



































































Approach to URTI
- 1. APPROACH TO UPPER RESPIRATORY TRACT INFECTIONS IN CHILDREN DR. SHIV RK DUBEY MBBS (Hons) MD (Pediatrics) KGMU, Lucknow SR-AIIMS Bhopal
- 2. Sunny falls ill • Sunny, 3 yr male, • Brought with history of acute onset cough with rhinorrhoea. • What more would you like to know? • What would you expect on examination? 2
- 3. • acute onset, • red eyes, • rhinorrhea, • diarrhea, • No exanthema, • hoarseness, • cough +++ • Similar cases in family • Throat mild congestion 3
- 4. • Clinically diagnosed : Seasonal viral pharyngotonsillitis • CBC / Throat Culture : not needed. • How will you Manage? • General & Symptomatic Therapy • Antibiotics : Not needed. 4
- 5. Therapy • Rest, oral fluids and salt water gargling- mainly supportive. • Avoidance of irritants (e.g. smoke) • Analgesics and antipyretics - Paracetamol DOC • Home remedies like tulsi, ginger/lemon with honey – good to sooth the throat. • Normal saline nasal drops may help, particularly in <2yrs, • other nasal decongestants sparingly for short term • First generation antihistamines may relieve rhinorrhea by 25 – 30%. • Cough suppressants? • Brandy/ soup/ other special Diet / Zinc/ Herbal products/vit C • No confirmed role. Takes 5-7 days to resolve, so do explain 5
- 6. Case History 6 year old Arjun was brought to your clinic with 2 day history of high spiking fever and mild cough What more will you ask? 6
- 7. • Acute onset, • Has no red eyes, or rhinorrhea or diarrhea, • No exanthema, • Pain and Difficulty in swallowing, not even able to take liquids easily • Cough mild, • No history of similar cases in the family • Arjun prefers to sleep most of the day. 7
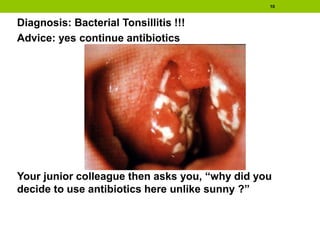
- 8. Examination • Arjun looks ill, • RR 28, HR 110, • Sats, perfusion and B.P normal. • Rt tonsil showed a purulent discharge with inflammation of both tonsils. • Bilateral tender cervical LN++, • Ear and Nose – Normal, • Other system examination – normal 8
- 9. “What does Arjun have?” asks the mother. “I had been to a nearby doctor in the morning and have been prescribed antibiotics, should I continue it”, she adds?” 9
- 10. Diagnosis: Bacterial Tonsillitis !!! Advice: yes continue antibiotics Your junior colleague then asks you, “why did you decide to use antibiotics here unlike sunny ?” 10
- 11. Sunny and Arjun Sunny • Acute onset, Red eyes, rhinorrhea, cough, diarrhea, Generalized maculo- papular rashes. • No Pharyngeal exudates and cervical lymphadenopathy. • Most probably viral Arjun • Explosive onset, throat pain, rapid progression, very little cough/cold. • Pharyngeal congestion more, thick exudates, ulcers and vesicles, purulent patchy tonsils with tender LN++, Toxicity +++ • Most probably bacterial 11
- 12. Etiology of pharyngo-tonsillitis Viral cause : • Rhino virus (common cold) (60%), • Enterovirus, Influenza virus, Para-influenza virus. • Adenovirus, • Special : HIV, Cytomegalovirus, Coxsackievirus, Herpes simplex, Ebstein-barr virus. Bacterial cause : • Group A ß-hemolytic streptococci (15-30% >3 years old ) • C. diptheriae, Hemophilus influenzae, N. meningitides. • Special : Gonococcus, A. hemolyticum, and Mycoplasma pneumoniae
- 13. Diagnosis of bacterial pharyngo-tonsillitis • Mainly clinical but accuracy only 35-50% • Blood count, ESR, CRP are generally not useful • ASLO not recommended • Throat culture • Gold standard (rule out test) for diagnosing strep pharyngitis • Negative throat culture result: very high NPV;false negative rates 5% to 10% • Positive result does not reliably distinguish acute streptococcal pharyngitis from asymptomatic carriage. • Should be sent only for clinically suspected strep pharyngitis. • Rapid antigen detection tests – good specificity (high PPV) but poor sensitivity (low NPV)
- 14. •Throat swab should never be sent in suspected viral disease as it may pick up carriers and lead to unnecessary antimicrobial therapy.
