Strabismus by raju
Download as PPT, PDF56 likes7,897 views

This document discusses the investigation of concomitant and nonconcomitant strabismus. It begins with definitions of strabismus and classifications based on direction of deviation, constancy, and comitance. Non-concomitant or incomitant strabismus is defined as a deviation that changes by more than 10 prism diopters in different gaze positions. Clinical evaluation techniques are described, including cover tests, ocular motility testing, and imaging tests. The force duction test is used to differentiate between paralysis and mechanical restriction as causes of incomitant strabismus. Diplopia charts and Hess screen tests are also used in evaluation.



























































Strabismus by raju
- 1. INVESTIGATION OF CONCOMITANCY AND NONCONCOMITANCY RAju kAITI OpTOMETRIST DhulIkhEl hOSpITAl, kAThMANDu uNIVERSITY hOSpITAl
- 2. DDEEFFIINNIITTIIOONN OOFF SSTTRRAABBIISSMMUUSS SSttrraabbiissmmuuss oorr ssqquuiinntt iiss ddeeffiinneedd aass tthhee ddeevviiaattiioonn oorr mmiissaalliiggnnmmeenntt ooff tthhee eeyyeess.. The term strabismus is derived from a Greek word ” STRABISMOS” , “TO SQUINT,TO LOOK OBLIQUELY OR ASKANCE”
- 3. CCLLAASSSSIIFFIICCAATTIIOONN OOFF SSTTRRAABBIISSMMUUSS SSttrraabbiissmmuuss ccaann bbee ccllaassssiiffiieedd iinn tteerrmmss ooff:: 1.DIRECTION OF DEVIATION - Hyper deviation - Hypo deviation - Divergent - Convergent
- 4. CCLLAASSSSIIFFIICCAATTIIOONN OOFF SSTTRRAABBIISSMMUUSS 22.. CCOONNSSTTAANNCCYY -- ccoonnssttaanntt -- iinntteerrmmiitttteenntt
- 5. CCLLAASSSSIIFFIICCAATTIIOONN OOFF SSTTRRAABBIISSMMUUSS 33.. CCOOMMIITTAANNCCYY -- ccoommiittaanntt // nnoonn--ppaarraallyyttiicc:: Same amplitude of deviation in all gazes Present in case of squint due to oculomotor imbalance -- iinnccoommiittaanntt // ppaarraallyyttiicc:: Amplitude of deviation changes with gaze found in paretic and restricted muscles Concomitant – Latin Word Concomitor: I Accompany (I Attend) : Duane
- 6. • Types 1. Non-concomitant (deviation differ by 10 Pd) 1. Non-paralytic (Special types of Strabismus 2. Paralytic (Paralysis of Cranial Nerve/s)
- 7. Differences: Paralytic (Incomitant) Non-paralytic (Comitant) 1 occurrence less common (15%) more common (85%) 2 onset usually acquired & sudden; usually a sign of neurological or orbital disease; any age usually congenital 3 deviation secondary deviation > primary deviation primary deviation = secondary deviation 4 limitation of movement + -
- 8. Differences:… 5 comitance Only in late stages common 6 diplopia present- homonymous or uncrossed in Esotropia; heteronymous or crossed in Exotropia no diplopia 7 vertigo (nausea or vomiting) present - due to diplopia & false projection absent 8 head posture Commonly abnormal Rarely abnormal 9 false orientation (past-pointing) Common with recent paralysis rare 10 H/O Head Trauma Common Uncommon
- 9. Incomitant deviation • Known as nonconcomitant/non comitant • Strabismic deviation that changes by more than 10pd for a given fixation distance in different directions of gaze • Misalignment of visual axis, marked by asymmetry between one position of gaze and another
- 10. Incomitant deviation ctd.. • May be congenital or acquired • Congenital –hydrocephalus,cerebral palsy, antenatal infections, birth trauma etc • Acquired-after 6 months of age, by trauma,tumour,vascular etiologies
- 11. Clinical Evaluation of Paralytic Strabismus 1. Observation 2. EOM Evaluation 3. Cover Test 4. Measurement of deviation 5. Past Pointing 6. Head tilt Test 7. Diplopia/ Hess Charting 8. Force duction/ Force Generation test 9. Imaging Test (CT/ MRI)
- 12. Examination and Diagnosis 1.Abnormal head posture • To compensate for deviation and to permit BSV • To eliminate diplopia and place eyes in most comfortable position • Three components-face turn/head tilt/chin up and down
- 13. • Patient position the head to reduce the need for affected muscle to contract • Head is placed in the field of action of involved muscle and eye moves out of field of action • Chin elevation for weakness of vertically acting muscles and in A/V pattern
