Benign and Malignant Tumours
Download as PPTX, PDF9 likes396 views

The document covers various odontogenic tumors and their classifications, distinguishing between benign and malignant types, including detailed information on specific tumors like ameloblastoma, ameloblastic fibroma, and odontogenic myxoma. It discusses clinical features, radiographic characteristics, histopathological variants, differential diagnoses, treatment options, and prognosis of these tumors. Additionally, it references established literature and studies regarding these lesions.
































































































Benign and Malignant Tumours
- 2. REFERENCES Odontogenic tumours & Allied lesions- Peter A Reichart , Hans P Philipson Textbook of Oral Radiology- White & Pharoah (6th ed.) Diagnostic imaging of jaws- Langland & Langlais Differential Diagnosis of Oral & Maxillofacial lesions- Wood & Goaz (5th ed.) Principles Practice Oral Radiologic Interpretation- H.M Worth Ameloblastic fibroma: A review of published studies with special reference to its nature and biological behavior Yan Chen, Jing-Ming Wang, Tie-Jun Li doi:10.1016/j.oraloncology.2007.05.009 Martin-Granizo Lopez R, Ortega L, Gonzalez Corchon MA et al: Ameloblastic fibroma of the mandible. Report of two cases, Med Oral 8(2):150-153, 2003
- 3. CONTENTS Introduction Definitions Benign tumours - Clinical features - Radiographic features - Differential diagnosis - Treatment Malignant tumours Odontogenic Non-odontogenic
- 4. DEFINITIONS NEOPLASM : A neoplasm as defined by Willis is “ An abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the same excessive manner after the cessation of the stimuli which evoked the change. ” BENIGN TUMOUR : Is a new growth, which is limited by a capsule and grows by local expansion without causing any harm to the host, excepting its position in a vital organ. MALIGNANT TUMOUR : Is a new growth which is characterized by rapid growth, sign of invasion, absence of capsule and last of all dissemination to other parts of the body usually by hematogenous or lymphatic route or both.
- 5. FEATURES OF BENIGN TUMOR Encapsulated Slow growing Painless No metastasis
- 7. ODONTOGENIC TUMOURS Classification Benign Tumors 1) Odontogenic epithelium with mature, fibrous stroma; odontogenic mesenchyme not present Ameloblastomas Calcifying epithelial odontogenic tumor Adenomatoid odontogenic tumor Squamous odontogenic tumour Editorial and Consensus Conference -Lyon, France (WHO/ IARC) in July 2003
- 8. 2) Odontogenic epithelium with odontogenic mesenchyme with or without dental hard tissue formation Ameloblastic fibroma Ameloblastic fibro-dentinoma Ameloblastic fibro-odontoma Complex odontoma Compound odontoma Odontoameloblastoma Calcifying cystic odontogenic tumor Editorial and Consensus Conference -Lyon, France (WHO/ IARC) in July 2003
- 9. 3) Mesenchyme and/or odontogenic ectomesenchyme with or without included odontogenic epithelium Odontogenic fibroma Odontogenic myxoma or fibromyxoma Cementoblastoma Editorial and Consensus Conference -Lyon, France (WHO/ IARC) in July 2003
- 10. Malignant I Odontogenic Carcinomas Metastasizing, malignant ameloblastoma Ameloblastic carcinoma Primary intraosseuos squamous cell carcinoma Clear cell odontogenic carcinoma Ghost cell odontogenic carcinoma II Odontogenic Sarcomas Ameloblastic fibrosarcoma Ameloblastic fibrodentino and fibro-odontosarcoma Editorial and Consensus Conference -Lyon, France (WHO/ IARC) in July 2003
- 11. AMELOBLASTOMA WHO Definition - • Ameloblastoma is a polymorphic neoplasm consisting of proliferating odontogenic epithelium which usually has a follicular or plexiform pattern lying in a fibrous stroma Reichart and Slootweg Definition • Ameloblastoma is a polymorphous neoplasm consisting of proliferating odontogeni c epithelium usually occurring in follicular or plexiform patterns embedded in mature connective tissue stroma. As stated by Robinson, Ameloblastoma is usually unicentric, non-functional, intermittent in growth, anatomically benign and clinically persistent.