- 15. •Pnuemococcus and Hib, if isolated from throat swab, are colonizers and not pathogens.
- 16. 16 In children with no Penicillin allergy Antibiotic (route) (days) Children (< 30kg) Children ( > 30kg) Penicillin V (Oral) (10d) 250 mg BID 500 mg BID Amoxycillin (Oral) (10d) 40mg/kg/day 250 mg TID Benzathine penicillin G (IM) (single dose) 6 lakh Units 1.2 Million Units. In children with Penicillin allergy (Non type 1) Antibiotic ( route ) ( days) Children ( < 27 kg) Erythromycin ethylsuccinate (oral) (10ds) 40-50 mg/kg/day TID Azithromycin (oral ) ( 5days) 12 mg/kg OD I generation Cephalosporin (oral) (10ds) Cephalexin(20mg/kg/dose BD/ Cefadroxil(30mg/kg OD) II Line: Clindamycin (oral) (10days) 7 mg/kg/dose TDS (max 300mg per dose)
- 17. • 2 months later, Arjun is back with fever, cough and coryza. See his throat • Doctor considers him to have viral pharyngitis. DO YOU AGREE? • HERPANGINA 17 Pharyngeal Erythema but not bacterial
- 18. 18 “But doctor” asks the mother “This is the 3rd episode of tonsillitis that Arjun has had in the past 2 years, and one of my family physicians has advised tonsillectomy for him. What is your opinion?
- 19. Guidelines for considering tonsillectomy 1. 7 or more episodes of tonsillitis in 1 yr. 2. 5 or more episodes per year over a 2 year period. 3. Atleast 3 episodes per year for 3 years WITH documentation in medical record for each episode of sore throat AND 1 or more of following 1. Temp>38.3 c 2. Cervical adenopathy 3. Tonsillar exudate 4. Positive test for GABS 19 Large tonsils like this if not causing any obstruction need
- 20. 20 Management Protocol Examine eye / ear / nose / body Conjunctivitis / Coryza Hoarseness / Cough Purulent / Patches / Toxic / Tender L.Nodes • Viral ? • Symptomatics (3-4d) • Bacterial • Antibiotics before / after Culture Responds No Resp. Response Follow up Culture/ RADT -- ve + ve
- 21. Arjun returns • Arjun, our 6 yr old, returns after 10 days, He has fever & headache for past 3 days. • O/E Purulent Nasal discharge, Slight Periorbital edema with tenderness on percussion on maxillary and frontal sinuses • Diagnosis ????? 21
- 22. 22 Arjun has developed Sinusitis
- 23. When does one suspect sinusitis? • Usually Clinical • Prolonged, upper respiratory signs/symptoms >10-14 days, worsens after initial improvement. • Severe upper respiratory signs/symptoms (Fever > 1020F, Facial swelling and pain) 23
- 24. Classification of Sinusitis • Acute Infection<30 days; • Persistent:>14/<30 days; • Severe: Temp>102 °F, Purulent discharge, Sick child. • Subacute:- 30-90 days • Chronic :->90 days. 24
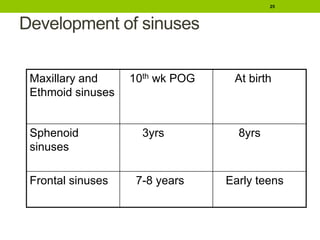
- 25. Development of sinuses Maxillary and Ethmoid sinuses 10th wk POG At birth Sphenoid sinuses 3yrs 8yrs Frontal sinuses 7-8 years Early teens 25
- 26. Predisposing factors • Viral URI • Allergic rhinitis and Nasal Polyps • Nasal Foreign Body • Adenoidal Hypertrophy • Nasogastric tube • Cleft Palate • GERD • Mucociliary disorders • CF • Kartageners Syndrome • Immunodeficiency states • Dental infections 26
- 27. Common Pathogens • Acute and Subacute Sinusitis • Strept. Pneumoniae • Non typeable H influenzae • Moraxella catarrhalis • Strept pyogenes (beta hemolytic) • Chronic Sinusitis • Bacterial Pathogens not well defined • Polymicrobial infection common • Alpha hemolytic Strept., Staph aureus, CONS, Non typeable H influenzae, Moraxella catarrhalis & Anaerobic Bacteria 27
- 28. What are the diagnostic facilities for sinusitis? 28 Clinical History Examination Radiology Microbiology (no major role) Diagnosis of Sinusitis is essentially clinical.
