Controlled drug release
Download as PPTX, PDF75 likes18,103 views

This document discusses various oral controlled release drug delivery systems. It describes dissolution controlled systems like encapsulation and matrix dissolution control where drug release is controlled by the rate of dissolution of a coating. Diffusion controlled systems like reservoir and matrix devices are also discussed where the rate of drug release depends on diffusion through a coating membrane. Combined dissolution and diffusion systems and ion exchange resins are also summarized. The document provides details on different types of controlled release tablets and their drug release mechanisms.

























Controlled drug release
- 1. ORAL CONTROLLED RELEASE DRUG DELIVERY SYSTEMS
- 2. The majority of oral controlled release systems rely on dissolution, diffusion, or a combination of both mechanisms to generate slow release of drug to the gastrointestinal milleu. A. DISSOLUTION CONTROLLED RELEASE: Sustained release oral products employing dissolution as the rate-limiting step are in principle the simplest to prepare. 1. Encapsulation dissolution control: These methods generally involve coating individual particles or granules of drug with a slowly dissolving material. The coated particles can be compressed directly into tablets as in Spacetabs or placed in capsules as in the Spansule Products. Since the time required for dissolution of the coat is a function of its thickness and aqueous solubility, one can obtain repeat or sustained action by employing a narrow or a wide spectrum of coated particles of varying thicknesses respectively
- 4. 2. Matrix dissolution control: An alternative approach is to compress the drug with a slowly dissolving carrier of some sort into a tablet form. Here, the rate of drug availability is controlled by the rate of penetration of the dissolution fluid into the matrix. This, in turn, can be controlled by porosity of the tablet matrix, the presence of hydrophobic additives, and the wettability of the tablet and particles surface. B. DIFFUSION CONTROLLED RELEASE: There are basically two types of diffusion controlled systems which have been developed over the past two decades, reservoir devices and matrix devices.
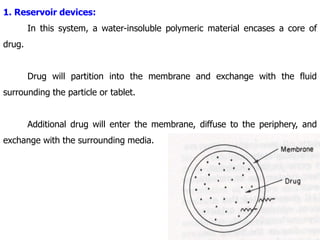
- 5. 1. Reservoir devices: In this system, a water-insoluble polymeric material encases a core of drug. Drug will partition into the membrane and exchange with the fluid surrounding the particle or tablet. Additional drug will enter the membrane, diffuse to the periphery, and exchange with the surrounding media.
- 6. 2. Matrix devices: In this system, a solid drug is dispersed in an insoluble matrix. The rate of drug release is dependent on the rate of drug diffusion but not on the rate of solid dissolution.
- 7. C. DIFFUSION AND DISSOLUTION CONTROLLED SYSTEMS: The main feature of this system is that the drug core is enclosed with a partially soluble membrane. Dissolution of part of the membrane allows for diffusion of the contained drug through pores in the polymer coat.
- 8. D. ION-EXCHANGE RESINS: Resins are water-insoluble materials containing anionic or cationic groups in repeating positions on the resin chain. The drug-charged resin is prepared by mixing the resin with drug solution either by repeated exposure of the resin to the drug in a chromatographic column or by keeping the resin in contact with the drug solution for extended periods of time. Polymer- coated drug-resin design Polymer- coated drug-resin dispersion
- 9. The drug-resin is then washed to remove contaminant ions and dried to form particles or beads. When a high concentration of an appropriately charged ion is in contact with the ion-exchange group, the drug molecules is exchanged and diffuses out of the resin to the bulk solution. E. pH - INDEPENDENT FORMULATIONS: The granules are designed for the oral controlled release of basic or acidic drugs at a rate that is independent of the PH in the GI tract. They are prepared by mixing a basic or acidic drug with one or more buffering agents, granulating with appropriate pharmaceutical excipients, and finally, coating with a gastrointestinal fluid permeable film-forming polymer. When the GI fluid permeates through the membrane, the buffering agents adjust the fluid inside to a suitable constant pH, thereby rendering a constant rate of drug release.
