













































PRINCIPLES OF DESIGN IN RPD DESIGING UG LEVEL
- 1. PRINCIPLES OF DESIGN IN RPD SARAH PAUL PART TWO
- 2. CONTENTS Introduction Biomechanical considerations Forces acting on the partial denture Factors influencing the magnitude of stresses transmitted to abutment teeth Controlling stress by design considerations Principles of design Philosophy of design
- 3. Biomechanical considerations Machines are classified : simple and complex Complex machines are a combination of simple machines
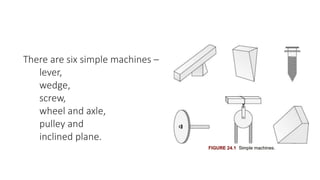
- 4. There are six simple machines – lever, wedge, screw, wheel and axle, pulley and inclined plane.
- 5. The removable partial denture in the mouth performs the action of two simple machines – lever and inclined plane. We have to avoid or reduce the effect of these two machines while designing the prosthesis.
- 6. LEVER Lever is a rigid bar supported somewhere along its length . Support point of the lever is called the fulcrum and lever can move around the fulcrum. There are three classes of levers: class I, II and III
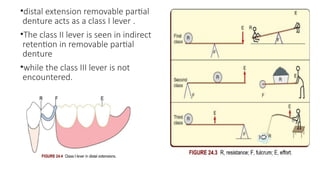
- 7. •distal extension removable partial denture acts as a class I lever . •The class II lever is seen in indirect retention in removable partial denture •while the class III lever is not encountered.
- 8. As downward forces act on the denture base (effort), the clasp (resistance), supported by occlusal rest (fulcrum) tries to come out of the undercut due to rotational forces at the fulcrum. This creates deleterious forces on the abutments and needs to be controlled by our design. This is the most efficient and easily controlled lever.
- 9. INCLINED PLANE The inclined plane effect is typically seen in the movement of minor connectors and direct retainers against the guiding planes, and with occlusal rests and their rest seats, if these are incorrectly prepared. Forces applied in an inclined plane may cause deflection of part applying the force (denture base), or result in movement in the plane itself (abutment tooth) .
- 10. Forces acting on the partial denture The tooth-supported partial denture is rarely subject to rotational stresses. The distal extension prosthesis is subjected to a composite of forces arising from three principal fulcrum lines. HORIZONTAL FULCRUM LINE SAGGITAL FULCRUM LINE VERTICAL FULCRUM LINE
- 11. Horizontal fulcrum line This fulcrum occurs along the horizontal line joining the rests on the two main abutments on either side of the arch Movement around this fulcrum line-sagittal plane Resulting in rotation of the denture base away from or towards the residual ridges. It is difficult to control the movement around this fulcrum line.
- 12. Sagittal fulcrum line This fulcrum extends from the occlusal rest on the terminal abutment along the crest of the alveolar ridge on one side of the arch . In a class I arch, there would be two such fulcrums on either side. Movement around this fulcrum occurs-vertical plane Resulting in rocking or side-to-side movement of denture base. It is easier to control this movement.
- 13. Vertical fulcrum line This is a vertical fulcrum line located in midline, lingual to anterior teeth . It controls rotational movements of the denture in horizontal plane (flat circular movements of the denture).
- 14. Factors influencing the magnitude of stresses transmitted to abutment teeth 1. Length of span 2. Quality of support of ridge 3. Clasp i. Qualities ii. Design iii. Length iv. Material 4. Abutment tooth surface 5. Occlusal harmony
- 15. LENGTH OF SPAN The longer the edentulous span (more missing teeth), greater will be the force transmitted to the abutment teeth. Every effort must be made to preserve posterior teeth so the span length is less.
- 16. Quality of support of ridge Large well-formed ridges : absorbing greater amounts of stress and good stability. Flat ridges give good support but poor stability. Sharp spiny ridge provides poor support and poor to fair stability. Soft, flabby displaceable ridges provide poor support and poor stability . Type of mucoperiosteum also influences the magnitude of stresses transmitted to abutment teeth. Healthy mucosa, 1 mm thick, absorbs forces better than a thin atrophic mucosa.