- 12. HISTORICAL BACKGROUND 1826 – Guzack – a tumor of jaw 1868 – Broca – 1st neoplasm of this nature in literature 1879 – Falkson gave its thorough description. 1885 – Malassez – ‘Admantinoma’ 1934 – Churchill – ‘Ameloblastoma’
- 13. PATHOGENESIS Resemblance to odontogenic apparatus – derived from the same. Malassez, 1885 – epithelial rests adj. roots of teeth – ‘les debris épithéliaux’ - proliferate Adamantine epithelioma Origin – varied origin Stimulus for initiation - unknown
- 14. GENETIC ALTERATION Overexpressed genes Proto-oncogene FOS – most highly -Fos protein – Activating protein-1 (transcription factor) -Cell proliferation, differentiation, oncogenic transformation -Bone development, regulator of osteoclast - macrophage lineage determination, bone remodelling. TNFR 1A – induction of AP-1 activity -TNF-α – signal transduction -Inflammation, cell proliferation, differentiation & apoptosis Heikinheimo et al (2002, J Dent Res)
- 15. Underexpressed genes – Cadherins, KRT7, NOTCH & TGFB1 Disturbances in cell adhesion & cell-cell communication Sonic hedgehog (SHH) – (expression of PTCH) Dysregulation of signalling pathway for ectomecenchymal interactions Heikinheimo et al (2002, J Dent Res)
- 16. VARIANTS Classical solid / multicystic ameloblastoma (SMA) Unicystic ameloblastoma (UA) Peripheral ameloblastoma (PA) Desmoplastic ameloblastoma (DA)
- 17. SOLID / MULTICYSTIC AMELOBLASTOMA Clinical features- Early stages – no clinical signs Later – Facial deformity – swelling (bony hard & bulky) Loosening of teeth Fractures Pain – less frequent (pressure on nerves, sec. infection) Large tumors – thinning of cortices (egg shell crackling) Perforation – late feature Age – Mean age – 35.9 yrs (range 9- 92yrs) Maxillary tumours – 47 yrs Mandibular tumours – 35.2 yrs Sex distribution – Male : female – 1.1 : 1 Reichart et al 1995, biological profile of 3677 cases of ameloblastoma
- 18. RADIOGRAPHIC FEATURES Honeycomb appearance Spider-like appearance Soap-bubble appearance Mother-daughter cell appearance
- 20. ROOT RESORPTION PATTERN Knife edged root resorption Multiplanar root resorption
- 21. RADIOGRAPHIC DESCRIPTION OF AMELOBLASTOMA WORTH (1963) 4 types Unilocular “Gross caricature of spider” Multilocular Replacement of normal bone with honeycomb appearance.
- 22. CT SCANS
- 23. CBCT
- 24. MRI T2WI Gd – T1WI
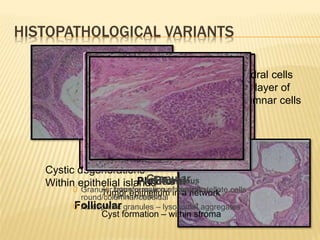
- 25. HISTOPATHOLOGICAL VARIANTS Islands – Central polyhedral cells Surrounded by layer of cuboidal / Columnar cells Cystic degenerations – Within epithelial islands Follicular Plexiform Tumor epithelium in a network Cyst formation – within stroma Acanthomatous 0 Extensive squamous metaplasia 0 Keratin formation Granular 0 Granular transformation of central stellate cells – round/columnar/cuboidal 0 Acidophillic granules – lysosomal aggregates Basal
- 26. PERIPHERAL AMELOBLASTOMA Extraosseous, soft tissue ameloblastoma Histology – similar to SMA Tooth bearing region Painless, sessile, firm, Surface – smooth / pebbly, granular / papillary, warty Pink / red / dark red
- 27. Duration – 2 days – 20 yrs 2 - 10% of ameloblastomas R/F- cupping or saucerization Resemblance to – Epulis Papilloma Pyogenic granuloma
- 28. UNICYSTIC AMELOBLASTOMA ‘UNICYSTIC’ – macro & microscopic appearance – well defined, monocystic cavity – lined focally / entirely of ameloblastomatous epithelium. Synonyms – Cystic ameloblastoma Mural ameloblastoma
- 29. Age – Dentigerous variant – younger (mean age – 16.5) Non dentigerous – mean age – 32.2 Male : female – Dentigerous - 1.6 : 1 Non-dentigerous – 1 : 1.8 Location – Mandible Posterior mandible, Asc. Ramus Dentigerous variety – 3rd molar