- 10. F. OSMOTICALLY CONTROLLED RELEASE: In this type of drug delivery systems, osmotic pressure is the driving force that generates constant drug release. This system is fabricated by applying a semipermeable membrane around a core of an osmotically active drug or a core of an osmotically inactive drug in combination with an osmotically active salt. A delivery orifice is drilled in each system by laser or by a high –speed mechanical drill. The elementary osmotic pump Osmotic pressure-controlled drug delivery system with compartments separated by a movable partition
- 11. G. ALTERED DENSITY FORMULATIONS: It is reasonable to expect that unless a delivery system remains in the vicinity of the absorption site until most, if not all of its drug contents is released, it would have limited utility. To this end, several approaches have been developed to prolong the residence time of drug delivery systems in the GI tract. One such approach is the bioadhesion approach, which is based on the adherence of bioadhesive polymers to the mucin / epithelial surface of the GI tract. The other approach is to alter the formulation’s density by using either high or low density pellets.
- 12. 1. High – density approach: In this approach, the density of the pellets must exceed that of normal stomach content and should therefore be at least 1.4. In preparing such formulations, drug can be coated on a heavy core or mixed with heavy inert materials such as barium sulfate, titanium dioxide, iron powder, and zinc oxide. The weighed pellet can then be covered with a diffusion controlled membrane.
- 13. 2. Low-density approach: Globular shells which have an apparent density lower than that of gastric fluid can be used as carrier of drug for sustained release purposes. Polystyrol, poprice, and even popcorn are all candidates as carriers. The surface of these empty shells is undercoated with sugar or with a polymeric material such as methacrylic polymer and cellulose acetate phthalate. Drug delivery system with flotation chamber
- 14. The undercoated shell is then coated by a mixture of drug with polymers such as ethyl cellulose and hydroxy propyl cellulose. The final product floats on the gastric fluid for a prolonged period, while slowly releasing drug. TYPES OF TABLETS: 1. MATRIX TABLETS: There are three types of matrix tablets 1. Hydrophilic matrices 2. Plastic matrices 3. Fatwax matrices
- 15. 2. ION-EXCHANGE RESIN TABLETS: The tablets are commonly developed by embedding the drug molecules in the ion-exchange resin matrix and then this core is coated with a semi permeable coating material such as ethyl cellulose. The most widely used and safe ion exchange resin is divinyl benzene sulphonate. Drugs that were prepared using cationic exchange resins include codeine, ephedrine.
- 16. 3. FILM COATED TABLETS: Simple coating of the tablets by the polymers can control the dissolution rate of drug from the tablets. Various polymers such as H.P.M.C, E.C & Eudragit polymers have been used for the polymeric film coating of the tablets. These polymer coatings act as diffusion controlling membranes. The selection of coating material will decide the dissolution rate of the drug molecules. Plasticizers also accelerate the drug release.
- 17. 4. FLOATING TABLETS: Floating tablets can be used for local action in the proximal G.I.T. Poorly soluble and unstable as well as poorly absorbable drugs are suitable for floating dosage units. These systems are retained in the stomach for prolonged time due to their floating property. Floating dosage forms have been developed to float over G.I fluids &to release the drug over a desired period of time. Increased G.I time is the consequent property of floating tablets. Drugs suitable to be formulated as floating tablets --morphine --captopril --diazepam
- 18. 5. ENTERIC COATED &DELAYED RELEASE TABLETS: The materials used for enteric coating are acid impermeable polymers. An ideal enteric coating should dissolve at a pH slightly lower than 7. Various solvents such as alcohol, acetone, and methylene chloride have been used to dissolve the enteric coating polymers. Ex: 1. Aspirin given as enteric coated tablets prevents gastric irritation. 2. Erythromycin degrades in gastric pH. Hence, it is given as prodrug/enteric coated formulation. The enteric coating formulation needs higher pH 6.5-7.0 for disintegration of coating, which delays the release of erythromycin beyond the absorption site. Here, efficacy of formulation depends on selection of suitable polymer.
