







































TEF PPT
- 1. CASE PRESENTATION ON TEF(Tracheoesophageal fistula) SANDEEP KAUR M.Sc. 1st year PAEDIATRIC NURSING
- 2. BIODATA OF THE PATIENT Name: Kaka Kirpal singh Age/sex: 3 days/male Father’s name: Kirpal singh Mother’s name: Gurwinder kaur Occupation of parents: Shopkeeper M.R.D no.:1933536 D.O.B: 31 march 2018 Doctor incharge: Dr. Karuna thapar & Gurpreet singh Diagnosis: Tracheo oesophageal fistula Informant: Father and written records Birth Weight: 2.7 kg
- 3. CHIEF COMPLAINTS: • Nasal flaring, difficulty in breathing since birth • Choking and cyanosis
- 4. HISTORY OF PRESENT ILLNESS • Baby is born through LSCS delivery. • Mother observes when baby take feed turns blue and difficulty in breathing. • After that they came into this hospital and diagnosed with TEF
- 5. HISTORY OF PAST ILLNESS • No H/O pulmonary HTN, TB, DM
- 6. PAST SURGICAL HISTORY. • No past surgical history in patient
- 7. PRESENT SURGICAL HISTORY • TEF is repaired on 2/4/18 by Dr. Pardeep Bhatia. • Premedication glycol 0.02 • Tramadol 6mg is given • Induction: Propofol 3mg + atracurium 1.5mg, ET tube fixed at 8.5cm, oxygen and nitrogen oxide is given. • Pulse rate at duration was up to 154-170 • SpO2 was 100% • I/V fluids 10% dextrose+ inj. Paracip 30mg was given
- 8. FAMILY HISTORY • Type of family: Joint • No. Of family members: 5 • Any illness in the family: H/O Hypothyroidism in mother and she is taking tab. Thyronorm 2.5mg. No H/O HTN, DM, TB, Epilepsy in family
- 9. HEALTH FACILITY NEAR HOME • TYPE: PHC • DISTANCE:7km • TRANSPORTATION: own
- 10. HOUSING • Type of house: Pucca • No. Of rooms: 6 • Toilet facility: Present • Electricity: good • Drinking water: RO
- 11. BIRTH HISTORY • Gestational history: or antenatal history • T1: -Spontaneous conception Urine pregnancy test is positive No H/O fever in mother • T2: - Two doses of tetanus are given to mother Folic acid is taken by mother H/O Hypothyroidism is present. • T3 : - Uneventful
- 12. CONT... • Intranatal history: - baby is term and delivered by LSCS in breech presentation. -Cries immediately after birth -Cord is cut and clamped -Vit. K was given -Oronasal suction is done
- 13. CONT... • Postnatal history:Apgar score was @ 1min: 7/10 @ 5min : 9/10 • Birth order: 4 • Mode of delivery: LSCS • Place of delivery: Local private hospital • Gestational age: 37 completed weeks • Birth weight: 2.7 kg • Condition at birth: normal
- 14. DEVELOPMENTAL MILESTONES • Baby has good sucking and routing reflex. • Good grasp reflex.
