

![JSS Medical College, Mysuru
Introduction
• Hip USG was the first and most successful application of USG
in the musculoskeletal system.
• Dr. Graf was the first to realize the potential of USG.
• Real-time and multiplanar USG evaluation of the hip was
introduced soon thereafter by Novick G[2] and Harcke et al.
• The sensitivity and specificity of USG for the diagnosis of hip
dysplasia is nearly 100%.](https://image.slidesharecdn.com/vishwajcppt-190531070520/85/Hip-ultrasonography-in-infants-and-children-3-320.jpg)












































Hip ultrasonography in infants and children
- 1. JSS Medical College, Mysuru Hip ultrasonography in infants and children Alka Karnik Dr. B Nanavati Hospital and Research Center, Sonosight Imaging Centre, Mumbai, India Authors: Journal: Presenter Dr.Vishwanath Patil PG Resident Moderator Dr. Vinay Raj Senior Resident • Indian J Radiol Imaging / November 2007 / Vol 17 / Issue 4
- 2. JSS Medical College, Mysuru Outline • Introduction • Developmental dysplasia of the hip • Examination technique • Graf’s Technique
- 3. JSS Medical College, Mysuru Introduction • Hip USG was the first and most successful application of USG in the musculoskeletal system. • Dr. Graf was the first to realize the potential of USG. • Real-time and multiplanar USG evaluation of the hip was introduced soon thereafter by Novick G[2] and Harcke et al. • The sensitivity and specificity of USG for the diagnosis of hip dysplasia is nearly 100%.
- 4. JSS Medical College, Mysuru Introduction • The older child, once the ossification nucleus in the head is well-formed, adequate USG imaging of the acetabulum becomes difficult.
- 5. JSS Medical College, Mysuru Introduction • USG of the hip is thus practical only up to 1 year of age, unless there is delayed ossification of the femoral head. • Draw backs 1. operator-dependent modality with a significant learning curve. 2. USG waves do not penetrate bony structures adequately. • Due to the presence of physiologic laxity, imaging is usually not performed on patients less than 2 weeks old.
- 6. JSS Medical College, Mysuru Developmental dysplasia of the hip • DDH is a common disorder the affects 0.8% to 3.5% of children. • It occurs more oft en in girls and usually involves the left hip. • Universal screening of all infants or of all female infants, have shown a higher rate of diagnosis of DDH by USG. • Carry the burden of significantly increased follow-up costs
- 7. JSS Medical College, Mysuru Developmental dysplasia of the hip • USG as a screening test is currently limited to infants at risk for DDH. • Breech presentation. • Family history of DDH. • club foot. • congenital torticollis and metatarsus adductus. • All infants with a positive physical examination should be imaged.
- 8. JSS Medical College, Mysuru Pathophysiology of DDH • Two major components 1. Instability . 2. Abnormal morphology.
- 9. JSS Medical College, Mysuru Pathophysiology of DDH • Ligamentous instability • Malposition of the femoral head out of the acetabulum • Femoral head becomes flattened postero-laterally. • Absence of the femoral head leads to a shallow and dysplastic acetabulum. • The capsule thickens and the labrum hypertrophies
- 10. JSS Medical College, Mysuru Pathophysiology of DDH • The space between the femoral head and acetabulum becomes filled with fibro-fatty tissue (pulvinar). • The femoral head moves further supero-laterally, the labrum is inverted and is deformed • The capsule thickens and may develop an hourglass deformity
- 11. JSS Medical College, Mysuru Pathophysiology of DDH • General consensus is that any diagnosis after the age of three months, is a late diagnosis. • Röntgenogramme for hip dysplasia becomes more reliable after appearance of the proximal epiphysis of the femur.
- 12. JSS Medical College, Mysuru Examination technique • Imaging is conducted with a linear transducer. • Sector probe-evaluation through small windows in a plaster cast during treatment. • Two distinct methods of examination • Static method introduced Dynamic method by Graf described by Harcke et al
- 13. JSS Medical College, Mysuru Graf’s Technique • The child is placed in a foam-padded trough in a lateral position and the hip is flexed to 90°. • The ultrasound probe is placed in a coronal plane parallel to the spine and a coronal section is obtained though the middle of the acetabular roof.
- 14. JSS Medical College, Mysuru Graf’s Technique • Standard plane is identified by the presence of the following three points. 1. Lower limb of the bony ilium, in the depth of the acetabular fossa. 2. The middle of the acetabular roof 3. The acetabular labrum
- 15. JSS Medical College, Mysuru Anatomical structures of the infant hip (as seen on coronal ultrasonography). 1, ossified external wall of ilium; 2, psoas muscle; 3, labrum; 4, lower limb of the os ilium; 5, triradiate cartilage; 6, Synovial fold; 7, chondro-osseous junction at the femoral neck, 8, greater trochanter.
- 16. JSS Medical College, Mysuru Graf’s Technique • A line is drawn parallel to the ossified lateral wall of the ilium (baseline). • A second line is drawn along the roof of the cartilaginous acetabulum to give the beta angle. • A third line is drawn from the inferior edge of the bony acetabulum, at the triradiate cartilage, to the distal part of the ilium, tangential to the slope of the bony acetabulum (roof line).