- 19. 6. OSMATIC TABLETS: The osmotic tablets are comprised of a drug contained in a rigid, semi permeable membrane in which an aperture is created by a mechanical drill or laser beam. These systems are suitable for the soluble drugs such as indomethacin & metoprolol. Semi permeable polymers such as cellulose acetate & polyurethane are commonly used for osmotic tablet formulations. 7. MUCOADHESIVE TABLETS: They are developed for administration of drug to the oral cavity. Buccal & sublingual mucosa offer for mucoadhesion. Drug can be applied locally and removed. Synthetic polymers including cellulose derivatives & polyacrylic acid are used for preparation of bioadhesive tablets.
- 20. 8. SWELLABLE TABLETS: The dosage forms can be developed in a size, which can be swallowed & when they reach the stomach fluid swell quickly & attain considerably large size. In addition to swelling, gel forming property of the polymer can retain the drug molecules within the dosage form thereby sustaining the release of drug from the formulation. 9. MULTIPLE UNIT TABLETS: They contain subunits that are homogenous or heterogenous They are prepared by combining the immediate release portion & controlled release portion.
- 21. 10. MICROCAPSULES & MICROSPHERES: The mechanism of drug release is either dissolution or diffusion of the drug & the formulation are either microencapsulated or matrix Various methods including interfacial polymerization, coacervation/phase separation are used to prepare micro particles. The coating material should be selected depending on the material to be coated & the release characteristics desired.
- 22. EVALUATION DISSOLUTION RATE - ASSESSMENT: DEMONSTRATION OF SAFETY AND EFFICACY OF CONTROLLED RELEASE DRUGS: 1. For drugs that have been approved by the FDA as safe and effective in conventional dosage forms, the Food and Drug Administration has taken the position that controlled clinical studies may be required to demonstrate the safety and efficacy of the drugs (already approved for use in conventional forms) in the controlled release formulations. In any case, bioavailability data for the drug (s) in the controlled release formulation are required. 2. For drugs that have been previously approved as safe and effective in controlled release dosage forms, data are required to establish bioavailability comparability to an approved controlled release drug product.
- 23. 3. Single dose bioavailability studies are acceptable for determining the fraction of the amount absorbed, lack of dose dumping, lack of food effects. etc. Pharmacokinetic studies, performed under study – state conditions, are acceptable to demonstrate comparability to an approved immediate release drug product, occupancy time with in a therapeutic window, percent fluctuation, etc, and are acceptable for supporting dosage administration labeling. 4. The optimum single dose study would be a three – way cross over comparing a rapidly available dosage form and the controlled release dosage form under fasting conditions with the controlled release form administered immediately after the ingestion of high fat meal. If significant differences are found in AUC and peak concentrations as a function of the meal, it is necessary to define the cause of the food effect. With drugs having a narrow therapeutic index, it might be necessary to carry out more extensive plasma concentration measurements in patients to determine the potential for unusual drug release patterns.
- 24. 1. Biopharmaceutical considerations: The invitro test was desirable for the purposes of A. Providing necessary process control and stability determinations of the relevant release characteristics. B. Facilitating certain regulatory determinations and judgments, concerning minor formulation changes, site of manufacturing change, etc. The key elements for the dissolution are: 1. Reproducibility of the method. 1. Proper choice of media. 2. Maintenance of sink conditions 3. Control of solution hydrodynamics. 4. Dissolution rate as a function of pH ranging from pH 1 to pH 8, 5. Selection of the most discriminating variables as the basis for the dissolution test and specification.
- 25. The dissolution procedure should establish: 1. Lack of dose dumping – indicated by a narrow limit on the one hour dissolution specification. 2. Controlled release characteristics – by employing additional sampling windows overtime. 3. Complete drug release – indicated by a 75 – 80 % minimum release specifications at the last sampling interval. 4. Dosage form pH dependence / independence indicated by percent dissolution in water, appropriate buffer, gastric and simulated intestinal fluid.
- 26. Invivo bioavailability data: A. General: B. Specific types of in vivo studies: 1. Fasted single – dose studies: 2. Post prandial study: 3. Multiple – dose study – state studies: