












































canted occlusal plane
- 1. Management of cantED occlusal PLANE Presented by:- Kumar adarsh
- 2. Contents:- • Introduction • Etiology • Evaluation • Management • Conclusion • References
- 3. Occlusal cant • Occlusal plane canting in the vertical plane is one of the parameters affecting smile esthetics and originates from facial asymmetry and/or vertical position asymmetry of the right and/or left quadrants of the dental arches without facial asymmetry.
- 4. • Symmetric growth and development enables the conservation of the angles between the cranial planes and OP during an increase in vertical dimensions. • Although changes in the inclination of the OP in the sagittal plane are associated with growth and development, changes in the inclination of the OP in the vertical plane result from asymmetric growth of the craniofacial structures and lead to an asymmetric OP; this is defined as OC.
- 5. • Occlusal cant is frequently associated with facial asymmetry; the reported frequency of facial asymmetry in cases involving this condition varies between 21% and 80%. • This wide range may result from differences between reports in characteristics of facial deformity, types of skeletal malocclusion ,age, or ethnicity. PREVALENCE
- 6. • Good et al indicated that the incidence of asymmetry increases in patients with skeletal class III malocclusion and increased lower facial height. • According to Severt and Proffit, OC is found in 41% of patients with class III malocclusion.
- 7. • Oliveres et al concluded that an OC of 2⁰ was acceptable to lay persons, general dentists, and orthodontists. • Lay persons failed to detect the existence of an OC reaching 3–4º. • Padwa et al concluded that 4⁰ is the threshold for detection of OC.
- 8. “When the vertical dimention of the growing face is altered, significant structural adaptations occur throughout the craniofacial complex” ETIOLOGY (Ref:-Thompson & Brodie, 1942; Breitner, 1943; Sergl & Farmand, 1975; McNamara,1977; Altuna & Woodside, 1985)
- 9. HEREDITARY Cleft lip and palate Hemifacial microsomia Juvenile idiopathic arthritis Treacher Collins syndrome Albright syndrome Crouzon syndrome Craniosynostosis
- 10. ENVIRONMENTAL Facial trauma and fractures (prenatal and postnatal) Jaw cysts, and facial tumors Teratogens Hormonal disorders (such as gigantism or acromegaly) posture Temporomandibular joint (TMJ) ankylosis Habits such as mouth breathing, finger or lip sucking, longterm bottle or pacifier use Incorrect use of force during orthodontic treatment or when using midline elastics
- 12. Evaluation of Occlusal Cant clinical assessment frontal photographs Cephalometry 3-dimensional imaging methods
- 15. Cephalometry
- 16. SMV radiographs • In the presence of asymmetry, basilar/submentovertex (SMV) radiographs are also useful. • The SMV radiographs allow the assessment of asymmetry within each component part of the craniofacial complex as well as the relative relationship of these parts to one another. • In addition, SMV radiographs are less vulnerable to head rotation • The SMV radiographs can be used to diagnose dental arch deviations resulting from • midline shifts • craniofacial asymmetry • condylar position in functional mandibular deviation • maxillary asymmetry in cleft lip and palate patients • mandible asymmetry.
- 17. Orthopantomograms • Orthopantomograms provide information about mandibular asymmetry. • Habets et al described condylar height symmetry calculated by condylar and ramus heights on orthopantomograms.
- 19. OC Management: Treatment Alternatives Orthognathic surgery orthodontic therapy a combination of orthognathic surgery and orthodontic therapy
- 22. Orthognathic surgery • Factor:- • patient’s self awareness of the esthetic problem • severity of the OC • jaw discrepancy in sagittal and vertical directions • Leveling of the OP is generally required before surgery. • single or double jaw surgery-in patients with dramatic OC • to correct • facial and maxillary midline deviation, • level the oral commissure, • obtain symmetric display of the canine teeth, and • correct chin deviation according to the normal facial midline.
- 23. • A combination of Le Fort I osteotomy and mandibular bilateral sagittal split osteotomy or internal vertical ramus osteotomy • The selection of the side for vertical movement depends on • maxillary incisor display, • OP angle in the sagittal direction, and • anterior vertical facial height.
- 24. • maxillary vertical elongation. • hemifacial microsomia, • craniofacial asymmetry, and • cleft lip and palate, • soft tissue defects and • decreased vertical height
- 28. orthodontic therapy • Posterior bite-blocks or high-pull headgear has been used to intrude the molars conventionally. Both of these methods require significant patient cooperation. With either method, it is difficult to control the direction and quantity of tooth movement. • With the advent of temporary skeletal anchorage devices (TSADs), orthodontic molar intrusion and occlusal plane canting correction have been reported, with minimal surgical intervention.
