj. Tacrolimus, Inj. Digoxin, Tab. Lithium carbonate •Anticoagulants – I.V. Heparin, Tab. Acenocoumarol (Acitrom), Tab. Warfarin •Insulins •Antipsychotics – Inj. Haloperidol •Anesthetic – Inj. Ketamine Hydrochloride (All CCU) kept under double lock
- 13. Cont.... • High alert sticker for all high alert medications • Double lock for Narcotics and high concentrated electrolytes • Key custodian • Tall Man lettering for LASA labels • Store LASA drugs in separate racks - Segregation • Color coding for insulin storage • Concentrated electrolytes are stored only in the specific areas • Independent Double check and double sign • Replace the empty ampoules of narcotics • Wastage of narcotics should be discarded in the presence of doctor and obtain doctor’s signature • HAM monitoring • Adverse events to be reported
- 15. Goal 4 Eliminate Wrong site, Wrong patient, Wrong procedure/Surgery
- 19. Goal 5 Reduce the risk of Healthcare Acquired Infections
- 21. Goal 6 Reduce the Risk Of Patient Harm Resulting from Falls
- 22. CARE OF PATIENT Patient safety is a new healthcare discipline that emphasizes the reporting, analysis, and prevention of medical error that often lead to adverse healthcare events.
- 23. Who & When For safety of the patient vulnerability assessment should be done for all the patients at the time of admission
- 24. When to be Used..... • If the AFRAT score is more than or equal to 45 then the Reassessment is done every 48 hrs • If it is less than 45 then re- assessment is done every 7th day • It is done except for HDU and ICU patients because they are already considered to be vulnerable • It is done at the time of admission for all the patients • Fall Risk reassessment is done when the patient condition changes eg.when the patient shifted from ICU to ward, after surgery when the patient shifted to ICU or ward • Moarse Fall Risk Assessment & safety first policy is used to meet the standards
- 26. CRITERIA FOR REASSESSMENT There is a change of disposition in the clinical condition of the patient (eg.post code orange ,code blue) When the patient undergoes a surgery for any reason Patients is placed on restraint Patient ,during his course of stay in the hospital has /develops hearing/vision impairment even with the use of aids Patient uses assistive devices to aid in mobility (eg.crutches,cane,walkers) Patient is disoriented- with impaired cognition, altered sensorium
- 27. SAFETY MEASURES • Patient should not be left unattended • Any untoward incident to be reported immediately • To use Safety belts while transporting patient • Bed to be locked always • Vitals have to be recorded • Safety brochure and fall prevention education to be given. • In case of falls, incident reports have to be documented. • Record the above in PFE form. • IDTR should be filled after 72 hours of admission
- 28. Cont.... • Safety first sticker is placed at the head end of the patient • Side rails should be always up & wheels should be locked when the patient is in the bed • Patient should not be left unattended • Avoid slippery floors • Accompany the patient to the wash room • Safety belt should be on when the patient is transported in the wheel chair or stretcher • Call bell should be at the reach of patient • Any untoward incident should be reported immediately in AIRS • All vulnerable patient’s elimination needs are to be met at the bedside. A bedside commode or bedpan should be provided