Introduction to Refractive Eye Surgery
58 likes11,612 views

The document provides an introduction to refractive surgery. It discusses different vision conditions like myopia, hyperopia and presbyopia. It explains how these conditions can be corrected through glasses, contact lenses or refractive surgery options like LASIK and PRK. It addresses common myths about refractive surgery, discussing the safety, effectiveness and long-term outcomes of these procedures.
![INTRODUCTION TO REFRACTIVE SURGERY Dan Z Reinstein MD MA(Cantab) FRCSC DABO FRCOphth London Vision Clinic, London, UK [email_address] General Medical Clinics, 3 rd September 2008](https://image.slidesharecdn.com/reinsteinintrotolasik-100622060016-phpapp01/85/Introduction-to-Refractive-Eye-Surgery-1-320.jpg)




































































































![Thank You Dan Z Reinstein MD MA(Cantab) FRCSC DABO FRCOphth London Vision Clinic, London, UK [email_address]](https://image.slidesharecdn.com/reinsteinintrotolasik-100622060016-phpapp01/85/Introduction-to-Refractive-Eye-Surgery-103-320.jpg)














































Introduction to Refractive Eye Surgery
- 1. INTRODUCTION TO REFRACTIVE SURGERY Dan Z Reinstein MD MA(Cantab) FRCSC DABO FRCOphth London Vision Clinic, London, UK [email_address] General Medical Clinics, 3 rd September 2008
- 2. Why can’t I see well without my glasses?
- 3. Emmetropia: Normal Eyesight Light is focused onto the retina
- 4. Myopia: Short-Sighted Objects in the distance are blurred Objects up close are clear Light is focused in front of the retina
- 5. Myopia: Short-Sighted Objects in the distance are blurred Objects up close are clear The cornea is too steep The eye is too long
- 6. Myopia: Short-Sighted The point of focus needs to be brought back to the retina This is achieved by flattening the centre of the cornea
- 7. Hyperopia: Long-Sighted Objects in the distance are clear Objects up close are blurred The light is focused behind the retina
- 8. Hyperopia: Long-Sighted Objects in the distance are clear Objects up close are blurred The cornea is too flat The eye is too short
- 9. Astigmatism Causes image ghosting Blurring at all distances There are two curvatures so two points of focus
- 10. Presbyopia Presbyopia Long/Short Sighted with Presbyopia Near vision is blurry
- 11. How can I correct my vision?
- 12. How Can I Correct my Vision? Glasses Contact Lenses Refractive Surgery
- 13. Vision with Glasses Distorted peripheral vision Magnification effect Objects appear to be in a different position and have a different size through spectacles lenses
- 14. Vision with Glasses Limited peripheral vision Reduced peripheral vision with glasses Exact prescription only in the centre of the lens As the eye is looking through a different part of the lens, the prescription is no longer optimum (in particular for progressive lenses)
- 15. Risks with Contact Lenses Ocular changes Oedema Neovascularisation Risk of infection Microbial Keratitis Acanthamoeba Incidence of Microbial keratitis per patient/year: 0.04% DW SCL (or 0.8% over 20 years of wear) Risk of permanent visual loss 0.1% for DW SCL over 20 years of wear
- 16. Safety of Contact Lenses Adverse reactions to contact lens wear Dryness CLPC (contact lens papillary conjunctivitis) Autoimmune reaction to SCL CLARE (contact lens acute red eye) Sterile peripheral ulcers Secondary to exotoxins from bacteria = corneal infiltrates Hypoxia (corneal oedema = halos and night glare) Not present with silicone hydrogel for High Dk RGPs lenses but these only account for 10-15% of C/L wearers in the UK Corneal warpage Endothelial cell loss or dysfunction due to chronic oedema