- 17. JSS Medical College, Mysuru Graf’s Technique Measurements made on this coronal view are the alpha and beta angles. • The alpha angle denotes the slope of the bony acetabulum. • Beta angle denotes the slope of the cartilaginous acetabulum.
- 18. JSS Medical College, Mysuru • Normally, the alpha angle is greater than 60° and an angle less than 55 is considered abnormal.
- 19. JSS Medical College, Mysuru It is important to identify type IIc and beyond (alpha angles less than 50 degree) on USG, as these are unstable hips.
- 20. JSS Medical College, Mysuru Femoral Head Coverage (FHC) and d/D Ratio • Morin has described it. • A line is drawn over the straight iliac line through the bony promontory and through the femoral head, gives the percentage coverage of the femoral head
- 21. JSS Medical College, Mysuru Femoral head overage • The lower limit of FHC in infants aged >1month is 50%. • Since the acetabular fossa cannot be visualized in older children; FHC is used only in the first year of life. • A=distance from the medial wall of the acetabulum to the level of the lateral bony rim • B= distance from the medial wall of the acetabulum to the lateral joint capsule
- 22. JSS Medical College, Mysuru Terjesen femoral head coverage.
- 23. JSS Medical College, Mysuru Dynamic Technique • The examination is conducted in the supine or lateral decubitus position • The dynamic technique is performed with the infant in both the lateral and supine position, and images are obtained in the coronal and transverse planes, both with and without stress. • hip and knee are flexed 90°, and the ultrasound transducer is placed perpendicular to the lateral aspect of the infant’s hip. B. Transverse ultrasound image shows gluteus muscles (G), the cartilaginous femoral head (FH), metaphysis, ischium (I), and labrum (L).
- 24. JSS Medical College, Mysuru • Stress views are achieved by holding the flexed hip in a mild degree of adduction and applying firm but gentle pressure towards the hip joint along the shaft of the femur Dysplastic hip will show subluxation. • The position of the femoral head is studied in three positions; neutral, flexion with adduction and flexion with abduction at rest. The same views are reevaluated after stress.
- 25. JSS Medical College, Mysuru Harcke’s method of dynamic hip evaluation To detect subtle instability, done in 4 steps: 1. Coronal neutral position: similar to Graf’s method, without angle measurements 2. Coronal flexion: with 90º flexion, identify tri-radiate cartilage (TC), transducer moved anterior to posterior (A-P). Normal: when the transducer is posterior to the TC – femoral head (FH) not visible. Abnormal head position: when the transducer is posterior to the TC – FH visible With knee push-up: hip instability diagnosed by seeing FH move over the posterior edge of the TC. 3. Transverse flexion: with 90° flexion. Normal: Head lies above the “U” formed by the anterior and posterior portions of the acetabulum, separated by the TC. With knee push-up: instability – gap between the FH and the acetabulum (TC / AP / PP) increases. With hip in abduction and pull-down of knee: the dislocated hip is relocated into the acetabulum. 4. Transverse neutral: Normal – FH in the “U” with its centre towards the TC. Dislocated – TC cannot be seen in this plane
- 26. JSS Medical College, Mysuru
- 27. JSS Medical College, Mysuru Subluxable on application of stress • Figure 9 (A-C): Unstable hip. Coronal USG images show that the femoral head is centrally placed in the acetabulum at rest (A), with subluxation ,after stress (B). The diagram (C) shows the extent of subluxation
- 28. JSS Medical College, Mysuru • Figure 10: (A-C): Hip subluxation (incomplete dislocation). Diagram (A), coronal USG image (B) and transverse USG image (C), show that the • femoral head lies below the labrum with partial contact between the femoral head and acetabulum Subluxated
- 29. JSS Medical College, Mysuru Dislocated Hip dislocation. Diagram (A) and coronal USG (B) show that the femoral head is completely out of the acetabulum, lying in the soft tissues, lateral to the iliac bone
- 30. JSS Medical College, Mysuru Dislocated Hip dislocation. Coronal USG images of a normal left hip (A) and right hip dislocation (B, C). A concavity (arrow) is seen along the iliac surface due to the pressure of the femoral head, leading to a pseudoacetabulum formation
- 31. JSS Medical College, Mysuru Reporting format • Anatomical description including the normal / dysplastic • Appearance of the bony and cartilaginous acetabulum, • Appearance of the femoral head with its shape, size and status of the ossification center. • Dynamic study • Description of the position of the femoral head in relation to the acetabulum at rest and on application of stress.
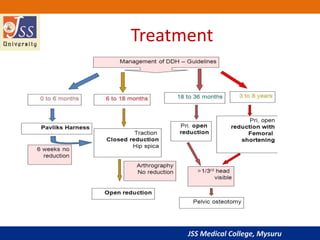
- 32. JSS Medical College, Mysuru Treatment
- 33. JSS Medical College, Mysuru Follow-up • Application of a Pavlik harness (spika), in the abducted position. • USG can be used to follow-up and monitor treatment, after three months. • Should not be performed, unless specifically requested by the orthopedic surgeon. • The improvement in acetabular morphology, as well as the location of the femoral head, can be documented to assist treatment monitoring.