- 14. Head posture: • Face turn -horizontal deviation • Chin elevation or depression –vertical deviation • Head tilt to one or the shoulder –torsional deviation
- 15. • In A/V pattern, to change the size of horizontal deviation in up/down gaze to get fusion and reduce deviation • Head tilt to counteract torsional and vertical diplopia • Not present in amblyopia/suppression • Some patients place head in opposite field to increase the separation between diplopic images
- 16. B.Cover Test • Measure primary and secondary deviation • Head tilt measurement with loose hand held prisms • In recently acquired paretic deviation, secondary angle exceeds the primary angle • In congenital and chronic paretic deviation-similar amount of deviation
- 17. B)cover test: 1. Cover-uncover test: *cover test detects tropia *uncover test detects phoria.
- 19. 2.Alternate cover test measures total deviation(phoria& tropia) 3.prismcover test: measures the actual heterotropia
- 20. Cover Test:
- 21. Cover Test:…
- 23. The Alternate Cover (Cross-Cover) Test:
- 24. C.Tests for Ocular Motility • To detect underactions and overactions • To differentiate paretic from mechanically restricted deviations • Check the ductions and version movements • Head erect with penlight as fixation target • Toy for children
- 25. • See limitation in eye movement that persist despite vigorous encouragement • Abduction/adduction/infraduction should have at least 10 mm of rotation,supraduction of 5-7 mm • Over action and underactions graded from 1 to 4 depending on severity
- 26. Underactions denoted by – sign ,overactions by + sign Each number represents a difference of 25% compared with normal movement - 1=slight(25%)underaction,-4=eye don’t extend beyond midline, +4=good portion of cornea disappears during adduction
- 27. • Ductions testing may not be as effective as version testing, it rules out mechanical restriction but don’t exclude possibility of paresis of EOMs • During ductions with paretic muscle, excessive innervations will flow to that eye, so needed movement actually be made.
- 28. Examination of ocular motility: 1.versions: binocular simultaneous conjugate movement.
- 30. Examination of squint ctd… 1)test for ocular alignment & measurement of deviation. D)corneal light reflex test i)Hirschberg test
- 31. ii)krimsky test: measures the manifest deviation iii)Major amblyoscope: separate target illumination is used which can be moved to centre corneal light reflex.
- 32. E)dissimilar image test : 1. Maddox rod test measures horizontal & vertical deviation.
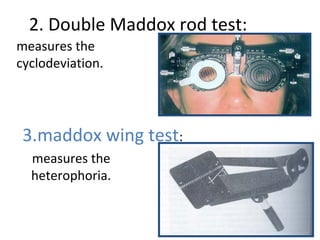
- 33. 2. Double Maddox rod test: measures the cyclodeviation. 3.maddox wing test: measures the heterophoria.
- 35. Synoptophore test : For assessing deviation & quantifying binocular vision. Can also detect suppression & ARC.
- 36. •Bielschowsky Diplopia chart Field of BSV Hess chart
- 37. Instrumentation • Originally to perform this test ,a black cloth 3 feet wide by 3 and half feet long ,marked out by a series of red lines subtending between them an angle of 5 degrees used. • At the zero point of this coordinate system and at each points of interaction of the 15 and 30 degree lines with one another and with corresponding vertical and horizontal lines ,there is red dot . • These dots form an inner square of 8 dots and an outer square of 16 dots
- 38. • The patient wears red –green goggles from which his fusion is dissociated and holds the green flashlight • Fixating eyes sees from red and non-fixating sees from green . • The patient is instructed to place the green light over red light as much as possible. • The examiners marks the position indicated by the patient on the small card with a reduced copy of the screen . • The point found by the patient are connected by straight lines and permit the examiner to determine which ,if any ,muscles react abnormally.