- 17. Risk of Infection and vision loss – Soft Contact Lenses Primary cause of vision loss with soft CLs is MICROBIAL KERATITIS Organisms most commonly associated with microbial keratitis Pseudomonas Staphylococcus Acanthamoeba Fungal (eg aspergillus ) Schein et al 2005 Ophthal Continuous wear soft contact lenses for up to 30 days and nights n=6245, 80% completed 12 mths f/u = 5561 person years WT Microbial Keratitis 18.0 per 10000 (0.18%) With vision loss 3.6 per 10,000 (0.036%) – 1 in 5 !! Risk of MK with Daily Wear soft contact lenses is 1/5 of that with Continuous Wear soft contact lenses > 3 weeks continuous wear MK with vision loss 2.3 per 10,000 (0.023%) MK without vision loss: 0.12% < 3 weeks continuous wear MK with vision loss 7.9 per 10,000 (0.079%) MK without vision loss: 0.4%
- 18. Myths in refractive surgery
- 19. Myths in Refractive Surgery It’s still very new It hurts If you blink or move during the procedure it can go wrong It doesn’t work very well It cannot correct long-sightedness It cannot correct astigmatism It cannot correct the need for reading glasses as you get older – Presbyopia You could end up blind If something goes wrong there is nothing that can be done It doesn’t last very long We don’t know about the long-term safety
- 20. History of refractive surgery It is still very new… Barraquer pioneered surgery in 1960
- 21. Jose Barraquer: Keratomileusis Jose Barraquer invented a new innovative method of vision correction: Keratomileusis
- 22. Jose Barraquer: Keratomileusis Cut and freeze a ~300 µm corneal disc Reshape the corneal disc to reduce myopia: shape change calculated using trigonometry
- 23. Jose Barraquer: Keratomileusis Reshaping achieved using a lathe
- 24. Jose Barraquer: Keratomileusis The corneal disc is sutured back onto the eye
- 25. Jose Barraquer: Keratomileusis Procedure required a very skilled surgeon Took a long time
- 26. Advances: Excimer Laser – 1991 Excimer laser originally funded by IBM for etching computer integrated circuits (1970s) It has moved on considerably into a number of applications since then!
- 27. Advances: Excimer Laser Each pulse penetrates only 1/4 µm from the surface ~ equivalent to 1/200 of a human hair Underlying tissue remains cool
- 28. Photo-Refractive Keratomileusis (PRK) Epithelium is removed using alcohol and a “hockey stick” Excimer laser is used to reshape stromal surface
- 29. Laser In Situ Keratomileusis (LASIK) Corneal flap ~130 µm created using microkeratome or femtosecond laser Flap is lifted, stromal surface is reshaped using excimer laser
- 30. Femtosecond Laser Flap Creation VisuMax (Carl Zeiss Meditec) Bubble layer created, then separated manually Advantages over mechanical microkeratomes More precise Less trauma; patient able to see throughout procedure
- 31. Millions of Procedures Performed 1996-2007: 28,492,590 laser refractive surgery procedures performed worldwide Data courtesy Dave Harmon, Market Scope , Manchester, MO, USA
- 32. Myths in Refractive Surgery It hurts…
- 33. I don’t remember much about the procedure, mainly because it was so quick – less than 10 minutes. It was a similar sensation to when you close your eyes and then press firmly on them Sitting on the edge of the chair, my eyes doused in saline, I could read the vision chart on the wall opposite. When I sat up my first words were, “That’s amazing!”
- 34. Quick Procedure Your time in the clinic is brief and the procedure itself is over in a matter of minutes The procedure is brief and painless
- 35. The procedure is indeed painless The best thing about it is that it is over in about 10 minutes
- 36. The Procedure It does not hurt It is very quick: 10 to 15 minutes in surgery Visual recovery Vision recovers 3 hours after LASIK Back to work the day after surgery One day results: 97% driving standard Staff at London Vision Clinic back to work after 35 minutes!
