uterus.ppt

The document discusses the normal structure and function of the uterus, as well as several uterine disorders including dysfunctional uterine bleeding, endometriosis, adenomyosis, endometrial hyperplasia, and endometrial carcinoma. It provides details on the etiology, pathogenesis, morphology, clinical features, and staging of these conditions. Key points include that the uterus contains a myometrium and endometrium, and the endometrium undergoes monthly changes regulated by hormones. Dysfunctional uterine bleeding is abnormal bleeding without structural abnormalities caused by hormonal disturbances. Endometriosis and adenomyosis involve the presence of endometrial tissue outside or within the uterus, respectively. Endometrial hyperplasia and




































uterus.ppt
- 2. Normal Uterus Normal Structure Myometrium – smooth muscle Endometrium – endometrial glands and stroma, glands lined by columnar epithelium Normal function Endometrium is stimulated by hormones (estrogen, progesterone) Proliferative phase Secretory phase Menstrual phase
- 3. Menstrual phase(day1-5) Shedding of upper 12 to 23rd of the endometrium Proliferative phase (6-14d) Straight round to oval, tubular glands Lined by regular, tall, pseudostratified columnar cells Stroma is dense & compact with spindle cells
- 4. Secretory phase (15-28day) Glands are tortuous, serrated/saw toothed Secretions in the lumen Cells show vacuolation Stromal changes – Edema & Increase in ground substance Spiral arterioles Predecidual change (Cytoplasmic eosinophilia)
- 5. FUNCTONAL ENDOMETRIAL DISORDERS Dysfunctional Uterine Bleeding (DUB) Abnormal uterine bleeding(AUB) without any organic (structural ) abnormalities but due to hormonal disturbances. Etiology: Prepuberty - Precocious puberty (hypothalamic, pituitary, or ovarian origin) Adolescence -Anovulation, coagulopathy Reproductive age – Anovulation, inadequate luteal phase Perimenopausal – Anovulation, atrophy
- 6. Etiopathogenesis: Most common cause - Anovulatory cycle Lack of ovulation is the result of – Endocrine disorder (Pituitary, thyroid, Adrenal) Primary lesions of ovary - Granulosa cell tumors or polycystic ovaries (produce excess estrogen) Generalized metabolic disorder – obesity (estrogen production from fat by steroidogenic enzymes) Results in excessive & prolonged estrogenic effects without the development of progestational phase
- 7. ENDOMETRIOSIS & ADENOMYOSIS ENDOMETRIOSIS The presence of endometrial glands or stroma in abnormal locations outside the uterus. Sites in the descending order of frequency – Ovaries Uterine ligament , Rectovaginal septum Pelvic peritoneum , Laparotomy scars Rarely in umbilicus , vagina or appendix ADENOMYOSIS The presence of endometrial tissue in the myometrium.
- 8. Theories regarding origin of the endometriosis- The regurgitationimplantation theory- Retrograde flow of menstrual endometrium The metaplastic theory- Endometrial tissue arise from coelomic epithelium The benign metastases theory – Vascular or lymphatic dissemination – endometriosis in lungs or lymph nodes The extrauterine stem/progenitor cell theory- Bone marrow stem cells differentiate into endometrial cells
- 9. Additional insights of endometriosis based on molecular analysis Release of proinflammatory factors – stimulate local synthesis of estrogen Increased aromatase enzyme in stromal cells–increased estrogen production (Aromatose is absent in normal stroma) Epigenetic alterations - increase responsiveness to estrogen & decreased responsiveness to progesterone Mutations in genes (PTEN and ARID1A) in endometriotic cysts, atypical endometriosis associated carcinoma (endometroid carcinoma) These abnormalities are present not only in ectopic endometriotic tissue, but also in normal endometrium.
- 10. Gross Morphology ENDOMETRIOSIS- The foci of endometriosis responds to hormonal stimulation - periodic bleeding – red-blue, yellow-brown, black appearance, situated just beneath the mucosal or serosal surface of involved organ. Advanced disease - fibrous adhesions. Endometriotic Ovary – uni/bilateral, distorted, with large cystic masses filled with brown blood debris (chocolate cysts) or endometriomas. ADENOMYOSIS- enlarged uterus with coarsely trabecular, ill defined hemorrhagic areas within myometrium.
- 11. Microscopic examination Endometriosis- Endometrial glands and stroma. Hemorrhage, hemosiderin laden macrophages. Surrounding inflammation and fibrosis. Atypical endometriosis – Premalignant. Adenomyosis – Presence of endometrial glands and stroma within myometrium separated from basalis by at least 2-3mm( 1 LPF below). Sometimes only stroma is seen – Stromal adenomyosis. Adenomyoma – Circumscribed mass of smooth muscle tissue(leiomyoma) with adenomyosis.
