




















































spinal cord injury ppt
- 1. SPINAL CORD INJURY Mrs. Mamta Toppo Associate Professor College of Nursing RIMS , Ranchi Neetu Kumari Roll no – 11 3rd year basic B.sc. Nursing Session – 2017 -21
- 2. CONTENT 1. Anatomy and Physiology of Spinal Cord 2. Introduction 3. Definition 12. Different surgeries for SCI 4. Incidence 13. Halo and orthotic devices 5. Risk factor 14. Nutritional Diet 6. Causes 15. Complications 7. Pathophysiology 16. Prognosis 8. Clinical Manifestation 17. Rehabilitation of SCI 9. Types 18. Recent Research 10. Diagnostic Evaluation 19. Summary 11. Management 20. Reference a. Emergency Management 21. Bibliography b. Medical Management c. Surgical Management d. Nursing Management
- 5. The SPINAL CORD is a part of the Central Nervous System. It is a long pipe- like structure arising from the Medulla oblongata part of the brain consisting of a collection of nerve fibres , running through the Vertebra column of the Backbone. In adults , the spinal cord is usually 40cm long and 2cm wide. It form a vital link between the brain and the body. The Spinal cord is divided into five different parts :-
- 6. 1. CERVICAL CORD :- Cervical means of the Neck. There are 8cevicalnerves that emerge from the cervical spine (C1 - C8). 2. THORACIC CORD :- Thoracic means of the Chest. There are 12 thoracic nerves that emerge from the thoracic spine (T1 – T12). 3. LUMBAR CORD:- Lumbar means from the lower back region . There are 5 lumbar nerves that emerge from the lumbar spine (L1 – L5). 4. SACRAL CORD :- Sacral means of the sacrum. The sacrum is a bony plate at the base of the vertebral column. There are 5 sacral nerves that emerge from the sacral bone (S1- S5). 5. COCCYGEAL CORD :- Coccygeal means of theTailbone. There is 1 nerve that emerges from the coccygeal bone.
- 7. FUNCTIONS OF SPINAL CORD Carrying signals from the brain:- The spinal cord receives signals from the brain that control movement and autonomic functions. Carrying information to the brain :- The spinal cord nerves also transmit messages to the brain from the body , such as sensations of touch , pressure and pain. Reflex responses :- The spinal cord may also act independently of the brain in conducting motor reflexes. Forms a connecting link between the brain and the PNS. Provides structural support and builds a body posture. Facilitates flexible movements.
- 8. INTRODUCTION The spinal cord is a collection of nerves that travels from the bottom of the brain down your back. There are 31 pairs of nerves that leave the spinal cord and go to arms, legs, chest and abdomen. These nerves allow your brain to give commands to your muscles and cause movements of your arms and legs.
- 9. DEFINITION Spinal cord injury (SCI) is damage or trauma to the spinal cord that results in a loss of impaired function causing reduced mobility or sensation. The cervical and lumbar vertebrae are the most common sites of injury.
- 10. INCIDENCE o SCI is highest among persons age 16-30, in whom 53.1% of injuries. o Males represent 81.2% of all reported SCIs and 89.8% of all sports related SCIs. o Among both genders , auto accidents , falls and gunshots are the three leading causes of SCIs. o Sports and recreation related SCI injuries primarily affect people under age 29.
- 11. RISK FACTORS Male sex Age between 18 to 25 years Young adults and seniors People who are active in sports People with predisposing conditions
- 12. CAUSES • Trauma • Loss of its normal blood supply • Infectious conditions • Extreme twisting of the middle of the body • Gunshot wounds • Inflammation of the spinal cord • Acts of violence • Spinal cord tumor • Falls from a great height • Sports and recreation injuries • Electric shock • Motor vehicle accidents • Multiple sclerosis
- 13. PATHOPHYSIOLOGY Damage to the Spinal cord ranges from transient concussion to contusion , laceration and compression of the cord substance to complete transection of the cord. Spinal cord injuries can be separated into two categories - Primary injuries are the result of the initial insult or trauma and are usually permanent. Secondary injuries are usually the result of a contusion or tear injury in which the nerve fibres begin to swell and disintegrate.