- 37. Myths in Refractive Surgery If you move …
- 38. Procedure Sophisticated eye trackers follow the eye movements
- 39. Myths in Refractive Surgery It cannot correct long-sightedness It cannot correct astigmatism
- 40. Who Is Suitable? -14.00 D +8.00 D -30.00 D +15.00 D Bioptics: Clear Lens Exchange & LASIK LASIK / PRK 0.00 D 0.00 D
- 41. Who is Suitable?
- 42. Who Is Not Suitable? Some eye conditions Keratoconus Terriens Marginal Degeneration Corneal Herpes Zoster Keratitis Autoimmune corneal melts Some general conditions Severe diabetes with active retinopathy (higher risk of infection and slower healing responses) Uncontrolled active auto-immune disease: Lupus, Rheumatoid Arthritis, etc
- 43. Myths in Refractive Surgery It does not work very well…
- 44. How To Get Good Outcomes
- 45. Myopia Outcomes: up to -12.50 D Binocular Vision (588 patients)
- 46. Myopia: Improved Contrast Sensitivity * * * *
- 47. Better Vision Than Glasses With Glasses Before LASIK Without Glasses After LASIK
- 48. Better Vision Than Glasses 32% of myopic eyes have better vision without glasses after surgery than with glasses before surgery 95.7% of myopic eyes have vision as good or better without glasses after surgery than with glasses before surgery
- 49. Hyperopia Outcomes: up to +7.25 D Binocular Vision (336 Patients)
- 50. Hyperopia: Improved Contrast Sensitivity * *
- 51. Advances: Correcting Wavefront Error Original images from the Hubble telescope were no better than ground-based telescopes Mirror was found to have irregular non-spherical optics (aberrations) causing blurring NASA developed wavefront mirror to correct the aberrations
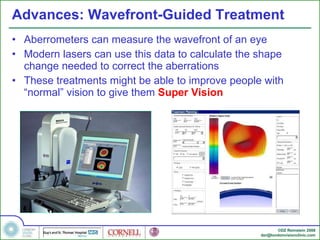
- 52. Advances: Wavefront-Guided Treatment Aberrometers can measure the wavefront of an eye Modern lasers can use this data to calculate the shape change needed to correct the aberrations These treatments might be able to improve people with “normal” vision to give them Super Vision
- 53. Advances: Super Vision Wavefront-guided refractive surgery: Correction of higher order aberrations Glasses or Contact lenses: Correction of lower order aberrations
- 54. Wavefront-Guided Treatment Refraction: -1.50 -0.75 x 163 No Glasses Vision With Glasses Before LASIK Without Glasses After LASIK
- 55. Myths in Refractive Surgery It cannot correct presbyopia
- 56. Current Presbyopic Refractive Surgery Intra-Ocular Lenses Multi-focal Accommodative Laser Refractive Surgery Multi-focal Monovision NEW: Laser Blended Vision
- 57. Problem With Multi-focality ReSTOR ReZoom Near Far Near Far Anschütz,Dausch,Klein,Joly (Meditec group, 1991) Avalos, Rozakis, Agarwal (PARM-technique, 1998) G.Tamayo (2000) Concentric distance near zones Diffraction design PROBLEM: Two Images Multi-focal Ablation Profiles Multi-focal IOLs
- 58. Visualization of Light Path for Multi-focal IOLs 2. Tecnis ZM900 (5 mm pupil) 4. ReZoom NXG1 (5 mm pupil) 5. ReSTOR SA60D3 (5 mm pupil)
- 59. Retinal Image with Multi-focal IOLs 2. Tecnis ZM900 3. Tecnis ZMA00 4. ReZoom NXG1 5. ReSTOR SA60D3
- 60. Optical Performance Multi-focal IOL 3 mm pupil 6 mm pupil ReSTOR ReZoom Tecnis ZM900
- 61. Accommodative Intra-Ocular Lenses Theory: lens movement forward and back replicates accommodation Published studies have shown little lens movement Even with Pilocarpine: max 455 µm would be only 0.50 D of accommodation