- 29. X ray not for all and recommended if: • Recurrent • Complications • Unclear diagnosis • Abnormal X-Rays- • complete opacification, • mucosal thickening of at least 4 mm, or • an air-fluid level. 29
- 30. X-Rays • Waters view • Maxillary and Frontal sinuses • Caldwells view- • Frontal sinuses seen well • Ethmoid & sphenoid superimposed. 30
- 31. Other views: • Open mouth view-Sphenoid sinuses • Lateral View Sphenoid Sinus. 31
- 32. Management - medical First Line Antibiotics Second line antibiotics3 Alternative antibiotics Type 1 allergy Non type 1 allergy Acute sinusitis1 amoxicillin Co amoxiclav azithromycin cefpodoxime Sinusitis requiring hospitalisation 2 Ceftriaxone or cefotaxime 1 presence of high grade fever (>39 c) with either facial pain or purulent nasal discharge 2 indications of severe infection requiring hospitalisation : high persistent fever with temp>39 C,orbital edema, severe headache, visual disturbance, altered mental status, meningeal signs. 3 no improvement in symptoms in 48-72 hours
- 33. Management Medical • Treat for 10-14 days or 1 week beyond symptom resolution, which ever is later • In case of persistent non response – imaging, sinus endoscopy and sinus aspiration should be done. 33
- 34. Azhar 15 month boy • Azhar, a 15 month otherwise healthy boy had rhinorrhea, cough and fever of 1020F for two days. • On day 5, he became fussy and woke up crying multiple times at night with ear tugging WHAT COULD BE WRONG? HOW DOES ONE EVALUATE THIS CHILD ? 34
- 35. AZHAR might have acute otitis media • CLINICAL EXAMINATION • ENT EVALUATION • OTOSCOPY, preferably pneumatic 35
- 36. 36 • THE RIGHT TYMPANIC MEMBRANE WAS RED AND HAD WHITE FLUID BEHIND THE UMBO l THE FOLLOWING DAY HE HAD SLIGHT REDNESS OF THE LEFT TYMPANIC MEMBRANE AND NO FLUID
- 37. AZHAR HAS ACUTE OTITIS MEDIA RIGHT EAR • Erythema • Fluid • Impaired mobility • Acute symptoms • MANAGEMENT ? 37
- 38. Management AOM – Under 2 Yrs • Analgesia • Paracetamol in adequate doses as good as Ibuprofen • Decongestants no role • Antibiotics in divided doses for 10 days • Choices first line Amoxycillin/ Co-amoxyclav • Second line • Second generation cephalosporins e.g. Cefaclor, cefuroxime. • Co amoxyclav – if not used earlier 38
- 39. Follow up: • Reviewed at 72 hrs • If improving- • Continue the antibiotic for ten days • If patient deteriorates • Consider changing the antibiotic • Choices are Ceftriaxone • Or third generation oral Cephalosporins like Cefopodoxime, Cefdinir (AND NOT Cefixime as has poor action against St pneumoniae and all common gram positive pathogens for OM) 39
- 40. Management of AOM in >2 yr old • Analgesics • Mainstay of treatment • Decongestants have a questionable role • Antibiotics • No urgency to start antibiotics unlike a <2 yr old baby • Wait and watch for 48-72 hrs • Start antibiotics only if deterioration • Drug of choice Amoxycillin 40mg/kg/day in two divided doses for 7 days 40
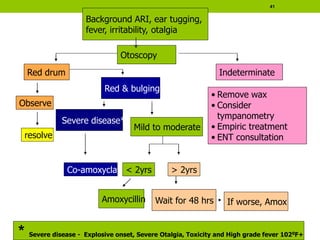
- 41. 41 Co-amoxyclav Mild to moderate < 2yrs Amoxycillin > 2yrs Wait for 48 hrs If worse, Amox Red drum Observe resolve • Remove wax • Consider tympanometry • Empiric treatment • ENT consultation Indeterminate Red & bulging Severe disease* * Severe disease - Explosive onset, Severe Otalgia, Toxicity and High grade fever 1020F+ Background ARI, ear tugging, fever, irritability, otalgia Otoscopy
