












































Manual muscle testing
- 2. Fundamentals of MANUAL MUSCLE TESTING (MMT) By Dr. Muhammad Ejaz PT DPT (AIMC), MS in Neurology * (UOL) Lecturer Lahore institute of science and technology 9/15/2015 1
- 5. INTRODUCTION TO THE TOPIC MMT is the most vital part of motor assessment Performa in medical examination. MMT is a procedure for the evaluation of strength of individual muscle or muscles group, based upon the effective performance of a movement in relation to the forces of gravity or manual resistance through the available ROM. i.e. how efficiently a muscle is working or muscles strength / power assessment using manual (hand) techniques.
- 6. BASIC COMPONENTS OF MOTOR EXAMINATION 1. Nutrition or bulk of muscle 2. Tone 3. Reflexes 4. Range of Motion or TCD’s assessment 5. Manual muscle testing (MMT) 6. Functional assessment ** Importance of the sequence
- 7. WHY MMT IS PERFORMED? To get some answers such as :- Is a particular muscle is normal? Is it weak ? (how much weak) Is it strong enough? (how much strong) Is it weak on both the sides (bilateral symmetrical) ? Is it weak only on one side (unilateral) ? Is proximal muscles are weaker than distal one ? Is distal muscles are weaker than the proximal one ? Is there any particular pattern of muscle weakness ?
- 8. CLINICAL REASONING OF PERFORMING MMT To get an over view of muscle performance status so that the cause of the problem can be understood. So that we can plan our treatmentgoals i.e. to strengthen certain weak muscles by means of strengthening exercises. Monitoring of certain conditions i.e. whether it is getting better or getting worst with time (Documentation and follow-up) Correlating muscle picture with its level of innervations (Myotomes)
- 9. EXAMPLE - LBA WITH NEUROLOGICAL DEFICIT MYOTOME MUSCLES L1 NONE L2 HIP FLEXOR L3 KNEE EXTENSOR L4 DORSIFLEXOR L5 GREAT TOE EXTENSION S1 PLANTER FLEXORS
- 10. GRADES OF MMT Numerical Objectivity for documentation Existing grading systems are :- 1. MRC SCALE (medical research council ) 2. OXFORD SCALE 3. KENDALL SCALE 4. AND SEVERAL OTHER
- 11. MRC SCALE EXPLANATION 0 No visible or palpable contraction. 1 Visible or palpable contraction. 2 Full ROM gravity eliminated. 3 Full ROM against gravity. 4 Full ROM against gravity, moderate resistance. 5 Full ROM against gravity, maximum resistance. Ref. muscle testing and function by kendall
- 12. OXFORD SCALE EXPLANATION 0 No contraction is present. 1 There is flicker contraction 2 Full ROM with gravity counter balance. *(Eliminated) 3 Full ROM against gravity. 4 Full ROM against gravity + added resistance. 5 Muscle function normally. ref: practical exercise Margaret Holleis(1)
- 13. KENDALL SCALE EXPLANATION NONE No visible or palpable contraction. TRACE Visible or palpable contraction. POOR Full ROM gravity eliminated. FAIR Full ROM against gravity. GOOD Full ROM against gravity, moderate resistance. NORMAL Full ROM against gravity, maximum resistance. Ref. muscle testing and function by kendall
- 14. PLUS (+) AND MINUS (-) GRADES (3) - Full range of motion against gravity (3+) - Full range of motion against gravity slight resistance (3-) - Movement >half but less than full range of motion against gravity
- 17. BASIC RULES Patient position Joint position Check the available passive range of the joint. (P.ROM) Give accurate, audible commands and instruction regarding movement. Demonstrate the desired movement. Check the strength of normal side first (in c/o unilateral). Do not change patient position repeatedly. Always start with Grade 3 i.e. against gravity movement.
- 18. CONT.. Isolation of muscle to be tested. Joint position. 1. Place the part in anti-gravity position. (Grade 3) 2. Horizontal (gravity eliminated) for weak muscle. (Grade 2) Apply gradual pressure opposite to the muscle segment being tested. (Grade 4 and 5) Use long Lever to apply resistance whenever possible. **
- 19. HAND PLACEMENT Proximal Hand:- At origin of muscle & proximal joint giving stabilization. Distal Hand:- distally offering resistance or assistance depending upon performance.
- 20. APPLICATION OF RESISTANCE Resistance is applied slowly and gradually. Increasing or decreasing manual resistance . Increasing or decreasing the length of weight arm. Example - with the patient in prone position a known resistance given at the level of knee joint is more easily overcome by the hip extensors than if it is applied at the foot.
- 21. APPLICATION OF LEVERAGE IN MMT
- 22. PRECAUTIONS Consider contraindications Do not Harm (Be gentle) Respect pain Know the available ROM Follow the principals of procedure Take care of patients comfort Record accurately (Documentation)
- 23. 7) INDICATIONS OF MMT: 1)Lower Motor Neuron (LMN) Disease. 2) Some other Neurological (Neuromuscular )disease. Such as, Multiple Sclerosis Muscular distrophy Guillian - barre syndrome (GBS), etc.... 3)Some Musculoskeletal disorders.