- 62. Case Example: Post RLE Pre-op Rx +3.00 D OD, +3.50 D OS No sign of cataract Monovision RLE in 2003 – monofocal lenses Complained of misting vision and felt off balance 3 months post-op, LASIK to correct “off balance feeling” Visual symptoms made worse Diagnosed with PCO in 2006 Bilateral YAG capsulotomies performed No improvement in symptoms
- 63. Case Example: Post RLE Visual Symptoms Constant mist over vision day and night Halos; can’t drive at night
- 64. Case Example: Post CLE 46 yo divorced mother of 2. CLE performed Nov 2006; ReStor IOLs implanted Extremely fatigued eyes and couldn’t drive at night Extreme glare and scattering of head lights ReStor IOLs removed in Jan 2007, replaced with monofocal IOLs – 2.5 hour procedure (bilateral!) Yag capsulotomy in November 2007 Night vision improved Fatigue better but not resolved Foreign body sensation “like a piece of glass in the eye” Distance vision clear, near blurred (absolute presbyopia)
- 65. Case Example: Post CLE
- 66. Case Example: Post CLE Pre-op Rx +5.50 -1.00 x 85 OD, +4.75 -1.50 x 95 OS Bilateral CLE in 2003; accomodating IOLs implanted Severe night vision symptoms Bilateral Yag treatment in 2005 to relieve night vision symptoms Night vision as below after Yag treatment
- 67. Case Example: Post CLE Night vision in 2008 Floaters
- 68. Case Example: Post RLE – OD Elshnig pearls Posterior capsule opacification
- 69. Case Example: Post RLE – OS Elshnig pearls Posterior capsule opacification
- 71. Presbyopia Near Intermediate Distance Far Distance Right Eye Left Eye
- 72. Presbyopia: Ideal Solution Near Intermediate Distance Far Distance Right Eye Left Eye
- 73. Current Possible Depth of Field Increase Near Intermediate Distance Far Distance Right Eye Left Eye
- 74. Laser Blended Vision – Micro-Monovision Near Intermediate Distance Far Distance Dominant Eye Non-Dominant Eye “ Blend Zone”
- 75. Contact Lens Monovision Near Intermediate Distance Far Distance Dominant Eye Non-Dominant Eye “ Blend Zone” “ Blur Zone”
- 76. Correcting Presbyopia: Contact Lens Monovision Dominant eye: mainly corrected for distance Non-dominant eye: mainly corrected for near Brain merges two images to see near and far without glasses ~60% Patients Tolerate
- 77. Correcting Presbyopia: Laser Blended Vision Brain merges two images to see near and far without glasses Dominant eye: mainly corrected for distance Non-dominant eye: mainly corrected for near ~97% Patients Tolerate
- 78. Myopia BV: Efficacy – Binocular Vision Combined Binocular Distance & Near UCVA
- 79. Hyperopia BV: Efficacy – Binocular Vision Combined Binocular Distance & Near UCVA
- 80. Safety and refractive surgery You could end up blind.. If something goes wrong there is nothing that can be done…
- 81. Risks: Surgical Information Pack
- 82. Risks
- 84. Safety: All Risks Combined -8.00 D Preop -8.00 D UCVA Hand movements BSCVA 20/16 Postop Situation 1 UCVA 20/25 (little blurry) BSCVA 20/16 Postop Situation 2 UCVA 20/25 (little blurry) BSCVA 20/25 (lose 2 lines) 0.1% chance Enh to 20/16
- 85. Complication Rate According to CRSQA (Council for Refractive Surgery Quality Assurance), a complication rate of " less than three percent is the norm " among ophthalmic surgeons performing LASIK, or 3 complications over 100 procedures (every eye treated counts as a procedure).