- 34. JSS Medical College, Mysuru Follow-up Hip dislocation with reduction. Coronal USG image (A) shows an empty acetabular cavity with dislocation of the femoral head seen in the coronal (B) and transverse (C) images. Follow-up coronal USG (D), after 5 weeks in a Pavlik Harness shows stable reduction. Note the improved slope of acetabulum
- 35. JSS Medical College, Mysuru Follow-up Hip dislocation with reduction. Coronal USG of the left hip shows subluxation (A) with stable reduction after 5- weeks in a Pavlik harness (C). Coronal USG of the right hip (B) shows subluxability after stress with stable reduction after 5-weeks in a Pavlik harness. Note the improved acetabular slope after reduction
- 36. JSS Medical College, Mysuru Uses • USG of the hip is sensitive and specific in the detection of DDH • False-positive and false-negative rates are reported at 1% to 2%. • USG can also be Used to document the presence and location of the femoral head in proximal focal femoral deficiency (PFFD)
- 37. JSS Medical College, Mysuru Sonographic evaluation of hip effusion • USG can detect very small amounts of intra-articular fluid. It is more sensitive than plain radiographs in diagnosing hip effusions. • It is however not always possible to differentiate between septic, traumatic and sterile effusions. • Diagnostic and therapeutic aspirations. • USG is useful in follow-up.
- 38. JSS Medical College, Mysuru Examination Technique • The patient lies in the supine position with the hip in the neutral position or in 15-20° internal rotation. • Scan is oriented along the long axis of the femoral neck which shows the acetabular brim, femoral head, femoral neck and the ilio-femoral ligament. • The contralateral hip is always examined for comparison.
- 39. JSS Medical College, Mysuru Sonographic appearance of effusion: • Anterior cortex of the femoral head and neck are important landmarks. • The joint capsule normally has a concave contour that parallels the femoral neck.
- 40. JSS Medical College, Mysuru Sonographic appearance of effusion • In the presence of effusion, the joint capsule /ilio-femoral ligament is displaced anteriorly and the anterior contour becomes convex • The fluid-filled hypoechoic space seen between the cortex of the femoral neck and the ilio-femoral ligament increases to more 5 mm. • Asymmetry of 2 mm or more as compared to the contralateral hip is considered significant
- 41. JSS Medical College, Mysuru Septic arthritis. Coronal USG (A) shows subluxation of the femoral head with synovial thickening. Longitudinal USG (B) shows fluid in the anterior ilio-femoral recess. Femoral osteomyelitis with a subperiosteal collection and soft tissue abscess are also seen (C, D)
- 42. JSS Medical College, Mysuru Sonographic appearance of effusion: • Absence of internal echoes does not rule out septic arthritis and aspiration of the fluid is mandatory in clinically suspected infective joint disease. • Anechoic fluid is seen in transient synovitis and usually resolves after 6 weeks.
- 43. JSS Medical College, Mysuru Color Doppler imaging • Epiphyseal flow can be identified in the normal femoral epiphysis. • Diminished or absent flow has been described as a risk factor for avascular necrosis. • RI increases with the amount of effusion. • A power Doppler USG may reveal increased flow in the capsule in inflammatory arthritis.
- 44. JSS Medical College, Mysuru 3D USG: • 3D projection offers imaging in the sagittal and craniocaudal projections, hence there is better demonstration of the position of the femoral head with respect to the acetabulum. • Slow data acquisition and suboptimal reconstruction. Therefore, it is not considered practical yet for routine use.
- 45. JSS Medical College, Mysuru
- 46. JSS Medical College, Mysuru Conclusion • USG is an extremely useful tool for the evaluation of some pediatric hip diseases. • In the assessment of infants with DDH, it is the imaging modality of choice. • Its role in a child with a painful hip is limited to documenting the presence of joint effusion and in guiding aspiration. • USG cannot reliably differentiate between sterile and infected effusions. • The role of color Doppler and 3D USG is at present limited.
- 47. JSS Medical College, Mysuru References 1.Graf R. The diagnosis of congenital hip-joint dislocation by the ultrasonic Combound treatment. Arch Orthop Trauma Surg 1980;97:117-33. 2.Novick G, Ghelman B, Schneider M. Sonography of the neonatal and infant hip. AJR Am J Roentgenol 1983;141:639-45. 3.Harcke HT, Clarke NM, Lee MS, Borns Please Þ nd the att achment, Thanks, MacEwen GD. Examination of the infant hip with real-time ultrasound. J Ultrasound Med 1984;3:131-7. 4.Dezateux C, Godward S. A national survey of screening for congenital dislocation of the hip. Arch Dis Child 1996;74:445-8. 5.American Academy of Pediatrics. Clinical practice guidelines: 6.Terjeson T. Ultrasound as the primary imaging method in the diagnosis of hip dysplasia in children aged < 2 years. J Pediatr Ortho B 1996;5:123-8.
- 48. JSS Medical College, Mysuru