Beta Blockers in current cardiovascular practice
Download as PPTX, PDF4 likes1,016 views

The document discusses the use of beta-blockers (BBs) in cardiovascular practice, particularly in managing heart failure, angina, and hypertension. It highlights the importance of BBs in improving mortality rates in heart failure with reduced ejection fraction and emphasizes the necessity for careful dosage and monitoring. Additionally, it addresses common myths and cautions regarding BB administration, noting the risks of abrupt withdrawal and specific contraindications.













































































Beta Blockers in current cardiovascular practice
- 1. BETABLOCKERS IN CURRENT CARDIOVASCULAR PRACTICE Dr. Nagula Praveen, MD, DM Assistant Professor of Cardiology, Osmania General Hospital, Hyderabad Email: drpraveennagula@gmail.com Twitter: @kizashipraveen
- 2. Case 1 A young male,cocaine addictive to be given BB or not?
- 3. A young patient with angina,BP 170/100 mm Hg on NTG persistnet chest pain.what to be given? BB
- 4. A patient with HF came with acute decompesnation ,basal crepts Bb to be continued?
- 6. Contents Introduction Beta Receptors Indications for usage of BBs Myths vs facts Words of caution Side effects BISOPROLOL - The cardioselective BB Take home message
- 7. Introduction Raymond P. Alquist discovered the adrenergic receptors as and receptors. James Whyte Black, discovered the drug propanolol (the greatest breakthrough after discovery of digitalis). Since then BB evolved as major group of drugs in different subsets of cardiovascular disease. They have significant mortality benefit in HFrEF (once contraindicated in HF).
- 10. Indications for use of BBs
- 11. HEART FAILURE Describe the magnitude of the problem Previous classification of heart failure previous theories of heart failure
- 13. Neurohormonal model of Heart Failure
- 19. BB had a significant effect
- 33. Target Doses of Heart Failure Medical Therapy and Blood Pressure: Insights From the CHAMP-HF Registry--- Eligible patients had a primary diagnosis of HFrEF (LVEF ≤40%) within 12 months of enrollment and were taking at least one oral drug for HF.. 3095 Patients were included between December 2015 and August 2017. 84% Of patients had NYHA functional class II or III. Median LVEF was 30% . Of 3093 patients, 61% were receiving ACEi/ARB, 12.9% were receiving ARNI, and 82.7% a BB. 78% had SBP>110mm Hg Analysis of the contemporary CHAMP-HF cohort of HFrEF patients revealed that an overwhelming majority of patients eligible for either BB or ACEi/ARB/ARNI were not receiving target doses. Most patients were on less than 50% of guideline-recommended target doses.
- 39. Angina Rate pressure product = SBP *HR Increases the duration of diastole
- 41. arrhythmias
- 42. Valvular heart disease Mitral stenosis with Atrial fibrillation Mitral valve prolapse
- 43. Aortic dissection IV betablockers to be used
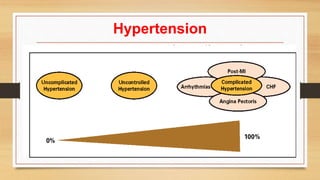
- 44. Hypertension
- 46. The evidence for a J – curve phenomenon calls for caution especially inpatients with angina treated with vasoactive drugs leading to low SBP and HR values.
- 49. Myths vs facts
- 50. 1. Lethargy
- 51. 2.Diabetes
- 53. 3.COPD
- 54. 4.Acute Decompensated Heart Failure
- 56. 6. Peripheral Artery Disease
- 57. 7.perioperative
- 59. caution 1.slow titration – initiation over two weeks, deterioration over one week. 2.abrupt stoppage of drug is problematic 3.
- 60. BISOPROLOL
- 61. MMP- MEDICINE MANAGEMENT PROGRAM
- 67. The Cardiac Insufficiency Bisoprolol Study (CIBIS) studied bisoprolol,a highly selective antagonist of β1 adrenoceptors, which are found mainly in the heart and especially in ventricular tissue. That trial showed a non-significant trend towards 20% lower mortality in the bisoprolol group and 30% fewer admissions to hospital for worsening heart failure.
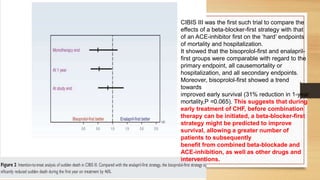
- 73. CIBIS III was the first such trial to compare the effects of a beta-blocker-first strategy with that of an ACE-inhibitor first on the ‘hard’ endpoints of mortality and hospitalization. It showed that the bisoprolol-first and enalapril- first groups were comparable with regard to the primary endpoint, all causemortality or hospitalization, and all secondary endpoints. Moreover, bisoprolol-first showed a trend towards improved early survival (31% reduction in 1-year mortality,P =0.065). This suggests that during early treatment of CHF, before combination therapy can be initiated, a beta-blocker-first strategy might be predicted to improve survival, allowing a greater number of patients to subsequently benefit from combined beta-blockade and ACE-inhibition, as well as other drugs and interventions.
- 74. The Cardiac Insufficiency Bisoprolol (CIBIS) III trial examined the optimum order of initiating CHF treatment in 1010 patients (65 years), with stable, mildly, or moderately symptomatic, systolic CHF. Patients were randomized to initial monotherapy with bisoprolol for up to 6 months, followed by the addition of enalapril, or the opposite sequence. Mean follow-up was 1.2 years. The bisoprolol-first and enalapril-first strategies showed similar efficacy for the combined primary endpoint of mortality or all-cause hospitalization, and similar safety. Compared with the enalapril-first strategy, the bisoprolol-first strategy significantly reduced sudden death during the first year on treatment by 46% (P , 0.05). Patients who achieved higher doses of the study drugs (particularly bisoprolol) had substantially and independently lower mortality and hospitalization risks. Thus, CIBIS III supports a free choice between bisoprolol and enalapril as initial therapy for stable, mild-to-moderate, systolic CHF, and suggests that early beta-blockade reduces the risk of CIBIS III – SUMMARY
- 77. Not proven in Pulmonary hypertension Endstage live disease
- 78. Take home message Beat blockers are the keys drugs in heart failure, with significant mortality benefit. Beta blockers are indicated in complicated hypertension not in uncomplicated hypertension. Most of the BB are withdrawn because of lethargy,which lasts for few weeks only. All benefits are not class effects, to be chosen individually. Abrupt withdrawal of drug is not to be done. Not to be used in patients with cocaine usage.
- 79. THANK YOU
Editor's Notes
- #71: In a multicentre double-blind randomised placebo controlled trial in Europe, enrolled 2647 symptomatic patients in NYHA III or IV, with LVEF 35% or less receiving standard therapy with diuretics and inhibitors ofangiotensin-converting enzyme. Randomly assigned patients bisoprolol 1·25 mg (n=1327) or placebo (n=1320) daily, the drug being progressively increased to a maximum of 10 mg per day. Patients were followed up for a mean of 1·3 years. Analysis was by intention to treat. Findings CIBIS-II was stopped early, after the second interim analysis, because bisoprolol showed a significant mortality benefit. All-cause mortality was significantly lower with bisoprolol than on placebo (156 [11·8%] vs 228 [17·3%] deaths with a hazard ratio of 0·66 (95% CI 0·54–0·81, p<0·0001). There were significantly fewer sudden deaths among patients on bisoprolol than in those on placebo (48 [3·6%] vs 83 [6·3%] deaths), with a hazard ratio of 0·56 (0·39–0·80, p=0·0011). Treatment effects were independent of the severity or cause of heart failure.