- 17. Clasp 1. Qualities of clasp 2. Clasp design 3. Length of clasp 4. Material
- 18. QUALITIES OF CLASP GOOD PERIODONTAL SUPPORT - LESS FLEXIBILE CLASP COMPROMISED PERIODONTAL SUPPORT – FLEXIBLE CLASP MORE FLEXIBLE : 1. LESS STRESS TRANSMITTED TO ABUNTMENT 2. LESS RESISTANCE TO HORIZONTAL STRESSES CLASP DESIGN DESIGN SHOULD BE PASSIVE ON COMPLETE SEATING DURING INSERTION AND REMOVAL OF PROSTHESIS THE RECIPROCAL ARM SHOULD CONTACT THE TOOTH BEFORE RETENTIVE TIP PASSES OVER GREATEST BULGE
- 19. LENGTH OF CLASP INVERSELY PROPORTIONAL TO LENGTH MORE FLEXIBLE CLASP – LESS STRESS ON ABUTMENT CLASP LENGTH INCREASED BY USING CURVED PATH RATHER THAN STRAIGHT PATH MATERIAL CHROME ALLOY – MORE RIGID CLASP ARM CHROME ALLOY – SMALL DIAMETER AND ENGAGE SMALL UNDERCUT
- 20. Abutment tooth surface Surface of gold crown or any restoration offers more frictional resistance to clasp arm movement than does the enamel surface of the tooth. Greater stress is exerted on a tooth restored with gold than on a tooth with intact enamel.
- 21. Occlusal harmony A disharmonious occlusion with deflective occlusal contacts transmits destructive horizontal forces to the abutment and ridge. Partial denture constructed opposing a complete denture will be subjected less occlusal stress than one opposed by natural dentition. Occlusal load applied to the distal end of denture base will result in more stress transmitted to the abutment teeth than load applied adjacent to abutment tooth. Ideally masticatory load should be applied in the centre of the denture-bearing area, both anteroposteriorly and buccolingually, i.e. in the second premolar–first molar region .
- 22. Controlling stress by design considerations Every effort must be made to minimize or control these forces through the design of component parts of the prosthesis . INCLUDE DIRECT RETENTION CLASP POSITION INDIRECT RETENTION OCCLUSION DENTURE BASE MAJOR CONNECTOR MINOR CONNECTOR REST
- 23. Direct retention The retentive clasp arm is responsible for transmitting most of the destructive forces to the abutment teeth. Clasp retention should be kept at the minimum yet provide adequate retention to prevent dislodgement of the denture. Other factors should be used to contribute to retention so that the amount of retention provided by clasp can be reduced. The factors are explained as follows: 1. Adhesion and cohesion 2. Atmospheric pressure 3. Frictional control 4. Neuromuscular control
- 24. 1. Adhesion and cohesion : Adhesion is the attraction of unlike molecules for one another – attraction of saliva to the denture on one side and tissues on the other. Cohesion is the attraction of like molecules to each other – internal attraction of molecules of saliva for each other. To obtain the maximum use of forces , the denture base must cover maximum area and must be accurately adapted to the mucosa. 2. Atmospheric pressure : This may also contribute to retention maxillary complete palatal plate major connector posterior margins are sealed by beading.
- 25. 3. Frictional control : Properly prepared guiding planes enable the minor connectors to contribute substantially to retention as a result of frictional contact with adjacent tooth surfaces. Guiding planes should be created on as many teeth as possible. 4. Neuromuscular control : A properly contoured denture base significantly contributes to the ability of the patient to retain the denture through the action of the lips, cheeks and tongue. Any overextension of denture will impinge on the patient’s neuromuscular control and lead to loss of retention and increased stress on abutments.