- 86. Complication Rate – Prof Reinstein FLAP COMPLICATIONS Eyes out of 12,977 % Lose 2 Lines Free Cap 1 (0.01%) 0.0000000% Thin Flap 2 (0.02%) 0.0000000% Incomplete Flap (no ablation) 6 (0.05%) 0.0000000% Corneal Perforation 0 (0.00%) 0.0000000% Blindness (total loss of vision) 0 (0.00%) 0.0000000% Corneal scarring reducing vision 0 (0.00%) 0.0000000% Inflammation with decrease of vision 1 (0.01%) 0.0000000% Infection 0 (0.00%) 0.0000000% Epithelial Ingrowth (requiring further surgery) 21 (0.19%) 0.0000000% Need for corneal transplantation 0 (0.00%) 0.0000000% Keratectasia 0 (0.00%) 0.0000000% LASER COMPLICATIONS Eyes out of 12,977 % Lose 2 Lines Visually sig. decentrations 0 (0.00%) 0.0000000% Laser parameter data entry error 3 (0.03%) 0.0000000%
- 87. Routine Post-Operative Management If managed properly, complications do not have to result in loss of BSCVA Routine follow up visits 1 Day 1-3 Weeks 3 Months 6 Months 1 Year Annually More frequent follow ups if required
- 88. Safety: Myopia up to -12.00 D Safety: Lines Change BSCVA
- 89. Safety: Hyperopia up to +7.25 D Safety: Lines Change BSCVA
- 90. Long term safety and refractive surgery Advances in diagnostic tools
- 91. LASIK: The Future LASIK approved for all US Military personnel
- 92. Topography Screening for Keratoconus
- 93. Pentacam Screening for Keratoconus
- 94. Ocular Response Analyzer Measurement of the stiffness of the cornea Could help diagnose keratoconus Normal Keratoconus
- 95. Advances: Artemis Cornell University Bio-Acoustic Lab 1991-1998 Ron Dan
- 96. Advances:“Artemis 2” by Ultralink LLC 50 MHz Arc-Scan Meridional sweep ( 0.4sec) : Whole anterior segment Whole Cornea Scan positional control IR video-image of eye Corneal light-reflex Internal fixation targets Exam time: 3-min per eye www.ArcScan.com FDA 2000
- 97. Artemis - LASIK
- 98. Epithelial Thickness Profile: Normal v Keratoconus Average Epithelium All Eyes – Left Eyes Mirrored Normal (n=110) Keratoconus (n=40) N T N T Thinnest 52 µm 44 µm Thickest 58 µm 62 µm Difference 6 µm 12 µm
- 99. Probability Model of the Inaccuracy of Residual Stromal Thickness Prediction to Reduce the Risk of Ectasia after LASIK
- 100. Long Term Safety: Risk of Ectasia Probability RST <200 µm for an eye with predicted RST of 250 µm Microkeratome Head Mean SD Risk RST<200 µm Allergan Surgical Amadeus 160 µm 181 µm 30.5 µm 18.62% Moria M2 130 µm 124 µm 21.9 µm 1.15% B&L Hansatome 160 µm 128 µm 21.1 µm 0.03% B&L Hansatome zero compression (DZR) 160 µm 124 µm 12.5 µm 0.00002% Carl Zeiss VisuMax femtosecond (DZR) 135 µm 111 µm 7.8 µm 0.00007%
- 101. Conclusions
- 102. Conclusions 29 million LASIK procedures performed worldwide “ LASIK” started in the 1960s Procedure has been refined ~ for a modern expert surgeon, the risk of major visual problem is extremely unlikely 800 years
- 103. Thank You Dan Z Reinstein MD MA(Cantab) FRCSC DABO FRCOphth London Vision Clinic, London, UK [email_address]
- 104. LASIK in Corneal Graft: Pre-Op
- 105. LASIK in Corneal Graft: Post-Op
- 106. Topography Guided LASIK in Corneal Graft Post-Graft 1 Year Post-LASIK Manifest -1.25 -7.00 x 92 -2.75 -1.25 x 120 BSCVA 20/40 20/25+2 UCVA 20/200 20/63-2 Intended -1.50 -1.00 x 92
- 107. Topography Guided LASIK in Corneal Graft Post-Graft 1 Year Ablation Difference Rx -1.25 -7.00 x 92 BSCVA 20/40 UCVA 20/200 Int -1.50 -1.00 x 92 Rx -2.75 -1.25 x 120 BSCVA 20/25+2 UCVA 20/63-2
- 108. What questions should your patient ask to select a skilled surgeon? S afety T echnology E xpertise E xperience R esults “ Do not pass go” – 8 questions
- 109. Do No Pass Go Checklist: Question 1 Question: Did the surgeon undergo formal refractive surgery training and for how long? Expected Answer: You want an eye surgeon that Has had at least 3 months formal training specifically in laser eye surgery. Did 100 procedures under supervision and Has done at least 1000 procedures since training.