- 42. CHILD WITH FEVER, COUGH AND NOISY BREATHING Croup Diphtheria Pertussis
- 43. Harshad – a child with fever, cough and noisy breathing 2 year old Harshad, presents with 1 day history of mild grade fever and running nose. His mother also says that his voice has changed and that his cough this time has a peculiar sound which she has not heard before. • What are the possibilities? • What other information one needs? 43
- 44. Harshad - Analyzed Characteristics: • Acute onset • Fever, running nose and cough – infective etiology – likely to be upper airway • Changed cough character – likely to be involving larynx • Hence an acute upper airway infection – laryngitis + 44
- 45. • Other information required: • Is the child playful? • Is the child feeding well? • History of similar complaints in the past? • His mother says that Harshad is quite playful and has been eating well. He does not seem to be disturbed by his loud and almost barking cough. He has not had any similar episodes in past. 45
- 46. • O/E: Harshad is active playful 2 year old, well nourished. His temp is 990F in axilla. • Ant rhinoscopy reveals rhinitis. His ears and throat are normal. • Harshad does have a barking loud cough, and a high pitched inspiratory noise, particularly after coughing and crying. But is absent during rest. • What could the diagnosis be? 46
- 47. 47 Acute viral croup How should Harshad’s illness be graded?
- 48. Grading severity of croup Mild Moderate Severe General Appearance Happy, Feeds well, Interested in surroundings Fussy but inter- active. Comforted by parents. Restless, agitated. Altered sensorium. Stridor Stridor on coughing and crying. No stridor at rest. Stridor at rest worsening with agitation Stridor at rest worsening with agitation Respiratory Distress No distress Tachypnoea, Tachycardia and chest retractions Marked Tachycardia, with chest retractions Oxygenation > 92% in room air >92% in room air <92% in room air. Cyanosis. 48
- 49. 49 Harshad has Mild Croup. How should one treat Harshad?
- 50. Croup - Treatment Mild Moderate Severe Steroids Oral/Nebulized/IM yes Yes Yes Nebulized Adrenaline No No (May be given if deterioration noted during observation) Repeated doses may be required. Oxygen No No As required to keep SaO2 >92% ANTIBIOTICS NO ROLE NO ROLE NO ROLE 50
- 51. Harshad has mild croup • Hence Harshad requires symptomatic treatment • Mother may also be advised to give Humidified air inhalation / bathroom steaming • Few authorities may use a single oral dose of Prednisolone / Dexamethasone to decrease the parental stress as well as the risk of return to medical care. 51
- 52. 52 Harshad’s mother rings you up in the middle of the night because his breathing severity has increased and she is bringing him to the emergency. O/E Harshad now has a audible stridor at rest, He is crying and restless but is consolable by parents. His HR 120, RR 26, Sats 92% in room air. He has minimal intercostals retractions, and has good air entry bilaterally. • Do we need to run tests on him? • How should he be treated now?