- 26. Clasp position The position of retentive clasp is more important than the number of retentive clasp used in any design. The number of clasps used and their location is determined by classification. It can be of the following three configurations: 1. Quadrilateral configuration 2. Tripod configuration 3. Bilateral configuration
- 27. 1. Quadrilateral configuration Indicated in class III arches particularly when modification space exists on the opposite side. A retentive clasp is positioned on each abutment tooth adjacent to the edentulous spaces. When no modification space exists, the goal should be to place one clasp as far posterior on the dentulous side as possible and one as far anterior as space and aesthetics permit.
- 28. 2. Tripod configuration Indicated in class II arches. When modification exists, all teeth adjacent to edentulous space are clasped resulting in this configuration . If there is no modification space present, one clasp on the dentulous side of the arch should be positioned as far posterior, and the other, as far anterior as factors such as interocclusal space, retentive undercut and aesthetics will permit .
- 29. 3. Bilateral configuration It is used in class I situations The terminal abutment tooth on each side of the arch must be clasped regardless of where it is positioned. In this configuration, the clasps exert little neutralizing effect on the leverage-induced stresses generated by the denture base.
- 30. Indirect retention It basically assists the direct retainer in preventing displacement of denture away from the tissues by moving the fulcrum farther from the force. In Kennedy’s class I arches, indirect retainer is mandatory. One on each side of arch is placed as far anteriorly as possible .
- 31. In class II arch, it is not critical as anyway the opposite arch will be clasped to make a tripod configuration and the most anterior clasp with its rest will function as indirect retainer . If modification space exists on the opposite arch, the mesial abutment on the tooth- supported side, with its rest and clasp assembly will serve as indirect retainer . If that mesial abutment is not far enough anteriorly, then another rest seat positioned further anterior may be used as indirect retainer .
- 32. In class III, indirect retainer is not necessary as there are no rotational forces. In class IV, the consideration is reverse of class I and II. The indirect retainer is placed as far posteriorly as possible on either side .
- 33. Occlusion Occlusion should be in harmony with movements of temporomandibular joint and neuromusculature to minimize the stress transferred to the abutment teeth and residual ridge. The initial occlusal contact should always be in the remaining natural teeth. Contact of the natural teeth should be same whether denture is in mouth or not. Steep cuspal inclines on the artificial teeth should be avoided because they tend to set up horizontal forces detrimental to the abutment.
- 34. Denture base It should cover maximum area of the supporting tissue as possible and flanges should be as long as possible to help stabilize against horizontal movements. Overextension should be avoided. Distal extension denture base should cover the retromolar area and tuberosity of maxilla as these structures absorb stress better. Accurate adaptation of denture base also lessens movement of the same and reduces stress. Contour of the polished surfaces in harmony with the cheeks, lips and tongue also helps in reducing the stress transmitted.
- 35. Major connector Some major connectors can control stress effectively. In the mandibular arch, the lingual plate major connector properly supported by rests aids in distribution of functional stress. It also supports periodontally weakened anterior teeth. Added rigidity provided by lingual plate also helps in distributing stress created on one side of the arch to the other side – cross-arch stabilization. In the maxillary arch, broad palatal major connector can distribute stress over a large area by covering hard palate and contributing to support, stability and retention of the prosthesis.
- 36. Minor connector Intimate tooth to partial denture contact is brought about by contact of minor connectors with tooth (guiding planes). It offers horizontal stability to partial denture and abutment tooth against lateral forces.
- 37. Rests These control stress by directing forces down the long axis of abutment teeth. Periodontal ligament is better suited to withstand vertical rather than horizontal forces. The floor of rest seat must form an angle less than 90° to the long axis, to hold the tooth in position and to prevent its migration. In distal extensions, the rest seat should be saucer shaped to allow some movement of the rest, so that forces are not transmitted to the abutment .
- 38. Principles of design These principles were developed by A.H. Schmidt in 1956. While designing removable partial dentures, the following instructions should be adhered to: 1. Dentist must have a thorough knowledge of both the mechanical and biologic factors involved in removable partial denture design. 2. The treatment plan must be based on a complete examination and diagnosis of the individual patient. 3. Dentist must correlate the pertinent factors and determine a proper plan of treatment. 4. The prosthesis should restore form and function without injury to the remaining oral structure. 5. A removable prosthesis is a form of treatment and not a cure.