- 110. Do No Pass Go Checklist: Question 2 Question: What preoperative examinations, preoperative testing and laser technology do you have? Expected Answer: You want a clinic that provides a dilated pupil exam, dry eye evaluation, contrast sensitivity testing, infrared pupil size measurement, front and back surface corneal topography, ultrasound pachymetry (corneal thickness), and Wavefront analysis. The laser should be able to perform custom treatments and have an eye-tracking device.
- 111. Do No Pass Go Checklist: Question 3 Question: What percentage of patients that present to your practice are turned down for medical reasons? Expected Answer: Should be at least 5% but no more than 20%
- 112. Do No Pass Go Checklist: Question 4 Question: Do you monitor your surgical success rates on an ongoing basis? Expected Answer: Must be YES
- 113. Do No Pass Go Checklist: Question 5 Question: Could you provide me with a table of your personal most recent outcomes (not those of other surgeons) including complication rates Expected Answer: % 20/20 should be at least 75% % eyes losing 2 lines BSCVA no higher than 0.2% shortsight 1.0% longsight
- 114. Do No Pass Go Checklist: Question 6 Question: What is the enhancement rate for all shortsighted (myopic) patients treated by you? What is it for longsighted (hyperopic) patients Expected Answer: Short-sighted ~ 5% Long-sighted ~ 15-20%
- 115. Do No Pass Go Checklist: Question 7 Question: How many procedures have you performed in the last 12 months? Expected Answer: At least 500 per year
- 116. Do No Pass Go Checklist: Question 8 Question: Have you ever had a claim put against you for malpractice in refractive surgery? Have any of these been successful or settled out of court? Expected Answer: No Delicate question but necessary
- 117. Outcomes: Comparison with Spectacles and Contact Lenses
- 118. Safety of Spectacles Spectacles generally protect the eyes but if broken can cause serious injury such as corneal or ocular laceration Increased protection from injury with : Frames : Large wrap around frames or goggles (Sources of injury: UV light, Blunt Trauma, High velocity projectiles (eg metal from grinding wheels) and Chemicals Materials : Polycarbonate CR-39 Toughened Glass Untoughened Glass Decreasing impact resistance
- 119. Vision Correction with Spectacles Many patients aren’t wearing the most accurate prescription in their spectacles Reasons Inaccurate refraction or incorrectly dispensed spectacles Cost of spectacles and/or eyecare Failure to attend annual or biannual routine ophthalmic examinations Reinstein et al 1993 Br J ophthal Study of Px presenting to A&E > 65 year old Screened for “Correctable undetected visual acuity deficit” (CUVAD) with pinhole testing 34% of Patients had a CUVAD
- 120. Safety of Contact Lenses Adverse reactions to contact lens wear Dryness CLPC (contact lens papillary conjunctivitis) Autoimmune reaction to SCL CLARE (contact lens acute red eye) Sterile peripheral ulcers Secondary to exotoxins from bacteria = corneal infiltrates Hypoxia (corneal oedema = halos and night glare) Not present with silicone hydrogel for High Dk RGPs lenses but these only account for 10-15% of C/L wearers in the UK Corneal warpage Endothelial cell loss or dysfunction due to chronic oedema
- 121. Risk of Infection and vision loss – Soft Contact Lenses Primary cause of vision loss with soft CLs is MICROBIAL KERATITIS Organisms most commonly associated with microbial keratitis Pseudomonas Staphylococcus Acanthamoeba Fungal (eg aspergillus ) Schein et al 2005 Ophthal Continuous wear soft contact lenses for up to 30 days and nights n=6245, 80% completed 12 mths f/u = 5561 person years WT Microbial Keratitis 18.0 per 10000 (0.18%) With vision loss 3.6 per 10,000 (0.036%) – 1 in 5 !! Risk of MK with Daily Wear soft contact lenses is 1/5 of that with Continuous Wear soft contact lenses > 3 weeks continuous wear MK with vision loss 2.3 per 10,000 (0.023%) MK without vision loss: 0.12% < 3 weeks continuous wear MK with vision loss 7.9 per 10,000 (0.079%) MK without vision loss: 0.4%
- 122. What does it mean to see well?
