2. At the end of the presentation students will be able to
1. Define Pancreas cancer.
2. Mention the Incidence of Pancreas cancer.
3. List out the etiological factors of Pancreas cancer.
4.Explain the pathophysiology of Pancreas cancer.
5. List down the clinical manifestations of Pancreas cancer.
6. Enlist the diagnostic measures to rule out Pancreas
cancer.
7. Elaborate the collaborative management of patients with
Pancreas cancer.
OBJECTIVES
3. INTRODUCTION
The human body is a composition of cells,
tissues, and organs among others that under typical
conditions work in harmony to preserve health. However,
there are specific instances when certain cells in the
human body develop at an abnormal speed and as a
consequence a person could get sick with different
aliments, including cancer.
4. PANCREAS
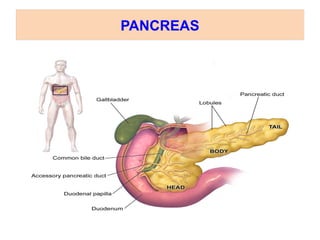
The pancreas is bout 6 inches long and sits across the
back of the abdomen, behind the stomach.
The head of the pancreas is on the right side of the
abdomen and is connected to the duodenum through a
small tube called the pancreatic duct.
The narrow end of the pancreas, called the tail, extends
to the left side of the body.
5. The pancreas plays a very important role in the digestive
process, producing enzymes essential for digestion of
food.
The other function of the pancreas, which can be described
as “fuel control”, is produce insulin.
More than 95% of the cells of the pancreas are exocrine
glands, responsible for producing pancreatic juice.
Such glands break down fats and proteins from food so
that nutrients can be absorbed by the small intestine.
PANCREAS
7. PANCREAS CANCER
• Pancreas cancer is a malignant tumor in the pancreatic
gland
• The exocrine and endocrine cells of the pancreas may
form completely different tumors. These tumors may be
benign
( non – cancerous) or malignant (cancerous).
• Exocrine tumors are by far the most common type of
cancer of the pancreas
8. INCIDENCE
• Annual incidence 10 new cases per 100000 population
• Lowest incidence – India and Middle East
• Incidence increases steadily with age – with 80 % over
6th decade of life
• Male: Female ratio – 2:1
• Pre and post menopausal women ratio is 2: 1
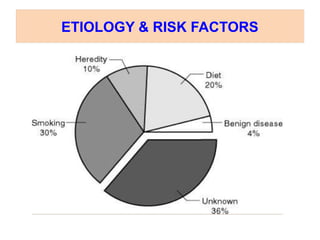
9. ETIOLOGY & RISK FACTORS
• Heredity - cancer family syndromes
• Cigarette smoking
• Diet – high intake of animal fat or meat.
• Occupational exposure to radiations
• Gastric surgeries
• Diabetes mellitus/pernicious anaemia/ chronic
pancreatitis
10. • Hereditary factors
• Most of the pancreatic cancers are sporadic
• 7.8% of pancreatic cancer patients give a positive family
history
• Hereditary syndromes
HNPCC
PZ syndrome
Ataxia Telangiectasia
Hereditary Pancreatitis
Familial Atypical Mole Melanoma syndrome
FAP
ETIOLOGY & RISK FACTORS
11. Diabetes – Is it a cause or effect
• Several studies have shown an increased incidence of
pancreatic cancer in diabetics
• Diabetes is considered as an early symptom of
pancreatic cancer rather than being a cause
• The diabetes of Pancreatic cancer is due to islet cell
dysfunction (Islet Amyloid polypeptide) and not due to
the destruction of the gland
ETIOLOGY & RISK FACTORS
12. Chronic Pancreatitis
Is it premalignant
The incidence of pancreatic cancer in various entities of
chronic Pancreatitis are as follows
Hereditary Pancreatitis 25%
Tropical Pancreatitis 10%
Alcoholic Pancreatitis 5%
ETIOLOGY & RISK FACTORS
14. TUMOURS OF THE PANCREAS
The tumours of the pancreas can be
A. Non-Endocrineneoplasms
B. Endocrineneoplasms
15. ENDOCRINE NEOPLASMS
These are less common than non-endocrine
tumours and generally benign and sometimes multiple.
They includes:
Insulinoma
Glucogonomas
Others: - common
Gastrinomas
Somatostatatinomas
Vipomas (Vasoactive Intestinal Polypeptide)
19. CLINICAL MANIFESTATIONS
It is unfortunate that malignant pancreatic cancers
are asymptomatic until local or systemic complication
develop.
1. Obstruction to bile duct – Jaundice and pruritus
2. Obstruction to duodenum /stomach- Gastric outlet
obstruction
3. Ulceration- Gastro intestinal haemorrhage
4. Trousseau’s syndrome - is an acquired blood clotting
disorder that results in migratory thrombophlebitis
(inflammation of a vein due to a blood clot).
5. Infiltration of peripancreatic nerve roots produce pain
The onset of symptoms are insidious and
progressive Abdominal pain is usually post prandial and in
epigastrium Pain in upper back denotes retroperitoneal
20. SYMPTOMS AND SIGNS CARCINOMA
HEAD OF PANCREAS
1. Weight loss – averaging about 40%
2. Obstructive jaundice
3. Deep seated abdominal pain
4. Non tender palpable gall bladder
5. Cholangitis occurs in 10 % of patients
21. CARCINOMA OF BODY AND TAIL
• Weight loss
• deep seated pain
• jaundice- < 10 % of patient
• sudden onset of diabetes mellitus-25% of patient
• migratory thrombophlebitis- occurs in about 10% patient
22. SYMPTOMS AND SIGNS CARCINOMA OF
AMPULLA OF VATER
1. Pain occurs less frequently – usually its colicky
2. Jaundice is often intermittent
3. Chills and fever – due to associated cholangitis
25. DIAGNOSTIC EVALUATION
Identifying risk factors.
