















































ITTABV1
- 1. Initial Assessment of the Trauma and Burn Patient Don Reiff, MD Assistant Professor, Section of Trauma/Burns/Critical Care Surgery Clerkship Director
- 2. Magnitude of the Problem What was the greatest medical problem financially and/or related to Hospital inpatient requirements during 1996? Heart Conditions ($58,030 / 2,519,000) Cancer ($37,695 / 1,416,000) Trauma ($37,144 / 1,620,000) COPD, Asthma ($28,594 / 1,291,000)
- 3. Magnitude of the Problem How has this changed by 2003? Trauma ($75,571 / 2,332,000) Heart Conditions ($67,801 / 3,893,000) Cancer ($48,428 / 545,000) Mental Disorders ($47,503 / 1,211,000) *Normal Birth (3,722,000)
- 4. Trauma/Burns Resuscitation Where did the notion of “Trauma Resuscitation” come from? 1976 J.K. Styner, MD piloted a plane in SE Nebraska Crashed resulting in the death of his wife and two of three children
- 5. Trauma/Burns Resuscitation What are the steps of the Trauma Resuscitation? Primary Survey Secondary Survey Lines/Tubes in every orifice Labs and adjuvant studies What are our goals?
- 6. Trauma/Burns Resuscitation What are the steps of the Primary Survey? Airway Breathing Circulation Neurologic Deficit Exposure What are the goals of the primary survey?
- 7. Trauma/Burns Resuscitation Airway Most expeditious means to evaluate the patency and ability to protect airway Should airway control be necessary, what is the best means?
- 8. Trauma/Burns Resuscitation Airway Rapid sequence intubation Cricothyroidotomy
- 9. Trauma/Burns Resuscitation Breathing Assessing the presence of breath sounds using auscultation Life-threatening Injuries Tension pneumothorax Open pneumothorax Flail chest Massive Hemothorax Cardiac Tamponade
- 10. Life-Threatening Chest Injuries Tension Pneumothorax Pathophysiology Progressive entry of air into pleural space Collapse of ipsilateral lung Mediastinal shift Compromised venous return to heart Hypotension / decreased cardiac output Cardiovascular collapse
- 11. Life-Threatening Chest Injuries Open Pneumothorax Physiologically, what’s the issue
- 12. Life-Threatening Chest Injuries Flail Chest Why is this dangerous? Current management is to “ internally” splint patients How would you manage this problem?
- 13. Life-Threatening Chest Injuries Massive Hemothorax Obviously bad for several reasons
- 14. Life-Threatening Chest Injuries Cardiac Tamponade How do we make the diagnosis? What is the physiologic problem and how do you correct it?
- 15. Trauma Resuscitation Circulation Shock is most simply defined as… inadequate delivery of oxygen and nutrients necessary for normal tissue and cellular function Equating shock and blood pressure is inaccurate Compensatory mechanisms result in shunting Reduction in renal blood-flow Reduction in splanchnic blood-flow
- 16. Trauma Resuscitation Causes of shock Obstructive Cardiogenic Neurogenic Septic Hemorrhagic/Hypovolemic Non-hemorrhagic
- 17. Shock Classification of shock Signs/Symptoms Narrowing of pulse pressure Tachycardia Tachypnea Hypotension Oliguria/Anuria Mental Status changes
- 18. Trauma Resuscitation Large bore peripheral IV Poiseuille’s law Bolus two liters of warm fluid Blood and/or coagulation factors Frequently monitor vital signs/UOP for response What about patients who don’t respond appropriately to our initial fluid bolus? Clinical intervention for hemorrhagic shock Q= Pr 4 8 l Large bore peripheral IV Poiseuille’s law Bolus two liters of warm fluid Blood and/or coagulation factors Frequently monitor vital signs/UOP for response Q= Pr 4 8 l
- 19. Algorithm Hemorrhagic Shock Where has the blood gone? Scene •Extremity fractures Thorax •Peritoneum Retroperitoneum How can we quickly eliminate several of the potential sources of blood loss?
