Sepsis - Process and Scale - Daniels
3 likes1,873 views

1) Sepsis is a life-threatening condition that arises when the body's response to infection causes injury to its own tissues and organs. Left untreated, sepsis can lead to septic shock, multiple organ failure, and death. 2) Early recognition and treatment of sepsis is key to reducing mortality. The "Sepsis Six" bundle of interventions should be completed within one hour for patients with sepsis, including administering oxygen, antibiotics, fluids, and monitoring lactate levels and urine output. 3) Sepsis can cause long-term cognitive and physical impairment in survivors. A study found that 16.8% of severe sepsis survivors had moderate to severe cognitive impairment after recovering.












































Sepsis - Process and Scale - Daniels
- 1. @SepsisUK Sepsis. Process & scale Dr Ron Daniels FFICM FRCA FRCPEd CEO, UK Sepsis Trust CEO, Global Sepsis Alliance
- 11. Iwashyna et al: Long-term cognitive impairment & functional disability among survivors of severe sepsis. JAMA, 2010. 16.8 3.8 6.2 7.1 0 5 10 15 20 Moderate-severe Mild Before sepsis After sepsis Cognitive impairment
- 14. Burns Burns Infection Sepsis Severe Sepsis Septic shock Systemic Inflammatory Organ dysfunction Hypoperfusion Response (SIRS)
- 15. Burns Burns Infection Sepsis Severe Sepsis Septic shock Systemic Inflammatory Organ dysfunction Hypoperfusion Response (SIRS) <1% 10% 30% 50%
- 16. Funk and Kumar Critical Care Clinics 2011 (in press) ‘For each hour’s delay in administering antibiotics, mortality increases by 7.6%’ Septic shock
- 18. Burns Burns Infection Sepsis Severe Sepsis Septic shock Systemic Inflammatory Response (SIRS) <1% 10% 35%
- 21. CVS SBP <90, MAP <70, or SBP decrease >40 SvO2 70% or ScvO2 <65% Cardiac index <3.5 Lmin-1 Decreased capillary refill or mottling Lactate >2 mmolL-1 RS PaO2/FIO2 <300 or SpO2 <90% Renal Urine output <0.5 mLkg-1hr-1 for 2 hrs Creatinine >177 micromolL-1 Hepatic Bilirubin >4 mgdL-1 or >70mmolL-1 Coagulation INR >1.5 or aPTT >60s Platelets <100,000 x 106L-1 GI Ileus
- 22. Prehospital SepsisScreeningandActionTool 1. Areany2of thefollowingpresent? Temperature > 38.30Cor < 360C Respiratoryrate > 20per minute Heart rate > 90per minute Acuteconfusion/ reducedconsciouslevel Glucose > 7.7mmol/l (unlessDM) 3. Isanyredflagpresent? SystolicB.P< 90mmHg Lactate> 2mmol/l Heart rate> 130per minute Respiratoryrate> 25per minute Oxygensaturations< 91% Respondsonlytovoiceor pain/ unresponsive Purpuricrash Sepsisnot present Treat tostandardprotocols RedFlagSepsis Thisisatimecritical condition, immediateactionisrequired. Resuscitation: 250ml bolusescrystalloidtomaximum2000ml (careinCHD) Oxygen15L/minNRB (careinCOPD) Intravenousantibiotics(ifavailable) Recordlactate(ifavailable) Communication: Pre-alert receivinghospital ofRedFlagSepsis Divert totheEmergencyDepartment (or other agreeddestination) Handover presenceofRedFlagSepsis Y Y Y Sepsispresent Transport todesignated destination. Communicatepresenceof sepsisat handover N N N Sepsisisatimecritical condition. Screening, earlyinterventionandimmediatetreatment saveslives. Thistool shouldbeappliedtoall adult patientswhoarenot pregnant whohaveasuspected infectionor their clinical observationsareoutsideofnormal limits 2. Couldthisbeasevereinfection? For example: Pneumonia UrinaryTract Infection Abdominal painor distension Meningitis Cellulitis/ septicarthritis/ infectedwound
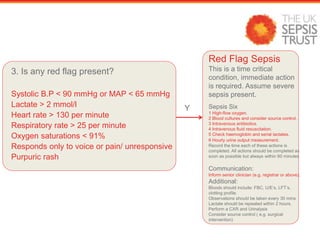
- 23. 3. Is any red flag present? Systolic B.P < 90 mmHg or MAP < 65 mmHg Lactate > 2 mmol/l Heart rate > 130 per minute Respiratory rate > 25 per minute Oxygen saturations < 91% Responds only to voice or pain/ unresponsive Purpuric rash Red Flag Sepsis This is a time critical condition, immediate action is required. Assume severe sepsis present. Sepsis Six 1 High-flow oxygen. 2 Blood cultures and consider source control. 3 Intravenous antibiotics. 4 Intravenous fluid resuscitation. 5 Check haemoglobin and serial lactates. 6 Hourly urine output measurement. Record the time each of these actions is completed. All actions should be completed as soon as possible but always within 60 minutes. Communication: Inform senior clinician (e.g. registrar or above). Additional: Bloods should include: FBC, U/E’s, LFT’s, clotting profile. Observations should be taken every 30 mins Lactate should be repeated within 2 hours. Perform a CXR and Urinalysis Consider source control ( e.g. surgical intervention) Y
- 24. 3. Is any red flag present? Systolic B.P <90 mmHg/MAP <65 mmHg Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
- 28. At least 53% of patients had sepsis prior to arrival in hospital
- 34. The Sepsis Six 1. Give oxygen as needed to target SpO2 > 94% 2. Take blood cultures consider source control 3. Give IV antibiotics according to local protocol 4. Start IV fluid resuscitation Hartmann’s or equivalent 5. Check lactate repeat within 2h 6. Monitor urine output consider catheterisation within one hour ..plus Critical Care support to complete EGDT
- 42. Breast cancer
- 43. Mortality
- 44. Breast cancer
Editor's Notes
- #17: New Insights into Infection Issues in the Canadian ICU Setting - Satellite Symposium Thursday, March 15th, 2007