- 15. DIETARY HISTORY • Breastfeeding: expressed breast milk is giving by NG • Weaning: no • Present diet: NG tube feeding
- 16. IMMUNIZATION HISTORY • Vit. K is given at birth • BCG is given • Polio drops are given
- 17. PHYSICAL EXAMINATION • SKIN COLOUR: pinkish body and extremities • POSTURE: normal • GAIT: normal • BLEEDING/DISCHARGE: no • HAIR: Black and shiny • EYE/ENT: -normal symmetry in eyes -No any discharge from eyes and ears and nose Pupil B/L reactive to light. • Body build: thin • Emotional state: normal • Foul body odor: absent • Foul breath: absent
- 18. CONT.. • TEETH AND GUMS: teeth are not present and gums are pink and normal • ORAL MUCOSA: good condition • GLANDS: no any lymph nodes are present • CHEST: -B/L air entry equal -B/L symmetrical chest size. -No retractions • ABDOMEN: -soft Non distended No organomegaly • TOES AND NAILS: Nails are grown up to finger tips • DEPENDENCY LEVEL: baby is on ventilator on SIMV mode
- 19. Vital signs Normal values 31-3-2018 1-4-2018 2-4-2018 Temperature 98.6°F 98.7º 100ºF 98.6ºF Respiration rate 30-60bpm 64bpm 74bpm 74bpm Heart rate 120-160bpm 156bpm 150bpm 140bpm VITAL SIGNS
- 20. Lab Investigation TEST 31/3/18 1/4/18 2/4/18 NORMAL RANGE REMAR KS -Hb -RBC -PCV -MCV -MCH -MCHC -Platelet count -Serum Ca - CRP - Random plasma Sugar - TLC - DLC Neutrophills lymphocytes Monocytes eosinophills 15.7gm% 4.98 48.4 97.2fl 31.5pg 32.4/dl 2.67 9.0 1.33 205 22,300 75 18 02 05 15.3 - 44.3 - - - - - - - - - - - - 15.0gm% - 48.2 97.4 31.5pg 32.4/dl 2.8 7.6 0.2mg/dl - 14,700 85 10 02 03 12-16gm% 5.1-5.3million 42-64% 95-125fl 27-33picogram 33-36gm/dl 2% 7.5-8.5mg/dl 1.8-.4mg/dl 74-140mg/dl 4000-11000/cum 50-70% 20-40% 2-10% 1-6% decreased decreased normal normal normal increased increased normal normal increased Increased increased
- 21. -Serum creatinine - serum sodium -Total bilirubin -Direct bilirubin -Serum potassium -PTI -CONTROL -TEST -INDEX -INR -Blood urea nitrogen -CRP Quantitative 0.58 - - - 3.9 - - - - - - - 134mmol/l 6.3 0.19 4.4 14sec 16sec 87.5% 1.1 - - 0.35mg/dl 132mmol/l 7.9 - - - - - - 6 0.2mg/dl 0.6- 136-145 0.2-1.0mg/dl 0.0- 0.20mg/dl 3.5- 5.1mmol/l 15-17sec 93.3-82.3% 7-18mg/dl 1.8-2.4mg/dl Normal Normal Increased Normal Normal Decrease d Decrease d decreased
- 22. MEDICATION DRUG DOSE ROUTE TIME ACTION -inj. Amikacin -Inj. Pipzo(piperacill in and tazobactum -IVF+Ca gluconate -Syrup Ostocalcium 40mg 200mg 75ml+2.5cc 5ml I/V I/V I/V NG OD for 8 days 8Hrly 8Hrly TDS Antibiotic Antibiotic Mineral supplement Mineral
- 24. TEF
- 25. INTRODUCTION Congenital atresia of the oesophagus and tracheoesophageal fistula are rare malformation that results from failed separation of the oesophagus and trachea by the fourth week of gestation. These defects are occur as separate entities or in combination. They have a fatal outcome without early diagnosis and treatment. TEF and oesophageal atresia are malformation of digestive system, in which oesophagus doesn’t develop properly. The oesophagus is a tube that normally caries a food from mouth to stomach. These disorders are commonly found among premature or LBW infants and mothers having polyhydroamnios. Its incidence is 1 in 3500 live birth.
- 26. DEFINITION • A Tracheoesophageal fistula (TEF) is an abnormal connection (fistula) between the Oesophagus and the trachea. TEF is a common congenital abnormality. • Oesophageal atresia is failure of oesophagus to form a continuous passage from the pharynx to the stomach and • TEF is an abnormal connection between the trachea and the oesophagus
- 27. CAUSES IN BOOK IN PATIENT -History of maternal polyhydroamnios -TEF present with VACTERL syndromes Acronym vertebral, anorectal, cardiovascular, tracheoesophageal, renal and limb abnormality. -With cardiac and renal anomalies. -Teratogenic stimuli -Genetic factors Absent Absent Absent Present absent
- 28. CLASSIFICATION TYPE 1: EA without fistula (8%) It is second most common type. There is no connection of oesophagus to trachea. The upper segment and lower segment of oesophagus are blind
- 29. Cont.. • TYPE 2: EA with TEF. It is rare and found in less than 1% of all cases. Upper segment of oesophagus is open into trachea by a fistula. The distal or lower segment is blind.