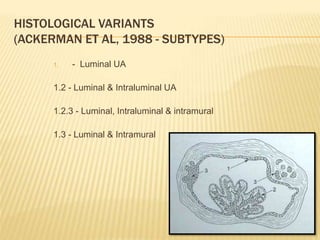
- 30. HISTOLOGICAL VARIANTS (ACKERMAN ET AL, 1988 - SUBTYPES) 1. - Luminal UA 1.2 - Luminal & Intraluminal UA 1.2.3 - Luminal, Intraluminal & intramural 1.3 - Luminal & Intramural
- 32. DESMOPLASTIC AMELOBLASTOMA Variant of SMA – extensive stromal collagenization / desmoplasia Benign, locally infiltrative Location - Maxilla = mandible Age – mean – 42.8 yrs Male : female – 1 : 0.9 Origin – similar to SMA
- 33. OTHER TYPES Clear cell A KeratoA & Papilliferous A Mucus cell differentiation Hemangiomatous Ameloblastoma Extragnathic Adamantinoma Metastasizing Ameloblastoma
- 34. DIFFERENTIAL DIAGNOSIS OKC Odontogenic Myxoma Aneurysmal bone cyst Central gaint cell granuloma Central hemangioma
- 35. TREATMENT Treatment depends on the type of lesion – SMA – radical surgical intervention UA – conservative surgical enucleation Peripheral ameloblastoma – more conservative surgery Radiotherapy – 1982 – Reynolds et al – effects of radiation on ameloblastoma – usefulness Not used as 1st line of treatment
- 36. PROGNOSIS SMA – ↑ Recurrence Maxilla – spreads faster - ↑ morbidity & mortality - Posterior maxilla – poorest prognosis Mandible – restricted by thick cortex Follow up – 5-10 yrs post-surgery DA – same rate of recurrence as SMA Peripheral ameloblastoma – low recurrence (16-19%) UA – 10.7%
- 37. CALCIFYING EPITHELIAL ODONTOGENIC TUMOUR Also called as Pindborg tumor, first described by J.J PINDBORG in 1956 Benign, odontogenic neoplasm exclusively epithelial in origin 1% of odontogenic tumors ORIGIN – remnants of primitive dental lamina
- 38. CLINICAL FEATURES Age ; Sex – 4th decade ; Males Site – Mandible : Maxilla = 2 :1 Malignant - Locally invasive with high recurrence rate
- 39. RADIOGRAPHIC FEATURES Expanded cortices in all dimensions Radiolucent ; poorly defined, non- corticated borders Unilocular, multilocular or “moth- eaten” “ Driven-snow ” appearance from multiple radiopaque foci Root divergence / resorption ; impacted tooth
- 40. Histology Islands of eosinophilic epithelial cells Cells infiltrate bony trabeculae Nuclear hyperchromatism and pleomorphism Psammoma-like calcifications (Liesegang rings)
- 41. DIFFERENTIAL DIAGNOSIS Dentigerous cyst Adematoid odontogenic tumor Ameloblastic fibro-odontoma
- 42. TREATMENT Behaves like ameloblastoma Low recurrence rate En bloc resection, hemimandibulectomy/partial maxillectomy. Recurrence rate - Franklin & Pindborg (1976) : 14%
- 43. ADENOMATOID ODONTOGENIC TUMOUR Adenoameloblastoma , Ameloblastic adenomatoid tumor First reported by - STAFNE Term coined by PHILIPSEN & BIRN (1969) ORIGIN – Dental epithelium TYPES- Peripheral Central - Follicular & Extra-follicular
- 44. CLINICAL FEATURES Age - 2nd decade Male : Female – 1 : 2 Slow growing expansile lesion Location : Anterior maxilla Associated with unerupted tooth
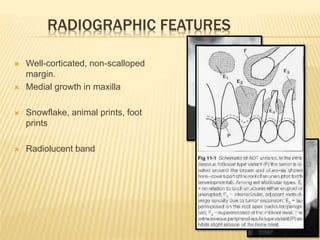
- 45. RADIOGRAPHIC FEATURES Well-corticated, non-scalloped margin. Medial growth in maxilla Snowflake, animal prints, foot prints Radiolucent band
- 47. HISTOLOGY Thick fibrous capsule, clusters of spindle cells, columnar cells (rosettes, ductal) throughout
- 48. DIFFERENTIAL DIAGNOSIS Dentigerous cyst Ameloblastic fibroma CEOT Treatment – enucleation, recurrence is rare Recurrence rate - Low : 0.2%
- 49. SQUAMOUS ODONTOGENIC TUMOUR Benign Epithelial Odontogenic Tumor Hamartomatous proliferation Origin CLINICAL FEATURES 2nd and 3rd decade 1:1 Tooth mobility Tenderness on percussion
- 51. HISTOLOGY Oval nest of squamous epithelium in mature collagen stroma.