- 29. • Kang et al introduced a rhythmic arch system using TSADs and obtained a considerable amount of canting correction. • Jeon et al reported correction of mandibular prognathism with mandibular surgery only, correcting the maxillary asymmetry by intrusion of the maxillary molars unilaterally using TSADs. • However, the treatment times were extended, increasing the risk of side effects
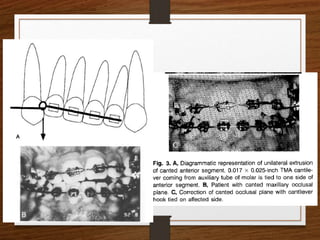
- 30. • Canted ant occlusal plane • Vertical interarch elastic • One piece intrusion arch • U/L cantilever • Canted posterior occlusal plane • Variation of intrusion arch • Preccision palatal arch in maxillary &/or precision lingual arch in mandible
- 39. Correction of a Canted Lower Incisal Plane Ref:-JCO,2006;VOLUME XL NUMBER 9
- 40. Skeletal anchorage • occipital headgear • removable appliances with elastics (McNamara,1977; Altuna & woodside,1985) • modified palatal appliances • elastomeric chain • magnets • miniscrews and miniplates • corticotomy-enhanced intrusion
- 41. Management of occlusal canting with miniscrews Angle Orthod, Vol 84, No 4, 2014
- 42. A combination of orthognathicsurgery and orthodontictherapy • skeletal anchorage (miniscrews or miniplates) in the maxilla and orthognathic surgery in the mandible • sagittal split ramus osteotomy and genioplasty and/or intraoral vertical ramus osteotomy
- 43. • Since Kole suggested clinical applications of corticotomy in 1959, various technical advancements have been reported. • One is orthopedic force application against intraosseous anchorage after corticotomy. • A heavier force is applied than the orthodontic force because the aim of this technique is not tooth movement through the bone but rather bony block movement by compression osteogenesis. • If the cortical layer of the basal and alveolar bone is removed, medullary bone can be bent by traction force.
- 44. (ref:-Ahn HW et al; Correction of facial asymmetry and maxillary canting with corticotomy and 1-jaw orthognathic Surgery;Am J Orthod Dentofacial Orthop 2014;146:795-805)
- 45. CONCLUSION • Occlusal plane canting in the vertical plane is one of the parameters affecting smile esthetics and originates from facial asymmetry and/or vertical position asymmetry of the right and/or left quadrants of the dental arches without facial asymmetry. • To obtain satisfactory treatment results in individuals with OC, the etiologic factors of OC should be examined, the classification of OC should be considered, and the benefits of alternative treatment choices should be discussed.
- 46. References • Dixon AD, Hoyte DAN, Ronning O. Fundamentals of Craniofacial Growth. Boca Raton, FL: CRC Press; 1997. • JCO,2006;volume xl number 9 • Semin Orthod 1998;4:153-164
Editor's Notes
- #11: Recently, the number of patients referred to orthodontic clinics as a result of TMJ disorders has been increasing. In patients with unilateral TMJ disorder, facial asymmetry is less associated with occlusal discrepancy; however, canting of the OP in these patients is increased because of mandibular hypoplasia on the affected side
- #13: Grummons frontal analysis and Sassouni analysis. Occlusal cant is related to the pattern of skeletal and/or dentoalveolar development and can be classified with or without facial asymmetry due to asymmetric development of the mandible, unilateral extruded molars, or asymmetric dentoalveolar development.
- #15: The evaluation of frontal facial photographs is a diagnostic tool used to evaluate soft-tissue asymmetry and lip cants. It was concluded that an OP angle of 2.15–2.90 degree on a digital photograph is acceptable. The incidence of a cant greater than 1degree between the bilateral mouth corners was found to be 28.6% when the face was measured on standardized frontal facial photographs
- #16: The following landmarks were identified and traced: supraorbital rims (ST), crista galli (cg), nasal septum (IX), piriform apertures (pa), mandibular angles (ma), and maxillary molars (mm). A vertical reference line was drawn from the top of cg through a point on the superior ns at the level of the equator of the globe and ethmoid sinuses (dotted line). A horizontal line was drawn perpendicular to the vertical and tangent to sr. The occlusal plane was drawn as a tangent to mm cusps. Occlusal cant was determined by measuring the angle of the maxillary plane in relation to the horizontal line. This patient had an occlusal cant of 0”.
- #23: invasive and expensive valid in patients with OC and/or facial asymmetry
- #37: About 1mm of intrusion can be expected every six weeks 40-60g force