- 53. Investigating Croup • Investigations not required in typical croup. • Croup is a clinical diagnosis. • In a child with airway obstruction, neck radiographs or blood tests cause anxiety which may precipitate further distress and obstruction. • X-ray AP view of the soft tissues of neck • if done – reveals a tapered narrowing (steeple sign) of the subglottic trachea instead of the normal shouldered appearance. 53
- 54. 54 X-ray AP View of neck showing a classical narrowed steeple like tracheal air column at larynx with a dilate hypo pharynx as seen in Croup
- 55. Harshad now has moderate croup • Observation for upto 4 hours. • Steroids: • If not given before, a dose of oral/nebulized/IM steroid has to be given. • If it is > 12h since previous dose, repeat dose of Nebulised steroid can be given. • Nebulised Adrenaline: • Used if symptoms are increasing, and repeated if clinically indicated (0.5ml/kg of 1:1000 dilution to maximum of 5ml). Routinely available adrenaline is as effective as racemic adrenaline. • If asymptomatic at the end of 4 hrs, he can be discharged. 55
- 56. Steroid and Adrenaline Dose Steroids • Repeated doses of 2 mg nebulised budesonide 12h x 48hrs • Oral and intramuscular dexamethasone is equally efficacious • Oral corticosteroids are preferred for their ease. • Doses: • Dexamethasone 0.15–0.3 mg/kg • Prednisolone is 1–2 mg/kg. Adrenaline • Adrenaline is used in severe cases and those poorly responsive to steroids. • Need for repeated doses should alert for the probable need for intubation/ PICU care. 56
- 57. 57 At the end of 2 hours, Harshad was clearly unwell. He is now non consolable. His saturations are 84 – 86% in room air and requires 2 lts of Oxygen by nasal cannula. How should one treat Harshad?
- 58. Harshad has developed signs of severe croup • Continue Oxygen as required. • Admit • Continue Nebulised adrenaline as frequently as needed clinically • If adrenaline is required more than 2 hourly, then he has to be shifted to a place with intensive care facilities. • Steroids to be continued. • If airway obstructions/ work of breathing is worsening, then one has to consider intubation and ventilation. Preferably use a tube half size smaller then optimal. • tracheostomy 58
- 59. Croup – Key points • Croup is essentially a viral illness. • No investigations are required in a child with typical croup • Most children with croup develop a mild illness and do not require any medical assistance. • Steroids are extremely useful and indicated in a child with moderate and severe croup. • Steroids can be given orally, IM or Nebulised and all routes are equipotent. • Adrenaline nebulization is reserved for children with severe croup. 59
- 60. Lucky 2 year old has persistent cough with some noise • Lucky has been coughing for past 2 weeks or so. He had low grade fever of initial few days. • Gets severe bouts of coughing, more often when the mother is cooking on her kerosene stove. • Few of the times, he becomes totally out of breath and makes a loud sound, which the mother describes as if its coming from a dog. What more information does one need? 60
- 61. 61 Lucky has Whooping Cough or Pertussis.