- 14. An injury to the upper portion of the spinal cord in the neck can cause quadriplegia paralysis of both arms and both legs. If the injury to the spinal cord occurs lower in the back , it can cause Paraplegia paralysis of both legs only.
- 16. CLINICAL MANIFESTATION Symptoms vary depending on the location of the injury. The most common sites are the cervical areas C5,C6 and C7 and the junction of the thoracic and lumbar vertebrae T12,L1. CERVICAL {NECK} INJURIES :- o Breathing difficulties o Loss of normal bowel and bladder control o Numbness o Sensory changes o Spasticity ( increased muscle tone)
- 17. THORACIC { CHEST LEVEL } INJURIES :- o Loss of normal bowel and bladder control o Numbness o Sensory changes o Spasticity (increased muscle tone) o Weakness , paralysis LUMBAR SACRAL {LOWER BACK} INJURIES :- o Loss of normal bowel and bladder control ( you may have constipation, leakage and bladder spasms) o Numbness o Pain o Sensory changes o Weakness and paralysis
- 19. Complete Spinal Cord Injuries It is described as absence of sensory and motor function in lowest sacral segment after resolution of spinal shock. 1. TETRAPLEGIA :- Spinal cord injury above the first thoracic vertebrae, or within the cervical sections of C1 – C8. Result is some degree of paralysis in all four limbs – the legs and arms. 2. PARAPLEGIA :- Spinal cord injury below the first thoracic spinal levels ( T1 – L5). Paraplegia are able to fully use their arms and hands , but the degree to which their legs are disabled depends on the injury.
- 20. Incomplete Spinal Cord Injuries It is defined as the presence of sensory and motor function in lowest sacral segment . 1. CENTRAL CORD SYNDROME :- CAUSE :- Injury or edema of the central cord , usually of the cervical area and cervical lesions. CHARACTERISTICS :- Motor deficits (in the upper extremities sensory loss varies in the upper extremities).
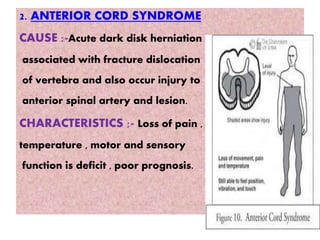
- 21. 2. ANTERIOR CORD SYNDROME CAUSE :-Acute dark disk herniation associated with fracture dislocation of vertebra and also occur injury to anterior spinal artery and lesion. CHARACTERISTICS ;- Loss of pain , temperature , motor and sensory function is deficit , poor prognosis.
- 22. 3. BROWN – SEQUARD SYNDROME CAUSE :- The lesion is caused by a transverse hemi-section of the cord , as a result of a knife or missile injury , fracture, dislocation of a unilateral articular process. CHARACTERISTICS :- Ipsilateral paralysis or together with ipsilateral loss of touch , pressure ,vibration and contralateral loss of pain and temperature.
- 23. DIAGNOSTIC EVALUATIONS o Spine x-ray o CT Scan or MRI of the spine o CBC (e.g. Hb , RBC , WBC) o Arterial blood gas level
- 25. EMERGENCY MANAGEMENT Emergency management of patient with spinal cord injury includes a rapid assessment , immobilization , stabilization or control of life - threatening injuries and transportation to the most appropriate medical facility. Emergency management involves careful monitoring of vital signs and airway and keeping the patient immobilized.
- 26. MEDICAL MANAGEMENT o Respiratory Management :- The goal of care of patient with spinal cord injury is maintenance of pulmonary and cardiovascular stability. Patient may require oxygen therapy , tracheostomy and continuous mechanical ventilation. o Pharmacologic Therapy :- Corticosteroids , such as dexamethasone or methylprednisolone , are used to reduce swelling that may damage the spinal cord. o Immobilization :- Spinal traction may be recommended. A special bed may help immobilize body such as Roto Rest bed and Stryker. o Supportive Therapy :-
- 27. SURGICAL MANAGEMENT o Surgery is necessary to remove fragments of bones , foreign objects , herniated disks or fractured vertebrae that appear to be compressing the spine. o If the spinal cord is being compressed by tumor , infection or severe arthritis , surgery can be performed to reduce the amount of compression. o Surgery may also be needed to stabilize the spine to prevent future pain or deformity.