- 20. Algorithm Hemorrhagic shock With two of five eliminated, how to work up last three? CXR/Pelvic X-ray Physical examination DPL/US Once identified, institute appropriate therapy Reduce fractures Pelvic binder Chest tube Operating room
- 21. Resuscitation Endpoints Classically, restoration of BP,HR and UOP Using only these parameters will leave 50-85% patients in “compensated” shock Recent data suggests Correction of lactate levels Correction of base deficits Tonomotry
- 22. Case Presentation 38 year old male Unrestrained driver Initially unresponsive, largely obtunded Initial vital signs: HR – 130’s SBP – 105 O2 sats – 92% on NRB
- 23. Approach to the Evaluation of Shock ABC’s Intubate Tachycardic/hypotensive/ hypoxic w/ absent BS Needle decompression w/ concurrent fluid resuscitation No rush of air/vital signs show no improvement “ Non-responder” Go through check list of etiologies
- 24. Case Presentation Primary survey Airway controlled Decreased breath sounds on right Severe shock with HR now 140’s to 150’s and SBP below 100 Non-hemorrhagic sources - Sepsis - Cardiogenic - Neurogenic - Obstructive
- 25. Approach to the Evaluation of Shock Primary survey Needle decompressed/volume resuscitation Non-responder - Sepsis - Cardiogenic - Neurogenic - Obstructive Eliminated CXR has ruled out Tension pneumothorax Use ultrasound to rule out pericardial tamponade All that remains is hypovolemic/hemorrhagic shock
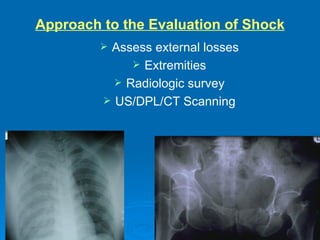
- 26. Approach to the Evaluation of Shock Assess external losses Extremities Radiologic survey US/DPL/CT Scanning
- 27. Case Presentation Right sided 40F chest tube with blood auto-transfused Initial ABG returns with 7.15/35/98/-10/8.5 In addition to auto-transfusion, 4u pRBC’s given slowing HR to 130’s and SBP improves to 115 Repeat ABG finds 7.26/38/135/-9/9.2
- 28. Case Presentation Package and run to CT
- 29. Case Presentation Package and run to operating room
- 30. BURNS
- 31. Presentation ABC’s Determine mechanism Flame, chemical, electrical Associated trauma Complete history and examination Labs and chest x-ray ABG with CO
- 32. Presentation Resuscitation Tetanus Prophylaxis Hypothermia Antibiotics/steroids NOT indicated
- 33. Severity of Injury Dependent on the depth and extent of burn injury. Depth 1 st , 2 nd , 3 rd degree Extent Estimated total burn surface area
- 34. Burn Depth
- 35. Burn Depth 1 st Degree Partial thickness Sun Burn Spontaneous healing
- 37. Burn Depth 2 nd Degree Partial thickness Usually heals spontaneously Involve epidermis and varying thickness of dermis
- 39. Burn Depth 3 rd Degree Full thickness burn Will not heal spontaneously Excision and Grafting Involves epidermis and dermis
- 41. Burn Depth 4 th degree Involves epidermis, dermis, and underlying structures Fat, fascia, muscle, bone Associated most commonly with electrical burns
- 43. Extent of Burn Rule of 9’s Lund and Browder
- 45. Resuscitation Fluid is determined by the severity of injury mount of 2 nd and 3 rd degree burn Lactated ringers Initial fluid determined by parkland formula 2-4cc/kg/%TBSA ½ over the first 8 hours DO NOT BOLUS Titrate fluid to urine output 30-50cc/hour
- 46. Escharotomy Full-thickness, circumferential burns to extremity or trunk Diminished blood flow to extremity Decreased pulmonary compliance Medial and lateral incisions on the extremities Anterior axillary line on trunk
- 48. Inhalation injury Most common cause of death 80% of burn related deaths Several mechanisms involved Oropharyngeal Tracheo-bronchial Toxic absorption Cyanide Carbon monoxide
- 49. Inhalation injury History Enclosed space Loss of consciousness Drugs and alcohol Physical exam Facial burns, singed nasal hairs Stridor Carbonaceous sputum Depressed mental status
- 50. Carbon Monoxide Most frequent cause of death at the scene. Very high affinity for hemoglobin. Impairs oxygen availability and use in the tissues.