

































MECHANISM OF LABOUR.ppt
- 1. MECHANISM OF LABOUR By: Akadango
- 2. LEARNING OUTCOMES To equip students in midwifery to gain knowledge and skill on the mechanism of labor to apply when managing mothers during labor and delivery
- 3. SPECIFIC OBJECTIVES: 1. Explain the concept of normal mechanisms of labor 2. Explain the normal mechanisms of labor in an occiput anterior position 3. Identify processes in the mechanism that are applicable in mechanisms of other head or cephalic presentations 4. Explain factors that influence descent, flexion, rotation and expulsion of the fetus 5. Explain the significance for the midwife of understanding the mechanisms of labor. 6. Reflect on the consequences of not understanding mechanisms of labor
- 4. MATERNAL –FETAL RELATIONSHIPS Review Maternal Fetal Relationships This is important in explaining the processes and factors that determine how the fetus negotiates the maternal pelvis and birth canal in labor and at birth.
- 5. MATERNAL –FETAL RELATIONSHIPS Normal Relationships prior to birth 1. Lie 2. Attitude 3. Presentation 4. Denominator 5. Position 6. Presenting part
- 6. MATERNAL –FETAL RELATIONSHIPS 1.Lie: • Long axis of fetus to long axis of the uterus: • when the long axis of the fetus lies parallel to the long axis of maternal uterus this is a longitudinal relationship as is desirable for normal mechanisms of labor
- 7. MATERNAL –FETAL RELATIONSHIPS 2. Attitude: Fetal limbs and head to its trunk: When the fetal head is flexed with chin on chest, back is bent, arms flexed on the chest, thighs on abdomen and legs on thighs then this is an attitude of flexion
- 8. MATERNAL –FETAL RELATIONSHIPS 3. Presentation: The part of the fetus that lies at the pelvic brim or lower pole of the uterus. Cephalic presentation refers to all head presentations. In a well flexed head the presentation is vertex
- 9. MATERNAL –FETAL RELATIONSHIPS 4. Denominator: The part of the presentation that determines the position of the fetus. In vertex presentation, the denominator is the occiput.
- 10. MATERNAL –FETAL RELATIONSHIPS 5. Position: The relationship of the denominator to the six areas of the pelvic brim (right and left posterior, lateral and anterior. If the occiput points to left anterior the position is left occiput anterior.
- 11. MATERNAL –FETAL RELATIONSHIPS 6. Presenting part: The part that lies over the cervical os during labor on which the caput forms. In left occipito anterior position, the presenting part is the posterior part of the right parietal bone.
- 12. DEFINITION OF MECHANISM OF LABOUR Cardinal movements in first and second stage of labor A series of passive movements of the fetus in its passage through the birth canal to the exterior The canal has different shapes with inlet and outlet differing in size and shape The fetus accommodates itself to the diameters and curve of the pelvic canal The knowledge is significant for the student midwife to manage the progress of normal and abnormal labour
- 13. MECHANISMS OF LABOR The fetal movements occurring during labor because of: expulsive uterine action abdominal muscle contractions, Diaphragm resistance of the pelvic floor.
- 14. MECHANISMS OF LABOR LEFT OCCIPITO ANTERIOR POSITION Fetal Head lies with the occiput in the anterior part of the pelvis on the mother’s left side • Occiput points to the left ileo-pectineal eminence on the left anterior area of the pelvic brim • Sagittal suture is in right oblique diameter of the brim
- 15. MECHANISM OF VERTEX PRESENTATION The expulsive action of the uterine that stimulates the dilatation and effacement of the cervix moves the fetus towards the cervix Resistance is offered by pelvis, cervix and pelvic floor muscles The presenting part reaches the pelvic bones and makes adjustments to pass through the pelvis and down the birth canal
- 16. MECHANISMS OF LABOR Mechanisms of Labor 1. Engagement of the head 2. Flexion of the head 3. Descent (a continuous process) 4. Internal rotation of the head 5. Crowning of the head 6. Extension of the head 7. Restitution of the head 8. Internal rotation of shoulders 9. External rotation of head 10. Lateral flexion of the body
- 17. MECHANISMS OF LABOR LEFT OCCIPITO ANTERIOR POSITION The lie is longitudinal The attitude is that of flexion The Presentation is cephalic The denominator is the occiput Position is Left Occipito anterior The presenting part is the posterior aspect of the right parietal bone The sub-occipito frontal diameter (SOF) (10cms) lies at the pelvic brim. The head is usually flexed with SOF (10cms) lying at the brim.