- 28. NURSING MANAGEMENT ASSESSMENT :- o Disturbance in level of consciousness from slightly drowsy to unconscious. o Sudden onset of neurologic deficits. o Cerebrospinal fluid leakage at ears and nose , which may indicate skull fracture. o Irregular respirations. o Puppillary abnormality.
- 29. DIAGNOSIS :- o Impaired physical mobility related to loss of motor function. o Fluid volume deficit related to decrease loss of consciousness. o Risk for injury related to loss of motor function. o Urinary retention related to inability to void spontaneously. o Pain and discomfort related to treatment and prolonged immobility. o Knowledge deficit regarding the treatment modalities and current situation.
- 30. PLANNING :- o Improved breathing pattern and airways clearance. o Improved mobility. o Improved sensory and perceptual awareness. o Maintenance of skin integrity. o Relief of urinary retention. o Improved bowel function. o Promotion of comfort.
- 31. INTERVENTIONS :- o Monitor respiratory rate , depth and pattern of the respirations. o Promote adequate breathing and airway clearance. o Range of motion exercises help to prevent contractures. o Place the patient on special beds that move the patient frequently without the need for turning. o Assess all body surfaces and document skin integrity at least every 8 hours. o Turn reposition the patient every 2 to 4 hours. o Assess the bladder distension , urinary and bowel function and elimination. o Record fluid intake , voiding pattern , amount of residual urine after catheterization. o Provide high fiber and high protein diet.
- 32. DIFFERENT SURGERIES FOR SCI o SPINAL FUSION :- It is a surgical procedure used to correct problems with the small bones in the spine (vertebrae). It is essentially a “welding” process. The basic idea is to fuse together two or more vertebrae so that they heal into a single , solid bone. This is done to eliminate painful motion or to restore stability to the spine.
- 33. DECOMPRESSION LAMINECTOMY It is a type of surgery in which a surgeon removes part or all of the vertebral bone (lamina). This helps ease pressure on the spinal cord or nerve roots that may be caused by injury , herniated disk or narrowing of the canal.
- 34. FORAMINO- TOMY This surgery is used to relieve pain associated with a compressed nerve in the spine. The surgeon cuts away bone at the sides of your vertebrae to widen the space where nerves exit your spine.
- 35. DISC REPLACEMENT A surgeon removes the damaged spinal disk and inserts an artificial one between your vertebrae.
- 36. INTERLAMINAR IMPLANT This is a minimally invasive alternative to more invasive laminectomy or laminectomy plus fusion surgery. The surgeon implants a U- shaped device between two vertebrae in lower back. It helps keep the space between them open and eases pressure on spinal nerves. It can be done at the same time as a laminectomy.
- 37. HISTORY o 5,000 years ago nearly Ancient Egyptians used first splints. o Middle ages armorers manufactured splints that protected as well as stabilized the body. o Late 16th century french surgeon Ambroise Pare developed metal corsets. o Late 17th century Lorenz Heister is created with developing the first spinal orthosis quite similar to the modern day halo brace.
- 38. HALO AND ORTHOTIC DEVICES FOR SCI Cervical – Thoracic Orthosis Lumbosacral Orthosis
- 39. Cervico – Thoraco - Lumbosacral Orthosis (CTLSO) Thoraco – Lumbo - Sacral Orthosis (TLSO)
- 41. NUTRITIONAL DIET o Eat a variety of foods such as whole grains , fruits and vegetables o Protein foods such as lean meats , eggs or legumes and low or non fat dairy products. o Eat foods high in fiber – fiber adds bulk to stool , making it easier to pass and prevent bowel problem. o Avoid the too much salt intake. o Eat less of foods high in fat and sugar. o Should drink plenty of water.