- 24. 8) CONTRAINDICATIONS OF MMT: 1) Cerebral Palsy 2) Cardio vascular disease / Brain injury 3) Dislocated/ unhealed fracture 4) Myositis ossifications 5) Parkinson’s disease 6) Pain 7) Inflammation /(inflammatory disease in muscles and or joints) 8) Severe cardiac & respiratory disease .
- 25. Cont. 9)Subluxation joint 10)Hemophelia (ability of the blood to clot is severely reduced, ) 11)Osteoporosis
- 26. LIMITATIONS OF MMT UMN Lesions :- Spastic muscle have poor control from higher centers thus its better to go for Voluntary control assessment rather than MMT. Presence of pain and swelling:- Pain and swelling increases the intra articular tension causing irritation of joint and can affect the MMT result, Thus in case always mention about presence of Pain along with grade.
- 27. Type of contraction - MMT gives idea about Quality of concentric contraction only. (Not eccentric which is more functional) Understanding of command (Pediatric Age group <5 years / IQ/ higher functions) Strength Vs Endurance?? MMT gives knowledge about only the strength and not the endurance. Subjectivity (Patient) Hoovers Sign
- 28. OBJECTIVITY AND RELIABILITY OF MMT OBJECTIVITY:- Examiners ability to palpate and observe the tendon or muscle response in very weak muscle. RELIABILITY :- reliability of MMT in clinical settings hasbeen low, it is found that percentage of therapist obtaining the same muscle grade, only ranged from 50-60% INTERRATER(rater mean observers ) AND INTRARATE R ( single individual, reusing the same rating instrument, consistently produces the same results ) RELIABILITY Despite of the above said lacunas MMT is still the most effective clinical method for assessing muscle function.
- 29. MMT CHART
- 30. ALTERNATE TECHNIQUES OF ASSESSING MUSCLE STRENGTH APART FROM CONVENTIONAL MMT 1. Resisted isometric test 2. Break test 3. Make test 4. Functional assessment 5. Myometer 6. Dynamometer
- 31. RESISTED ISOMETRIC TESTING Useful way of assessing muscle function when the movement is contraindicated or causes pain. i.e. Resistance to muscle while performing Isometric contraction. The location of pain and painful movements suggests whether a lesion is contractile tissue(muscle or tendon) or inert/ non-contractile tissue (capsule) is involved.
- 32. TESTING Patient’s joint position should be in middle ROM as this position is resting position of the joint. Proximal part is stabilize to minimize substitution. The patient is then asked to hold the position against resistance.
- 33. RESULT INTERPRETATION Findings Possible pathology Strong and painless contraction No neurological deficit Strong and painful contraction Minor lesion of tested muscle or tendon Weak and painless contraction Disorder of nervous system, complete rupture of muscle or tendon or disuse atrophy Weak and painful contraction Fracture, neoplasm, partial rupture of muscle or tendon, inflammation inhibiting contaction.
- 34. BREAK TEST Resistance applied at the end of tested range is termed as break test. Resistance applied throughout the test is called make test. Patient is instructed to complete the test movement and then hold the segment against resistance. The isometric hold (break test) shows the muscle to have a higher grade then the make test. For one joint muscle resistance is applied at end of ROM and for two joint muscle it is applied at mid range.
- 35. INDICATION OF BREAK TEST When movement is contraindicated When there is pain in movement When we have to assess the quality of strength and not the quantity.??
- 36. FUNCTIONAL TEST Correlating the muscle strength with its functions Such as Standing/ walking on toes Standing/ walking on heels Walking on medial or lateral border of foot One leg standing Squatting and up squatting Sit to stand Intrinsic plus hand Backward / forward/ lateral trunk bending / hand to knee.. Gower’s Sign
- 37. GOWER’S SIGN
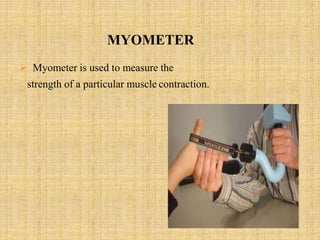
- 38. MYOMETER Myometer is used to measure the strength of a particular muscle contraction.
- 39. DYNAMOMETER Dynamometers are spring loaded device. The best tool for accurately evaluating muscle strength and objective way to document muscle weakness. As force is applied to the dynamometer the spring is compressed and moves a needle to indicate the force output from the muscles.
- 40. GRASP or HAND DYNAMOMETER Types of Dynamometer
- 43. LOW BACK AND LEG DYNAMOMETER .
- 44. ADVANTAGES 1. Easy to use 2. More objective 3. Lesser chances of discrepancy in result 4. Visual Feed back
- 45. DISADVANTAGE 1. Availability 2. Cost 3. No Universal equipments available 4. Group of muscle can be assessed but not individual muscle. (Example Grip strength)
- 46. MMT CLINICAL VARIATION Individual muscle MMT – ex. tendon transfer. Gross MMT – ex Major muscles only as in case ofAmputation. Myotomal MMT – ex Neck or back pain with neurological deficit/ SCI.