- 62. When should one suspect pertussis? • Any individual (child/ adolescence) with • Prolonged (2 weeks or more) paroxysmal cough • With or without whoop/ post tussive vomiting • Irrespective of immunization • Respiratory illness with complications like conjunctival hemorrhages, rectal prolapse or encephalopathy. 62
- 63. 63 • Paroxysmal cough is an essential criteria • Even partially immune individuals retain this • Typical paroxysm : • A series of rapid, forced expirations (usually 5-10), followed by gasping inhalation, leading to the typical whoop. • Cyanosis, bulging eyes, protrusion of the tongue, salivation, lacrimation and distension of the neck veins occurs • Post-tussive vomiting is common. • Can occur several times per hour during both day and night • triggered by yawning, sneezing or physical exertion. • Whoop and post tussive vomiting component of the paroxysm may not be found in the partially immune- therefore not essential for diagnosis
- 64. How to confirm the diagnosis ? • CBC • Leukocytosis with lymphocytosis is the hallmark • Normal count does not exclude pertussis • Neonates may have much higher counts • CXR Not sensitive or specific • Cultures – are gold standard but • Positive only in first week with no prior antibiotics • Need special transport and culture media • Serology – not recommend • PCR Not routinely available, expensive • Diagnosis usually clinical aided by CBC 64
- 65. Treatment • Antibiotics • Reduce transmissibility • May reduce symptoms if given in 1st week • Limited role as usually diagnosed later • Gentle suction for removal of secretions • Avoidance of cough provoking factors • Humidified oxygen and assisted ventilation if required Dose & Duration Status Erythromycin 40-50 mg/kg/day q 6 hrly X 14 days Side effects Duration/ adherence Not < 1 month Clarithromycin 15 mg/kg/day Q 12 hrly X 7 days Expensive Drug interaction Not < 1 month Azithromycin < 6 mths:10 mg/kg/day X 5 d > 6 mths: 10 mg/kg on day 1 and 5 mg/kg day 2-5 Cheap No drug interactions Can be given < 1 mth Cotrimoxazole 8 mg/kg of TMP Q 12 hrly X 14 days Intolerant/CI of macrolides 65 Azithromycin is DOC considering all factors
- 66. Treatment- Supportive • Maintenance of hydration and nutrition • Avoidance of triggers like smoke • One may try bronchodilators/cough sedatives and individualise as per response • Not of any benefit • Antihistaminics • Steroids • Salbutamol ? • Pertussis immunoglobulin 66
- 67. 67 • Un-immunised child, has difficult noisy breathing x 2d • Mother reports mild moderate grade fever and sania is very lethargic and dull for 1 day. • Mother also feels that her neck is swollen. • O/e • Temperature 1000F • Laboured noisy breathing • Diffuse swelling of her neck. • Throat examination : a greyish white membrane over the pharyngo-tonsillar area and beyond. The membrane bleeds on touch and is difficult to remove Sania, 4 year old female child
- 68. What is Sania likely sick from? Sania probably has Diphtheria (Bull neck appearance) 68 http://www.idph.state.il.us/about/immunepics/diphtheria2.htm
- 69. 69 Suspecting diphtheria : • Sore throat with membrane in tonsillopharyngeal area • Fever, hoarseness, barking cough, stridor, membrane over pharynx and larynx • Sero-sanguinous nasal discharge, crusts and a white membrane on septum • Late Presentations : may not be any visible membrane • Palatal or bulbar palsy • Myocarditis with prior sore throat • Acute polyneuropathy with or without prior sore throat. • May occur even in previously immunized Confirming diphtheria • Smear and culture of the membrane or scraping below the membrane • Stain with Neisser or Albert stain
- 70. How will you treat Sania? • Hospitalization in infectious disease facility • Droplet isolation till three consecutive daily cultures are negative • Start treatment without waiting for microbiologic culture confirmation • Components of therapy • Diphtheria antitoxin (DAT), most crucial • Antibiotics for 14 days (Pen G/procaine penicillin/erythromycin) • Supportive care ( ABC and nutrition ) • Management of complications – myocarditis • Complete immunisation on recovery 70
- 71. Treatment - DAT • Always administer test dose • If allergic desensitize • Full dose given IV at one time, diluted in NS (1:20), rate of 1 ml/minute • Limited availability at ID hospitals • Serum sickness in 10% patients Type Total dose in units Nasal 10,000- 20,000 Laryngeal/ Pharyngeal 20,000- 40,000 Tonsillar 15,000-25,000 Combined types/ delayed diagnosis 40,000-60,000 Severe disease* 80,000 –100,000 Carrier/ Contact Not required 71 *extensive disease/ more than 3 days duration/ neck edema/tachycardia/ collapse/ breathlessness
- 72. Treatment continued • Antibiotics (Penicillin G/ Procaine penicillin/ Erythromycin for 14 days) • Strict bed rest for 2- 3 weeks (b/o myocarditis) • Adequate nutrition and hydration • Steroids not recommended • Complete immunization on recovery 72
- 73. THANK YOU