- 52. DIFFERENTIAL DIAGNOSIS Dentigerous & Radicular cyst Treatment – Conservative enucleation & thorough curettage ; low recurrence rate.
- 53. II. ODONTOGENIC EPITHELIUM WITH ODONTOGENIC MESENCHYME WITH OR WITHOUT DENTAL HARD TISSUE FORMATION
- 54. AMELOBLASTIC FIBROMA AF – True mixed odontogenic tumor Consists of both epithelial and ectomesenchymal components are neoplastic. 1946, Thoma and Goldman were the first to classify this tumour as a separate entity
- 55. CLINICAL FEATURES Hard swelling Mandibular posteriors 2nd and 3rd decade Tumour size - 1 - 10 cm Recurrence rate - 33.3% Malignant transformation - 11.4% Yan Chen, Jing-Ming Wang, Tie-Jun Li . Ameloblastic fibroma : A review of published studies with special reference to its nature and biological behavior.
- 56. RADIOGRAPHIC FEATURES Martin-Granizo Lopez R, Ortega L, Gonzalez Corchon MA et al: Ameloblastic fibroma of the mandible. Report of two cases, Med Oral 8(2):150-153, 2003.
- 57. DIFFERENTIAL DIAGNOSIS Dentigerous cyst Ameloblastoma
- 58. TREATMENT Conservative surgery Excision Enucleation Curettage Radical surgery Marginal resection Segmental resection Hemisection
- 59. AMELOBLASTIC FIBRO-ODONTOMA Hooker -1967 Ameloblastic fibroma + odontome 2% incidence- Regezi et al
- 60. FEATURES C/F 83%- unerupted tooth 2nd decade of life M : F - 1.4 : 1 Posterior mandible - 53.2% R/F- Expansile, smooth- well defined cortication Radiopaque flecks - 1 – 2 mm to 1cm Tooth displacement
- 62. TREATMENT Conservative enucleation Resection with removal of impacted teeth.
- 63. ODONTOME Benign Hamartoma 1971 - Pindborg et al. 2 types - Compound and complex Pathogenesis Local trauma Infection Family history Genetic mutation
- 64. CLINICAL FEATURES Slow growing , expansile lesion Compound – 2nd decade of life ; before 20yrs of age Complex - 2nd decade of life ; before 30yrs of age M : F - 1.5 : 1 Location – Compound – anterior maxilla ; posterior mandible – 2 : 1 Complex – anterior maxilla ; posterior mandible – 1 : 2 Displacement of tooth
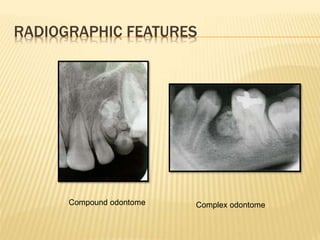
- 65. RADIOGRAPHIC FEATURES Compound odontome Complex odontome
- 66. VARIANTS Cystic odontome 28% incidence Amelobalstic odontome Treatment : Surgical enucleation Differential diagnosis Ameloblastic fibro-odontome
- 67. III. Mesenchyme or odontogenic ectomesenchyme with or without included odontogenic epithelium
- 68. ODONTOGENIC MYXOMA Benign non-encapsulated odontogenic neoplasm. In 1947- Thoma and Goldman Pathogenesis Arises from mesenchymal portion of the tooth germ, dental papilla, the follicle or the periodontal ligament.