- 42. COMPLICATIONS IMMEDIATE COMPLICATION :- o Respiratory arrest o Spinal shock LONG – TERM COMPLICATION :- o Autonomic dysreflexia o Pressure ulcers o Urinary tract infection o Contractures o Respiratory tract infection o Calcium loss from the bones
- 43. PROGNOSIS o Patients with a complete cord injury have a less than 5% chance of recovery. o If complete paralysis persists at 72 hours after injury , recovery is essentially zero. o The prognosis is much better for the incomplete cord syndrome. o If some sensory function is preserved , the chance that the patient will eventually be able walk is greater than 50%. o Ultimately , 90% of patients will SCI return to their homes and regain independence.
- 44. REHABILITATION OF SCI “It is a measures that help individuals with a disability or a disabling health condition achieve and maintain optimum functioning in interaction with their environments”. GOAL :- The primary goals of rehabilitation are prevention of secondary complications. Promote recovery and maximize independence.
- 45. TEAM MEMBERS :- Physical therapists typically focus on lower extremity function and on difficulties with mobility. Occupational therapists address upper extremity dysfunction and difficulties in activities of daily living. Rehabilitation nurses are concerned with the issues of bowel and bladder dysfunction and the management of pressure injuries. Psychologists deal with the emotional and behavioral concerns of the newly injured patient and with any potential cognitive dysfunction. Speech-language pathologists address with issues of communication and swallowing.
- 46. Case managers and social workers are the primary interface between the rehabilitation team, the patient and his or her family and the payer source.
- 47. RECENT RESEARCH A Follow-Up Program In India For Patients With Spinal Cord Injury: Paraplegia Safari M. Prabhaka , MS (Ortho) &Tejas H. Thakker , MS (Ortho) Pages 260-262 | Received 13 Jun 2003, Accepted 06 Nov 2003, Published online: 02 Sep 2016 Abstract Background: Once patients with spinal cord injury (SCI) were discharged from the hospital, it was very difficult for them to return for follow-up, particularly during the first year, due to problems
- 48. regarding finances and social issues, as well as extreme physical barriers. Because of these barriers, a large number of patients were presenting for re- admission for reasons that might have been prevented if they had come for routine follow-up. Therefore, it was felt that an attempt to visit the patient's residence to conduct follow-up would be of great help. Objectives: To evaluate and improve the status of rehabilitation of community-dwelling SCI patients in their homes and attempt to decrease the rate of re-admissions. Material and Methods: ln this program, the home visit team consisted of an orthopedic surgeon, physiotherapist, occupational therapist, prosthetist and orthotist engineer, medical social worker, and a nurse. Rehabilitated discharged patients received needed medical treatment, orthotics, and vocational guidance at their residences. Patients who required re-admission were assisted back to the hospital. Conclusion: The home visit program decreased the number of re-admissions by improving the status of rehabilitation, which raised the quality of care for patients with SCI.
- 49. SUMMARY Spinal Cord Injury (SCI) is a sudden onset disruption to the neuronal tissue within the spinal canal resulting in spinal cord damage , which occurs as a result of trauma , disease or degeneration. Any damage to the spinal cord is a very complex injury. It can present as either an upper motor neuron lesion or lower motor neuron lesion with varying loss of motor , sensory and autonomic function.
- 50. EVALUATION o What do you mean by spinal cord injury? o What is the types of spinal cord injury? o Listed the diagnostic evaluation? o What is the difference between a complete and incomplete spinal cord injury? o What are causes of spinal cord injury? o What is the prognosis of spinal cord injury?
- 51. REFERENCE o Books o Internet o Teacher
- 52. BIBLIOGRAPHY o Ansari Javed , textbook of medical surgical nursing , volume – 2 , PV publications , page no – 312 to 316. o Brunner and Suddarth’s , Textbook of Medical Surgical Nursing , South Asia edition , volume – 2 , Wolters kluwer publications , page no- 1676 to 1682 o www.wikipedia.org o www.slideshare.com