- 123. Vision testing Quality of vision is not only being able to read black letters on a white background
- 124. Vision Testing Quality of vision = Visual Acuity Contrast Sensitivity Aberrations = Quality of the optics of the eye
- 125. Vision Testing Good Quality of vision = 1. Good Visual Acuity : small letters on the chart 2. High Contrast Sensitivity 3. Low level of aberrations : Low order aberrations can be corrected with glasses and contact lenses High order aberrations cannot be corrected with glasses and contact lenses
- 126. How can I correct my vision?
- 127. How Can I Correct my Vision? Glasses Contact Lenses Refractive Surgery
- 128. History of Glasses
- 129. Inconvenience with Glasses Can’t see when you wake up Alarm clock Toilet!! Glasses require cleaning Glasses steam up Discomfort Ugly imprint on nose Can’t wear other types of glasses Sunglasses (need clip-on) Swimming goggles Telescopic gun sights
- 130. Inconvenience with Glasses People just don’t look good in glasses!!! Children wearing glasses get bullied!
- 131. Risk with Glasses Losing glasses Glasses can get knocked off Glasses can break Sharp pieces of glasses or lenses may cause injury
- 132. Vision with Glasses Distorted peripheral vision Magnification effect Objects appear to be in a different position and have a different size through spectacles lenses
- 133. Vision with Glasses Limited peripheral vision Reduced peripheral vision with glasses Exact prescription only in the centre of the lens As the eye is looking through a different part of the lens, the prescription is no longer optimum (in particular for progressive lenses)
- 134. Vision with Glasses Riding at night was the most unpleasant because of the glare and ghosting from the glasses Riding in the rain totally smeared the lenses Glasses don’t have full peripheral vision , so you are not fully aware of people coming up behind you
- 135. Inconvenience with Contact Lenses Daily cleaning Risk of losing contact lenses
- 136. Inconvenience with Contact Lenses Discomfort Dehydration Dryness at the end of the day Dry conditions (air conditioning, aeroplane) Dusty, windy conditions
- 137. Vision with Contact Lenses Fluctuating vision with toric contact lenses Decreased quality of vision with bifocal contact lenses Lens rotation
- 138. Risks with Contact Lenses Ocular changes Oedema Neovascularisation Risk of infection Microbial Keratitis Acanthamoeba Incidence of Microbial keratitis per patient/year: 0.04% DW SCL (or 0.8% over 20 years of wear) Risk of permanent visual loss 0.1% for DW SCL over 20 years of wear
- 139. What are the advantages of refractive surgery?
- 140. Convenience for Outdoor Activities
- 141. Golf: Michael Hoey … my vision is probably better than 20/20 and it has made an outrageous difference to me on the golf course I feel I can read greens a lot better I was playing against the best players in the world and I couldn’t see where my ball was finishing
- 142. Sports Vision: Golf Tiger Woods Vijay Singh Phil Mickelson Retief Goosen Ernie Els Official World Golf Rankings (2005) Tiger Woods says that the hole looks bigger and his ability to read greens has improved dramatically Tiger Woods won the first five tour events after having the surgery Then he won the Tiger Slam of four consecutive majors in 2000-01
- 143. Diving If you take part in any water sports and suffer from poor eyesight, the benefits of refractive surgery are enormous Your time in the clinic is brief and the procedure itself is over in a matter of minutes The procedure is brief and painless
- 144. Diving I don’t think it would be exaggerating to call it a life changing moment
- 145. They are the crack gun cops who guard Tony Blair, ready to respond in a split second with a precision shot to rub out anyone deemed to threat his life. Trouble is, some of them don’t exactly have 20/20 vision… Some workers will become more productive following the operation
- 147. Results for the Met Police
- 148. Population 7 officers: 6 myopic patients (short-sighted) and 1 hyperopic patient (long-sighted) Age: 41-56 years Average Distance Vision Average Near Vision Pre op: 20/82 Post op: 20/14.8 Pre op: N12 Post op: N4
- 149. Visual Acuity Improvement Dark blue columns are the vision levels achieved after LASIK Red columns are the level of vision without glasses before LASIK Light blue columns representing the vision of ‘normal’ eyes in the population
Editor's Notes
- #37: Complete 1 day results
- #39: Add picture of eye tracker and speculum
- #47: Not only is the quantity of vision (20/20 etc) improved with the MEL80, but the contrast sensitivity is also slightly improved This is a huge advance from the previous generation lasers where the contrast sensitivity was worse after surgery Refractive surgery is now starting to be able to compete with glasses vision!