- 69. CLINICAL FEATURES 1-3% 2nd and 4th decade M:F- 1:1.6 Mand posteriors
- 70. RADIOGRAPHIC FEATURES Two pattern depending on evolution of tumor: Osteoporotic appearance Breakout/destructive phase
- 72. DIFFERENTIAL DIAGNOSIS Ameloblatoma Central giant cell granuloma Central hemangioma Osteosarcoma Treatment : As infiltrative local recurrence rate - 33% Resection with 1-1.5 cm of bone
- 73. ODONTOGENIC FIBROMA Two variants can be distinguished: an intraosseous or central type (COF) and an extraosseous or peripheral type (POF) Clinical variants- 1) hyperplastic, 2) simple, 3) WHO type C/F - age- 3rd decade M:F- 1:2.8 Maxilla : mandible – 1 : 6.8 Siar C H et al ,Clinicopathological study of peripheral and central odontogenic fibromas (WHO – type in Malaysians ( 1967 - 9 5 ). B r J Oral Maxillofac Su rg 2000 ;38: 19- 22 .
- 75. BENIGN CEMENTOBLASTOMA True cementoma, Attached cementoma First reported by NORBERG (1930) Term given by KRAMER < 1% of all odontogenic tumors Unique in two ways: True neoplasm of cementoblasts Attached routinely to an involved tooth Origin - PDL
- 76. CLINICAL FEATURES 2nd and 3rd decade Mand 1st premolar and molar M : F – 1 : 1.2 SYMPTOMS Pain – 53% of cases SIGN Swelling-73% cases
- 77. RADIOGRAPHIC FEATURES Three radiologically distinct stages: Uncalcified matrix stage Calcified blastic stage Mature stage
- 78. HISTOLOGY
- 79. DIFFERENTIAL DIAGNOSIS Periapical cemental dysplasia Enostosis Hypercementosis Sclerosing osteitis TREATMENT Surgical extraction of involved tooth Tumor can be amputated from tooth & tooth endodontically treated
- 80. Pattern of flecks on CEOT According to histological criteria by Franklin and Pindborg, scattered flecks are seen with central radiolucency Histopathologically, features of unilocular or multilocular ameloblastoma are similar. Lichen planus of jaw – Odontogenic myxoma ; Traumatic bone cyst
- 81. Metastasizing malignant ameloblastoma Criteria for identifying metastatic diseases of the jaws – 1. Lesion must be a true metastasis localized to bone tissue, as distinguished from direct invasion by a primary tumour of contiguous structure 2. Lesion must be verified microscopically as carcinoma 3. Primary site of the lesion must be known Ameloblastoma – metastasizes in spite of its benign histologic appearance. Associated with hypercalcemia Age – Third decade (5 - 74 yrs) Gender – M : F = 1 : 1.2 Location : Posterior mandible
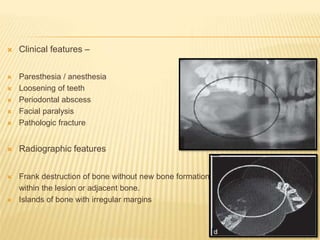
- 82. Clinical features – Paresthesia / anesthesia Loosening of teeth Periodontal abscess Facial paralysis Pathologic fracture Radiographic features Frank destruction of bone without new bone formation within the lesion or adjacent bone. Islands of bone with irregular margins
- 83. Ameloblastic Carcinoma Corio and associates – Any ameloblastoma in which there is histologic evidence of malignant disease in the primary or recurrent tumour, independent of the presence of metastasis. Most ameloblastic carcinomas presumably arise de novo, and less than 1% of ameloblastomas undergo malignant transformation. Ameloblastic carcinoma, secondary type, is defined as a malignantly transformed tumor within a pre-existing benign ameloblastoma, regardless of the presence of metastasis. Yukio Yoshioka, Shigeaki Toratani, Ikuko Ogawa and Tetsuji Okamoto. Ameloblastic Carcinoma, Secondary Type, of the Mandible: A Case Report. J Oral Maxillofac Surg 71:e58-e62, 2013.
- 84. Clinical Features Age – 4th decade Female : Male - 1 : 2.7 Swelling (61.5%), bleeding, ulceration and fistula (15.4%). Progressive types : cortical bone perforation, soft tissue invasion, recurrences and metastases.