- 18. CARDINAL MOVEMENTS: 1.ENGAGEMENT OF THE FETAL HEAD This is called lightening or dropping of the fetal head into the pelvic brim Engagement in prims may occur during the latter weeks of pregnancy In multigravida the muscle tone is lax descent and engagement may not occur until labor begins Uterine contractions and retraction allow progress to speed up
- 19. CARDINAL MOVEMENTS: 2.DESCENT: In primgravid it begins two weeks before the onset of labor when engagement occurs unless there is disproportion of the head Further descent happens in 1ST stage of labor due to effective uterine contractions Meeting resistance to the cervix increases flexion of the head Dilating cervix allows the fetal head to descend
- 20. DESCENT:
- 21. CARDINAL MOVEMENTS: 3. FLEXION OF THE HEAD: Flexion is a function of baby’s attitude, anterior position, and anterior position of the head and contractions. When flexion is increased the Suboccipital- bregmatic diameter(9.5cm) engages Smaller presenting diameter facilitates descent The attitude of the fetus is of flexion hence the uterine contractions increase the existing attitude The occiput becomes the leading part that influences next movement that of internal rotation
- 22. FLEXION OF THE HEAD:
- 23. CARDINAL MOVEMENTS: 4.INTERNAL ROTATION OF THE HEAD: With further descent the fetal head rotates anteriorly and the fetus assumes an oblique position The fetus may rotate to occipital anterior position • The movement causes the larger diameters of the head,shoulders and buttocks to emerge under the pubic arch in the antero posterior which is the largest diameter • The head escapes under the pubic arch and allow the sub-occipito region to pivot on the lower border of the symphysis pubis.
- 24. CARDINAL MOVEMENTS: In LOA the occiput rotates forwards 1/8 of the circle from left ilio-pectineal eminence to the symphysis pubis to escape under the pubic arch FACTORS FACILITATING IR: Resistance of the pelvic floor muscle Uterine contractions causes the occiput to stretch the left half of the pelvic floor The pelvic floor direct the leading part towards the front to pass under the pubic arch
- 25. INTERNAL ROTATION OF THE HEAD:
- 26. CARDINAL MOVEMENTS: 5.CROWNING: It is the term used when the occipital prominence escapes under the symphysis pubis A smaller diameter the SOB- 9.5cm distends the vulval orifice instead of the larger SO- Frontal diameter 10cm Head no longer receded between contractions. This means that the widest transverse diameter of the fetal head is born.
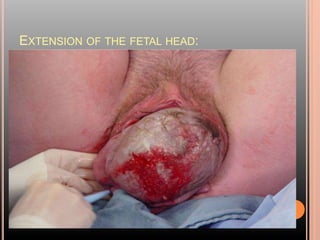
- 27. CARDINAL MOVEMENTS: 6. EXTENTION OF THE FETAL HEAD: Begins after the head crowns The flexion of the head is undone The sinciput,face and chin pass over the thinned perineum It happens due to uterine and abdominal muscles exerting downward pressure The SO- Frontal diameter 10cm sweeps the perineum Brow,face and chin pass over the sacrum and coccyx are over the perineum
- 28. EXTENSION OF THE FETAL HEAD:
- 29. EXTENSION OF THE FETAL HEAD:
- 30. CARDINAL MOVEMENTS: 7.RESTITUTION: This is turning of the head to undo the twist in the neck that took place during internal rotation of the head LOA the occiput restitutes 1/8 of the circle to the left back to where it started before IR took place It helps midwife to deliver the shoulders on the right direction to prevent laceration. LOA or ROA
- 31. CARDINAL MOVEMENTS: 8.INTERNAL ROTATION OF THE SHOULDERS: The shoulders in an LOA are in the left oblique diameter of the pelvic cavity The anterior shoulder reaches the right side of the pelvic floor and rotates forward bringing the shoulders into the Antero-Posterior Diameter of the outlet with effective uterine contractions
- 32. CARDINAL MOVEMENTS: 9. EXTERNAL ROTATION OF THE HEAD: Turning of the head that accompanies internal rotation of the shoulders The occiput turns a further 1/8 of the circle in the same direction as in restitution This indicates that the head is in antero –posterior diameter of the pelvic outlet in readiness for expulsion Allow the ER of head before the shoulders are born
- 33. EXTERNAL ROTATION OF THE HEAD:
- 34. CARDINAL MOVEMENTS: 10. LATERAL FLEXION OF THE BODY: Lateral flexion is a sideways bending of the spine, which takes place while the body is being expelled so that it conforms to the curve of the birth canal Anterior shoulder escapes under the symphysis pubis Posterior shoulder passes over the perineum allowing smaller diameter to distend the vaginal orifice than if both shoulders were expelled simultaneously The baby is carried forward over symphysis pubis towards the mother’s abdomen by the midwife to facilitate lateral flexion