- #51: Not only is the quantity of vision (20/20 etc) improved with the MEL80, but the contrast sensitivity is also slightly improved This is a huge advance from the previous generation lasers where the contrast sensitivity was worse after surgery Refractive surgery is now starting to be able to compete with glasses vision!
- #55: This slide demonstrated how higher order aberrations affect the vision Before surgery, the E is very blurry, mainly due to the myopic refraction Once the refraction has been treated, the E is much clearer Once the aberrations have been treated as well, the E is crisp
- #58: Multifocal (and accommodative) intra-ocular lenses have also been designed and are being used
- #72: In presbyopia, the loss of accommodation means that the near vision in both eyes becomes blurred, leaving the patient needing reading glasses.
- #73: The ideal solution would be to increase the depth of field so that both eyes could see clearly at both distance and near.
- #74: So far, the non-linear aspheric profiles have been able to increase the depth of field, but not enough to give the patient clear vision at all distances.
- #75: So, in order to give the patient good reading vision, the non-dominant eye is shifted towards myopia. This results in one eye being clearly focused for distance vision, but only slightly blurred at near, and the other eye being clearly focused for near vision, but only slightly blurred at distance. However, the increased depth of field in each eye means that there is a region where the range of clear vision overlaps – know as a blend zone. The result is that good binocular near and distance vision can be achieved with a lower degree of anisometropia than traditional monovision – which we refer to as micro-monovision. Therefore, much less suppression is required and there is no dissociation between the eyes.
- #76: In traditional monovision, the depth of field in each eye is comparatively smaller, meaning that the near eye needs to be more myopic for the patient to read comfortably, leaving a gap between the range of vision of the two eyes and replaces the “ blend zone ” with a “ blur zone ” .
- #79: 98% of myopic patients could see 20/20 at distance and J5 (newsprint) at near
- #80: 95% of hyperopic patients could see 20/20 at distance and J5 (newsprint) at near
- #87: Update numbers
- #97: The Artemis is commercially available from Ultralink LLC in St Petersburg, FL. It is an FDA approved device, based on 50 MHz ultrasound high-speed arc-scanning that produces high resolution, real-time imaging. It was specifically designed as a refractive surgical tool capable of imaging and measuring the whole anterior segment, or the whole cornea in one scan sweep. Three dimensional data sets can be obtained by multi-meridional scanning. 3D data acquisition takes 3 minutes total per eye. One of it’s major features is infrared eye position control to enable the surgeon to know exactly from where on the eye or cornea a scan plane was taken.
- #98: Legend from publication: Geometrically corrected horizontal B-scans through the visual axis of a cornea before (A above) and 4 months post-LASIK (B - below). The epithelial and posterior corneal boundaries are clearly visualized from one end of the corneal scan to the other, spanning a 9-mm diameter of cornea. Post-LASIK the extra interface produced by the interface between the stromal component of the flap and posterior residual stroma is clearly visualized along it's entire trajectory; The keratome entrance point, with a small separation in the cut ends of Bowman's layer under the epithelium is evident (E); A small irregularity in the smoothness of the keratome track is evident (I); The flap is noted to be thinner (T) nasally than temporally; The keratome track is noted to stop abruptly within the nasal stroma to produce the flap hinge (H).
- #100: In November 2006, we published a probability model for the inaccuracy of RST prediction in the Journal of Refractive Surgery. These papers outline a method to predict the risk of the keratectomy being excessively deep for individual cases and for a population of refractive surgery patients.
- #146: Add article (pdf)
- #147: Add evening standard pic