- 39. Performing Hess Screen test
- 40. Hess Screen Chart Additional information: 1. Contraction of ipsilateral antagonist 2. Overaction of contralateral synergist 3. Inhibtion palsy of contralateral antagonist. Diagnosis - Smallest field – Affected eye - Field deviated maximum towards the centre - affected muscle Charts with sloping fields indicate the presence of A and v patterns
- 41. Consequences of EOM Paralysis Ex: LLR Palsy 1. LMR Contract 2. RMR Overaction 3. RLR Under action
- 42. • The right eye is abnormal eye. The limited eye movement is shown by the smaller field . • RLR is underacting LMR is overacting . • Right sixth nerve palsy.
- 44. Look for - Gaze with maximum image separation (affected gaze) - Remote image belongs to affected eye - Image crossed / uncrossed
- 45. Forced duction test Force generation test Palsy Vs Paresis Paralytic Vs Restrictive Pathology Positive in restrictive pathology, negative in paralytic. Tug is appreciated in Restrictive pathology.
- 46. Force duction test • Also known as traction test • Described by wolf ,Gifford and jaensch (1900- 1929). • It is performed to differentiate between the incomitant squint due to paralysis of EOM and that due to mechanical restriction of the ocular movement.
- 47. Force duction test A. No restriction is encountered when rotating the adducted eye into abduction . B. Contracture of MR muscle prevents examiner from the abducting the eye .
- 48. Procedures • Apply several drops of local anesthesia to limbal area of near the insertion of possibly mechanically restricted muscle ,which will be on the opposite side of the possibly paretic muscle. If the lateral rectus muscle ,the anesthesia would be applied near the insertion of medial rectus.
- 49. • The patient is then directed to look at a target that is held in the direction of action of the possible paretic muscle ,which is in the opposite direction of action of the possible mechanically restricted muscle . • If a RLR was the possible paretic muscle ,the patient would be directed to look at a target to the right .
- 50. • The eye is then grasped with toothless forceps near the limbus where the anesthesia was applied .the eye is grasped close to the limbus to get as little conjunctiva as possible in the forceps • An effort is then made to rotate the eye with the forceps in the direction of action of the possible paretic muscle .if the lateral rectus was the possible paretic muscle ,the eye would be grasped at the medial limbus and the rotation attempted would be an abduction movement .
- 51. • if the eye can be rotated with the forceps past the voluntary moved limit –presence of paretic muscle . • FDT is positive in cases of incomitant squint due to mechanical restriction and negative in cases of EOM PALSY.
- 52. Past Pointing • Described by Von Graefe – Anomalies of egocentric localization
- 53. Park’s Bielschowsky Head tilt Test- Park’s Procedure Useful for only Isolated Nerve Palsy Park’s Diagnostic Scheme 1. Which is the hyper eye in primary gaze? – RE/LE 2. Which horizontal field of gaze (right or left) does the hyperdeviation increase? 3. Bielchowsky Head-Tilt Test: Toward which shoulder does the hyperdeviation increase?
- 54. Park’s Procedure
- 55. The 3 step Test Circling Method
- 56. Features of congenital incomitant deviation • Infrequent diplopia • Patients not aware of head posture • Nearly equal primary and secondary angle of deviation • Amblyopia and suppression may be present • Mild limitation of ocular movement
- 57. Recently acquired incomitant deviation. • Frequent diplopia • Patients aware of head posture • Significant difference in primary and secondary angle of deviation • Absence of Amblyopia and suppression • Severe limitation of ocular movement
- 58. Investigations: Diagnosis of strabismus is mainly clinical, if any neurological abnormality is suspected than we go for CT Scan,MRI and neurosurgical consultation.. Conclusion: Early diagnosis and management is essential for eliminating the effect of most difficult conditions -amblyopia or constant strabismus. Treatment under 6 years of age is ideal and allows better result.
- 59. References • Practical orthoptics (5th edition) – T. keith Lyle • Binocular vision and ocular motility – Gunter K. Von Noorden • Clinical Management of Strasbismus – Elizabeth E. Caloroso • Pediatric ophthalmology and strabismus- AAO section 6 • Internet
- 60. …..THANK YOU