- 39. Philosophy of design The challenge is primarily in designing class I and II arches and to some extent in class IV arches and distributing the forces acting on the removable partial denture between the soft tissues and teeth. There are three philosophies that drive the design process of removable partial denture : 1. Stress equalization 2. Physiologic basing 3. Broad stress distribution
- 40. 1. Stress equalization Resiliency (movement) of the tooth secured by the periodontal ligament in an apical direction is not comparable to the greater resiliency and displaceability of the mucosa covering the edentulous ridge. So if a load was applied to the denture base, the greater movement of the mucosa would cushion the force, while the lesser movement of abutment tooth would generate more stress on the tooth. Type of stress equalizer is needed to replace the rigid connection between denture base and direct retainer and transfer the load from the abutment to the ridge. These are also called stress breakers or articulated prosthesis.
- 41. 1.Stressequalizerhavingamovablejointbetweenthedirectretaineranddenturebase Click icon to add picture They may be hinges, sleeves and cylinders or ball and socket joints. They allow vertical movement and hinge action of the distal extension denture base and help transfer load from the abutment to the ridge. Examples: Dalbo, Crismani and ASC 52 attachments
- 42. 2.Stressequalizerhavingaflexibleconnectionbetweenthedirectretaineranddenturebase. Click icon to add picture They may be wrought wire connectors and divided major connectors .
- 43. ADVANTAGES 1. Minimal direct retention-denture base acts more independently. 2. Minimize tipping forces on abutments-preserving alveolar bone support. 3. Force evenly distributed between abutment and ridge. 4. Intermittent movement of denture base against mucosa has a massaging or stimulating effect on the soft tissues. 5. Splinting-weak teeth. 6. If relining is not done, abutment is not damaged as quickly. DISADVANTAGES 1. Construction complex and costly. 2. Constant maintenance is required and it is difficult or impossible to repair. 3. Vertical and horizontal forces are concentrated on ridge- leads to rapid resorption. 4. If relining is needed but not done- excessive ridge resorption. 5. Effectiveness indirect retainer lost. 6. More food entrapment-joint and spaces. 7. easily distort-not handled properly.
- 44. 2. Physiologic basing The proponents of this theory also believe that there is relative lack of movement in abutment teeth in an apical direction compared to the ridge. They advocated distributing the stress by displacing or depressing the ridge mucosa during the impression making procedure or by relining the denture base after it has been constructed. So when an occlusal load is applied on denture base, it will adapt better and will withstand the force. The tissue surface is recorded in functional form and not anatomic form.
- 45. Prosthesis constructed from tissue displacing impression will be above the plane of occlusion when the denture is not in function. To permit vertical movement from rest position to functional position, the retentive clasps need to have minimum retention and also their number has to be less.
- 46. ADVANTAGES 1. Intermittent base movement has a physiologically stimulating effect on the underlying bone and soft tissue. 2. Less need relining and rebasing. 3. Simple in design and construction with minimal maintenance and repair. 4. The looseness of the clasp on the abutment tooth reduces the functional forces transmitted to the tooth. DISADVANTAGES 1. Denture is not well stabilized against lateral forces. 2. There will be always premature contact when mouth is closed, which is uncomfortable for the patient. 3. It is difficult to produce effective indirect retention
- 47. 3. Broad stress distribution The proponents of this philosophy advocated distributing the forces of occlusion over as many teeth, and as much of the available soft tissue area as possible. This is achieved by means of additional rests, indirect retainers, clasps and broad coverage denture bases. Out of these three philosophies, stress equalization has few advocates. Broad stress distribution is the most widely used philosophy and will be followed in the design procedure.
- 48. ADVANTAGES 1. Teeth can be splinted. 2. Prosthesis is easier and less expensive to construct. 3. No flexible or moving parts so less danger of distorting the denture. 4. Indirect retainers and other rigid components provide excellent horizontal stabilization. 5. Less relining required DISADVANTAGES 1. Greater bulk may cause prosthesis to be less comfortable. 2. Increased amount of tooth coverage can lead to dental caries if oral hygiene is not maintained properly.
- 49. THANK YOU