- 85. Radiographic Features Unilocular or multilocular Ragged borders Root resorption Cortical perforation
- 86. Histopathology Kar, et al.:Ameloblastic carcinoma: A clinicopathologic dilemma – Report of two cases with total review of literature from 1984 to 2012. Annals of Maxillofacial Surgery | January - June 2014 | Volume 4 | Issue 1
- 87. Differential Diagnosis Metastatic carcinoma Squamous odontogenic tumour
- 88. TREATMENT Radical surgery with neck dissection Hemimandibulectomy / maxillectomy Postive margins : adjuvant radiotherapy - 5 fractions of 1.8 Gy each for a period of 5 weeks (45 Gy).
- 89. Primary Intraosseous Squamous Cell Carcinoma WHO defines: “ Odontogenic carcinoma consisting of a squamous cell carcinoma arising within the jaws having no initial connection with the oral mucosa and presumably developing from residues of the odontogenic epithelium or from an odontogenic cyst or tumour”. Elzay 1982: Arising from odontogenic cysts Arising from ameloblastoma( malignant or AC) De novo
- 90. CLINICAL FEATURES Age : 6th and 7th decade M : F- 3 : 1 Location : Posterior mandible Tooth mobility Paraesthesia Regional LN involvement Exfoliation Non-healing Extraction sockets (50- 60%) Mitsuyoshi Iino et al. Solid type primary intraosseous squamous cell carcinoma in the maxilla: report of a new case. Ear, Nose and Throat Disorders 2013, 13:13.
- 91. Radiographic Features Alveolar bone destruction Cortical perforations Pathologic fractures “Floating tooth” “ Bays within bays ” Huang et al.: Primary Intraosseous Squamous Cell Carcinoma. Arch Pathol Lab Med—Vol 133, November 2009
- 92. HISTOPATHOLOGY
- 93. Differential diagnosis Gingival carcinomas Ameloblastic carcinoma
- 94. Treatment Partial or total maxillectomy or mandibulectomy. Radiotherapy - Fractionated in seven weeks each session of 50 Gy. Adjuvant chemotherapy Cisplatin 100 mg/m2 IV or 40-50 mg/m2 IV weekly for 6-7wk. Cetuximab 400 mg/m2 IV loading dose 1wk before the start of radiation therapy, then 250 mg/m2 weekly (premedicate with diphenhydramine and ranitidine) .
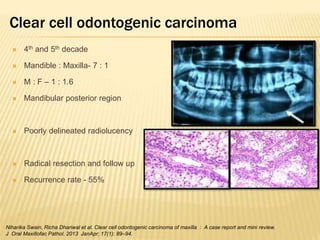
- 95. Clear cell odontogenic carcinoma 4th and 5th decade Mandible : Maxilla- 7 : 1 M : F – 1 : 1.6 Mandibular posterior region Poorly delineated radiolucency Radical resection and follow up Recurrence rate - 55% Niharika Swain, Richa Dhariwal et al. Clear cell odontogenic carcinoma of maxilla : A case report and mini review. J Oral Maxillofac Pathol. 2013 JanApr; 17(1): 89–94.