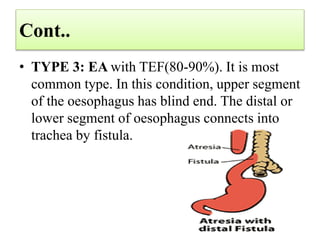
- 30. Cont.. • TYPE 3: EA with TEF(80-90%). It is most common type. In this condition, upper segment of the oesophagus has blind end. The distal or lower segment of oesophagus connects into trachea by fistula.
- 31. Cont.. • TYPE 4: EA with TEF both upper and lower segment. it is also rare(less than 1%). There is EA with fistula between both upper and lower ends of the trachea and oesophagus.
- 32. Cont.. • TYPE 5: H-Type TEF. It is found in about 4% of all cases and not usually diagnosed at birth. Both upper and lower segment of the oesophagus open into the trachea by a fistula. No EA is present.
- 33. PATHOPHYSIOLOGY • In intrauterine life, during the 4th and 5th week of gestation period the foregut normally lengthens and separate longitudinally and each longitudinal portion fuses to form two parallel tubes, the trachea and the oesophagus, which are joined at the larynx. The abnormality of the trachea- esophagus occurs due to defective separation , incomplete fusion of the tracheal folds or abnormal cellular growth during the development of child.
- 34. CLINICAL MANIFESTATION IN BOOK IN PATIENT •Excessive salvation •Constant drooling •Large amount of secretions from mouth •Coughing •Gagging •Choking •Cyanosis •After first feed during first and second swallow the infant coughs , chokes or fluid returns through nose and mouth •Abdominal distension •Apnoea Present Present Present Present Present Present Present Present Absent Absent
- 35. DIAGNOSTIC EVALUATION IN BOOK IN PATIENT -USG -Chest X-ray -Passing radio opaque catheter through oesophagus and conforming the anomaly by X-Ray -Bronchoscopy -ECG NOT DONE DONE DONE NOT DONE NOT DONE
- 36. CHEST X-RAY
- 37. MANAGEMENT(IMMEDIATE) IN BOOK IN PATIENT Nothing per mouth 30° position to prevent reflux of gastric secretions NG Tube aspiration NG tube to be kept in situ Oxygen therapy I/V Fluid therapy Blind pouch to be washed with NS Gastrostomy Prevention of infection Antibiotic therapy Respiratory support Continuous monitoring of patient Chest physiotherapy Postural drainage
- 39. SURGICAL MANAGEMENT IN BOOK IN PATIENT •Postereolateral thoracotomy followed by intercostal chest drainage •Gastrostomy is done in initial stage followed by oesophageal anastomosis DONE DONE
- 40. NURSING MANAGEMENT • Assess the vital signs of the patient continuously including pulse oximetery. • Assess the colour of the child. • Assess the family coping strategy and after explanation at the time. • Written consent was taken by the family member. • Ensure adequate nutrition. • Monitor fluid intake and output chart. • Strict vital monitoring. • Provide information to family before discharge about; • how to manage the temperature of the child. • Encourage the mother to give breast feeding to the child. • Follow up.
- 41. NURSING DIAGNOSIS • Ineffective airway clearance related to disease process as evidence by surgery. • Risk of infection related to surgical incision and long stay in the hospital as evidenced by fever. • Impaired nutrition related to surgery as evidenced by patient is on ventilator. • Fluid volume deficit as evidence by the nil oral intake and less and less output. • Knowledge deficit related to disease condition as evidence by doubtful questioning by family members