- 13. adenomyosis
- 14. ENDOMETRIOSIS
- 15. ENDOMETRIAL HYPERPLASIA Increased proliferation of the endometrial glands relative to the stroma, resulting in an increased gland to-stroma ratio. Etiopathogenesis Prolonged unopposed estrogen stimulation - by anovulation or increased estrogen production as in Obesity (peripheral conversion of androgens to estrogens) Menopause - Prolonged administration of estrogenic substances (estrogen replacement therapy) Polycystic ovarian syndrome, cortical stromal hyperplasia Functioning granulosa cell tumors of the ovary Inactivation of the PTEN (tumor suppressor gene) - endometrial cells become more sensitive to estrogenic stimulation - endometrial hyperplasia - cancer
- 16. Morphology In recent past, most widely used system : 4 categories 1. Simple hyperplasia without atypia; 2. Complex hyperplasia without atypia; 3. Simple hyperplasia with atypia; 4. Complex hyperplasia with atypia. The most current WHO classification: 2 major groups- 1. Non-atypical hyperplasia and 2. Atypical hyperplasia (Endometrial intraepithelial neoplasia)
- 17. ENDOMETRIAL HYPERPLASIA- WHO Classification Non-atypical hyperplasia Increased gland to stroma ratio without nuclear atypia. Simple hyperplasia : Glands - various sizes, shapes & cystic alterations Complex hyperplasia: Complexity of gland architecture - papillary infolds or out-pouchings, crowding
- 18. Atypical hyperplasia (Endometrial intraepithelial neoplasia) Increased gland to stroma ratio with cytological & architectural atypia. Complex patterns of proliferating glands - Gland enlargement, crowding, Back-to-back arrangement and branching. Nuclear atypia – vesicular chromatin, nucleoli. 23% to 48% of women with a diagnosis of atypical hyperplasia are found to have carcinoma when a hysterectomy is performed.
- 20. TUMORS OF ENDOMETRIUM Tumors of endometrial glands Endometrioid carcinoma Serous carcinoma Clear cell carcinoma/ mucinous carcinoma Tumors of endometrium with stromal differentiation Mixed Malignant Mullerian Tumor (MMMT) or Carcinosarcoma–malignancy of both glands & stroma Adenosarcoma- benign glands with stromal malignancy Pure stromal neoplasms Benign - stromal nodule Malignant - stromal sarcoma
- 21. Endometrial carcinoma Characteristics Type I Type II Age 55 – 65 yrs 65 - 75 yrs Clinical setting Unopposed estrogen, obesity, HTN, DM Atrophy, thin physique Morphology Endometrioid ca Serous ca, Clear cell ca, Mixed Mullerian tumor Precursor Hyperplasia Serous endometrial intraepithelial carcinoma Mutations PTEN, ARID1A, PIK3CA, KRAS, MSI, B-catenin TP53 Aneuploidy Behaviour Indolent Spread via lymphatics Aggressive, Intraperitoneal spread, lymphatic spread
- 22. ENDOMETRIOD CARCINOMA(Type-I) Accounts for 7% of all invasive cancer in women Peak incidence in the 55-65yrs Etiopathogenesis Stepwise acquisition of several genetic alterations PI3K/AKT pathway – hallmark of endometrioid ca Muatations in PTEN(tumor suppressor gene) occurs before invasion(Non atypical hyperplasia)- DNA mismatch repair mutations/microsatellite instability - HNPCC syndrome, KRAS mutations(Atypical hyperplasia)- PIK3CA(oncogene)(39%), B- catenin mutation– increase PI3K/AKT signaling cause invasion(Endometroid carcinoma). Loss of function/ mutation in ARID1A – also found in endometroid CA.
- 24. Gross morphology Grossly 2 types- Localized polypoid tumor. Diffuse tumor involving entire endometrial surface. Spread by direct continuity, to myometrium, other adjacent structures. Dissemination to regional lymph nodes & ultimately distant metastasis - lungs, liver, bones.
- 25. Microscopic examination Adenocarcinoma( characterized by gland patterns resembling normal endometrial epithelium) - 3 step grading system Grade I - well differentiated – composed entirely of well formed glands without intervening stroma. Grade II - moderately differentiated – well formed glands mixed with solid sheets (upto 50% tumor area) of malignant cells. Grade III - poorly differentiated – more than 50% solid sheets of cells with barely recognizable glands. Upto 20% of carcinomas have squamous differentiation.
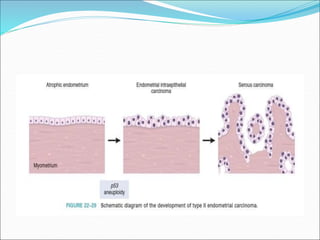
- 27. Type II endometrial CA Women are older- 65 to 75 yrs. Setting of endometrial atrophy. Poorly differentiated- grade 3. Most common type is serous. Other types are clear cell, MMMT. TP53 mutations in over 90% cases.
- 28. Precursor lesion- serous endometrial intraepithelial carcinoma. Poorer prognosis is due to the propensity to exfoliate. Travel to the fallopian tubes, implant on peritoneal surfaces.
- 30. Morphology- Gross- Arise in small atrophic uteri. They are large bulky tumors, deeply invasive. M/E- Papillary growth pattern or glandular. Cells having marked cytologic atypia. High N-C ratio, hyperchromasia, atypical mitoses, prominent nucleoli.
- 32. Clinical features Postmenopausal women. May be asymptomatic for a period of time. Postmenopausal bleeding. Prognosis depends on stage, grade, subtype.
- 33. MMMT Aka carcinosarcoma. They are endometrial carcinomas with a malignant mesenchymal component. Gross: Fleshier than adenocarcinoma, may be bulky and polypoid, and protrude through cervical os. M/E: Composed of adenocarcinoma (endometrioid, serous, clear cell) mixed with malignant mesenchymal (sarcomatous) elements.
- 35. Staging of endometrial carcinoma Stage I- carcinoma confined to uterine corpus Ia - < 50% myometrial invasion Ib - >50% myometrial invasion Stage II- carcinoma has involved the corpus & the cervix Stage III- carcinoma has extended outside the uterus but not outside the true pelvis Stage IV- carcinoma has extended outside the true pelvis or has involved the bladder or rectum
- 36. Staging of endometrial carcinoma