- 96. Ghost cell odontogenic carcinoma Gorlin 1962- “Malignant counterpart of calcifying odontogenic cyst”. Age – 4th and 5th decade Gender – M : F = 2.6 : 1 Location – Maxilla > Mandible Clinical features Swelling with or without pain Osseous destruction with paresthesia
- 97. Radiographic features Cortical destruction, obliteration of maxillary sinus Ill-defined radiolucency Opacification
- 98. Ameloblastic Fibrosarcoma It is a rare malignant neoplasm composed of benign , ameloblastomous epithelium and malignant ectomesenchyme. Represents only 2% of all odontogenic tumors. Clinical features Pain and swelling Ulceration and bleeding Paresthesia of lower lip 2nd decade Mandible : Maxilla = 2.3 : 1 M : F - 2 : 1
- 99. Radiographic Features Ill-defined radiolucency Pathological fractures Treatment Wide local excision Partial maxilla or mandibulectomy Post surgical radiotherapy / chemotherapy Recurrence rate - 20% Daniela Otero Pereira et al. Maxillary Ameloblastic Fibroma: A Case Report . Braz Dent J (2011) 22(2): 171-174
- 100. Osteosarcoma Osteosarcoma - Two types An osteoblastic (sclerosing) and An osteolytic type. Gender : Males > Females Age - 33 years (Mean) Location : Mandible > Maxilla Arise due to – Radiation induced Trauma
- 101. Clinical Features Pain, swelling, paraesthesia and ulceration. Affected teeth may be loosened and displaced Age- 4th & 5th decade M : F - 1.1 : 1
- 102. Radiographic Features Earliest radiographic sign - widening of the periodontal ligament space or a radiolucency around one or more teeth. Later on, the lesion assumes an osteolytic radiolucent form, an osteoblastic radiopaque form or a mixed radiolucent image with radiopaque foci. Ill-defined borders. Expansion and destruction of the cortical plates. Characteristic sunray , sunburst or fan-shaped appearance - thin spicules of new bone extend outwards away from the bone cortex. Chittaranjan B, Tejasvi MA, Babu BB, Geetha P. Intramedullary Osteosarcoma of the Mandible: A Clinicoradiologic Perspective. J Clin Imaging Sci 2014;4, Suppl S1:6
- 103. TREATMENT The cornerstone of primary jaw osteosarcoma treatment is adequate surgical resection. Radiotherapy or chemotherapy can be used in association with surgical resection or alone as a palliative treatment in advanced cases. Literature review has shown that patients treated initially by aggressive local or even radical procedures such as hemimandibulectomy fared better. Introduction of multi-agent chemotherapy has improved the survival rates, with 60-70% patients surviving after treatment.
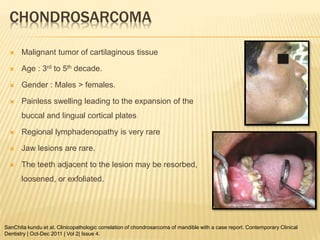
- 104. CHONDROSARCOMA Malignant tumor of cartilaginous tissue Age : 3rd to 5th decade. Gender : Males > females. Painless swelling leading to the expansion of the buccal and lingual cortical plates Regional lymphadenopathy is very rare Jaw lesions are rare. The teeth adjacent to the lesion may be resorbed, loosened, or exfoliated. SanChita kundu et al. Clinicopathologic correlation of chondrosarcoma of mandible with a case report. Contemporary Clinical Dentistry | Oct-Dec 2011 | Vol 2| Issue 4.
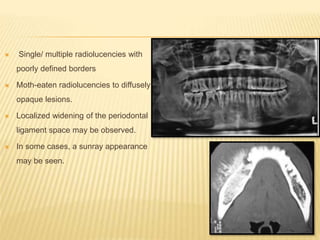
- 105. Single/ multiple radiolucencies with poorly defined borders Moth-eaten radiolucencies to diffusely opaque lesions. Localized widening of the periodontal ligament space may be observed. In some cases, a sunray appearance may be seen.
- 106. TREATMENT Wide surgical excision is the mainstay of treatment for These tumors are radioresistant and chemotherapy can be used as an adjuvant therapy after wide surgical excision is made Prognosis is poor. Local recurrence occurs and may indicate subsequent metastasis; hence adequate treatment and long-term follow-up, including periodic systemic evaluation, are required.
- 107. EWING’S SARCOMA Malignant tumor of bone derived from mesenchymal connective tissue of the bone marrow. Rarely occurs in the jaws Rapidly growing, highly invasive tumor Pain and swelling are the most common manifestations. Age : Children ; young adults Gender : M : F = 2 : 1
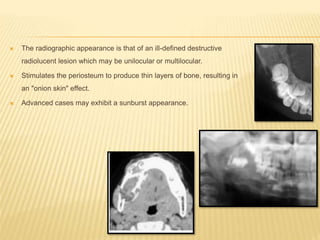
- 108. The radiographic appearance is that of an ill-defined destructive radiolucent lesion which may be unilocular or multilocular. Stimulates the periosteum to produce thin layers of bone, resulting in an "onion skin" effect. Advanced cases may exhibit a sunburst appearance.