Mass during physical Examination
Ultrasound – Bile duct distension – Mass
CT scan with IV contrast
Triple phase CT (pancreas protocol) 90% accurate at
finding lesions . A scanner takes multiple X-ray pictures,
and a computer reconstructs them into detailed images
of the inside of the abdomen
26. Endoscopic ultrasound
Help find lesions not seen on CT
Help determine resectability
Excellent way to get biopsy
MR cholangiopancreatography (MRCP), which can be
used to look at the pancreatic and bile ducts, is
described below in the section on
cholangiopancreatography.
MR angiography (MRA), which looks at blood vessels, is
mentioned below in the section on angiography.
• Endoscopic retrograde cholangiopancreatography
(ERCP)
DIAGNOSTIC EVALUATION
28. Inoperable disease
Locally Advanced stage III (30-40^)
Chemoradiation
Chemotherapy
Metatatic Stage IV (40-50%)
Chemotherapy
Supportive Care
MANAGEMENT
29. SURGICAL MANAGEMENT
Surgery with the intention of a cure is only possible in
around one-fifth (20%) of new cases.
Whipple`s procedure
total pancreatectomy
distal pancreatectomy
radiation therapy
chemotherapy
30. WHIPPLE`S PROCEDURE OR RADICAL
PANCREATICODUODENECTOMY
The resection of the proximal pancreas, the
adjoining duodenum, the distal portion of stomach and
the distal segment of common bile duct. An anastamosis
of pancreatic duct, common bile duct, and the stomach
to the jejunum.
32. • Total pancreatectomy – for head of tumor. Sometimes a
simple bypass procedure, such as
cholecystojejunostomy to relieve billiary obstruction.
• Surgery Roux en Y choledochojejunostomy
• Radical resection – Total Pancreaticoduodenectomy With
Spleenectomy
• Billiary stents (cotton – leung stent) for palliative care
when tumors compress the bile duct
SURGICAL MANAGEMENT
34. • Radiation therapy
Internal radiation
External radiation
• Chemotherapy
• It usually consists of gemcitabine either alone or
combination with capecitabine or erlotinib.
MANAGEMENT
35. PROGNOSIS
• Fatal disease 5 year survival after successful surgery
• NOT guarantee of CURE without surgery successful
curative resection (about 20 % patients)
• HEAD and NECK early presentation-obstructive jaundice
better prognosis
• Body and tail late presentation(mass) worse prognosis
36. NURSING MANAGEMENT
Nursing diagnosis
• Acute pain related to obstruction, and inflammation
• Ineffective breathing pattern related to pain secondary to
disease process
• Fluid volume deficit related to vomiting
• Imbalanced nutrition less than body requirement
• Anticipatory Grievingrelated Anticipated loss of
physiological well-being
• Low Self-Esteem related to chemotherapy or
radiotherapy side effects, e.g., loss of
hair, nausea/vomiting, weight loss, anorexia, impotence,
sterility, overwhelming fatigue, uncontrolled pain
37. • Assess the level of pain
• Position patient for comfort, usually in semi-Fowler's
position.
• Provide non pharmacologic methods of pain relief, such
as massage and guided imagery.
• Administer pharmacologic agents, as ordered, to control
pain, considering metabolism through a liver with
decreased function.
– Use caution not to administer doses more frequently
than prescribed.
– Monitor for signs of drug toxicity.
• Assess patient's response to pain control measures.
CONTROLLING PAIN
38. • Assess the patients nutritional status
• Monitor daily weight.
• Encourage patient to eat small meals and to take
supplementary feedings such as Ensure.
• Assess and report changes in factors affecting nutritional
needs: increased body temperature, pain, signs of
infection, stress level. Encourage additional calories as
tolerated.
IMPROVING NUTRITIONAL STATUS
39. • Monitor intake and output chart and weight
• Assess the skin turgor and moisture of mucous
membranes. Note reports of thirst.
• Monitor the electrolyte lavel
• Encourage increased fluid intake to 3000 mL per day as
individually appropriate or tolerated.
• Provide IV fluids as indicated.
NURSING INTERVENTION – RISK FOR FLUID
VOLUME DEFICIT
40. • Assess the patient condition and stage of grief
• Provide open, nonjudgmental environment.
Use therapeutic communication skills of Active-Listening,
acknowledgment
• Encourage verbalization of thoughts or concerns and
accept expressions of sadness, anger, rejection.
Acknowledge normality of these feelings.
• Arrange for care provider and support person to stay
with patient as needed.
• Reinforce teaching regarding disease process and
treatments
NURSING INTERVENTION –
ANTICIPATORY GRIEVING
41. • Chintamani., Lewis., Heitkemper., Dirksen., O’brien and
Bucher. (2011). Lewis’s Medical Surgical Nursing:
Assessment and Management of Clinical Problems. (7th
Ed.) Mosby.
• Black.J.M., Hawks.J.H., & Annabelle.M.K.(2005). Medical
Surgical Nursing – Clinical Management for positive
outcomes. (6th
ed). Mosby.
• Suzanne.C.S., Brenda.G.B.,Hinkel. J.L. &.Cheevar.K.(2015)
.Brunner & Suddarth’s Textbook of Medical Surgical Nursing
(12th
ed). Wolters Kluwer.
• Lippincott Manual of Nursing Practice.(2010). 9th
ed. William
and Wilkins.
REFERENCES






























![Ca pancreas [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/capancreasautosaved-200627065511-thumbnail.jpg?width=560&fit=bounds)













