- 109. Chemotherapy, radiation therapy and surgery, has led to an improvement in prognosis. Poor prognostic factors are patients below 10 years of age, presence of metastasis, presence of systemic symptoms, large tumor volume. ES of the mandible has got better prognosis than long bones since facial sites are diagnosed earlier. TREATMENT
- 110. BURKITT'S LYMPHOMA Characteristic form of non-Hodgkin's lymphoma that is endemic in Africa and occurs sporadically in North America. The Epstein-Barr virus has been implicated in the etiology. Age : Peak : 5 years Primarily a tumor of childhood, with occasional cases seen in young adults. Location : Maxilla > Mandible. Gender : M : F = 2 : 1 Vasudevan V, Mohandas U, Manjunath V. Burkitt's lymphoma in leukemic phase in an Indian boy. Indian J Dent Res 2011;22:340-4
- 111. Clinical features – Loosening of teeth Bilateral jaw tenderness Swollen gingiva Cervical lymphadenopathy Radiographic features Ill defined radiolucency extending into tooth crypt Displacement of developing and erupting teeth Floating in air appearance Sunray spicules
- 112. TREATMENT Good response to chemotherapy, particularly cyclophosphamide. The tumor also has been shown to be sensitive to methotrexate, vincristine, and cytarabine. Combinations of drugs have achieved remissions in more than 90% of patients. Unfortunately, most of the cases recur and patients ultimately succumb to the disease. Recent clinical trials with intensive, multiagent chemotherapeutic protocols have shown a fair remission rate. Individuals who do not receive treatment are not likely to survive longer than 3 to 6 months.
Editor's Notes
- #12: Significant of all OT – high incidence, clinical behavior & high recurrences
- #16: Amelogenin gene –Tsujigiwa et al (2005, Oral Oncology)
- #19: Septae are usually coarse and curved, may be remodelled. Numerous small locules. Also seen are a few larger ones. Root resorption & displacement On a tangential view – margin of the lesion meets the buccal cortex – acute angle – tumor like manner of expansion Unilocular
- #20: This resembles a dentigerous cyst – varied thickness of expansion of buccal cortex – more in favor of a tumor
- #23: Coronal CT in a bone window – expansile lesion of the rt ramus of mandible – thinning & perforation in areas
- #25: MRI – correlates well with histopathology – can diff solid & cystic areas (better than CT). Varied high to low signal intensity on MRI On a T2WI mr – hetrogenous high signal intensity noted in the body of mand. An area of very high signal intensity – cystic areas On a Gd – T1WI mr – enhancement of the lesion (indicating solid nature of lesion) also there is an area of low signal intensty with no enhancement – cystic space.
- #28: Currently, t here is general agreement that the PA and t he BCC are essentially the same lesion and thus should be regarded as a single entity
- #33: Shows mixed radiolucent-radiopaque appearance similar to fibro-osseous lesions
- #35: Aneurysmal bone cyst Tooth displacement > tooth resorption. Fluid levels – CT. < 20yrs, Female Unilocular, multilocular (thin wispy trabeculae). Rapid growth & expansion Displacement of tooth. Multiplanar root resorption
- #51: Hamartomatous proliferation. Maxillary incisor-canine and mandibular molar. Tooth mobility common complaint Radiology – triangular, localized radiolucency between contiguous teeth. Histology – oval nest of squamous epithelium in mature collagen stroma Treatment – extraction of involved tooth and thorough curettage; maxillary – more extensive resection; recurrences – treat with aggressive resection
- #56: This fibroma is often associated with an impacted tooth.
- #57: No root resorption, no hydraulic effect
- #60: Thus radiographically, it appears as a combined radiolucent/radiopaque lesion and must be differentiated from other similar-appearing lesions such as the ossifying fibroma, the calcifying epithelial odontogenic tumor, the calcifying odontogenic cyst, an odontoma, and an adenomatoid odontogenic tumor.
- #61: washer like appearance
- #65: Mild expansion- odontome Large expansion- cystic odontome or ameloblastic odontome
- #66: 48% unerupted tooth
- #71: Tennis racket- osteoporotic Sun burst- break out
- #87: Among all the reviewed cases, 27% presented at first histopathologic Diagnosis as a follicular Or Plexiform Ameloblastoma And Secondarily as an ameloblastic carcinoma
- #92: Bays within bays- margins with large eroded areas within which smaller areas of bone destruction are present
- #100: The degree of malignancy of the mesenchymal component is decided by the cellularity, palisading pattern and cellular atypia (mitosis, shape and size).
- #102: Osteosarcoma of jaw bones have some distinct features such as older age at presentation, longer median survival, rare metastases and local recurrences difficult to control, typically leading to death of the patients