1. TRY-IN procedure in
complete denture
Dr Athira K Nair
1st
Year MDS
Department of Prosthodontics, crown and bridge
and Oral Implantology.
Bharati Vidyapeeth Dental College, Pune.
DATE: 23/02/2022
3. Maxillary Trial Denture itself
Mandibular Trial Denture itself
Both dentures together
Conclusion
References
4. INTRODUCTION
Once the teeth arrangement is done according to the information
secured at the record stage, it is necessary to try the wax-up dentures in
the patient’s mouth before processing them.
It is difficult to make alterations on to a processed denture whereas at
waxed-up stage changes can be made easily.
A technician may arrange artificial teeth, but it is the responsibility of the
dentist to verify the positions of the teeth.
5. DEFINITIONS
1. TRY-IN VERIFICATION :
According to GPT-9,
“A preliminary insertion of a removable denture wax- up or a partial
denture casting or a finished restoration to determine the fit,
aesthetics, maxillomandibular relation.”
6. 2. TRIAL DENTURE :
According to GPT-9,
“A preliminary arrangement of denture teeth that has been prepared
for placement into the patients mouth to evaluate aesthetics &
maxillomandibular relationships”
7. OBJECTIVES
To check and verify the maxillomandibular relationship :
- Verification of established vertical dimension of occlusion
- Verification of centric relation
To determine the position of teeth and contours of the denture base are
compatible in oral cavity.
To evaluate aesthetics and phonetics.
To make additional interocclusal maxillomandibular records if needed.
8. HOW TO GO FORWARD WITH THE
COMPLETE DENTURE TRY IN?
It is important to get into the habit of working to a definite plan.
Following order is suggested:
9. 1. Extra oral examination of trial denture
2. Intra oral examination of trial denture
11. INTRA ORAL EXAMINATION
I. THE MANDIBULAR DENTURE ITSELF
Denture extension:
1. Labial and buccal extension
2. Posterior extension
3. Lingual extension
Stability to occlusal stresses
Tongue space
Lower occlusal plane
12. II. THE MAXILLARY DENTURE ITSELF
Denture extension:
1. Labial and buccal extension
2. Posterior extension
Retention
Stability to occlusal stresses
Orientation of occlusal plane
13. III. BOTH DENTURES TOGETHER
Verification of jaw relation:
1. Verification of vertical dimension
2. Verification of centric relation
3. Eccentric relation records
Evenness of occlusal presssure
Balanced occlusion
14. Evaluation of facial and functional harmony with anterior teeth:
1. Midline
2. Anterior plane
3. Lip form in profile
4. Phonetics
5. Lip line
6. Tooth visibility
7. Characterization
8. Shape, size and shade of the teeth
Approval of appearance from the patient and patient relatives.
15. NOTE:
Before carrying out these checks, remove the trial dentures from the
articulator and place them in a bowl of cold water as the wax softens at
mouth temperature and if kept for long can cause the displacement of
the teeth.
16. EXTRA ORAL EXAMINATION
1. THE MASTER CAST:-
As the finished denture is processed on the master cast. So the master
cast should be:
Has good shape
Free from air bubbles or scratches
17. Free from wax debris which lead to improper adaptation of the trial
denture bases leading to false relationships.
If there are any undercuts present in the cast, these undercuts should
be relieved
18. 2. Trial denture base:-
Must be stable
The borders of the trial denture base should be smooth, round and
no sharp edge.
19. 3. On the articulators:
The mounted cast is checked for:
Maintaining of the vertical dimension of occlusion
The mounting rings are firmly screwed in their position
20. Moving of the articulator smoothly from centric to eccentric positions
without cuspal interlocking
The trial denture bases lie properly on their casts and teeth meet
evenly in centric relation.
21. 4. The teeth:-
It is the responsibility of the dentist to select the proper shade and
size of the teeth and to determine that the teeth are set correctly.
Elimination of the excess wax is done.
22. INTRA ORAL EXAMINATION
To reduce the risk of cross contamination, the trial denture should be
sprayed with suitable antiseptic solution.
First the mandibular denture is placed followed by maxillary denture.
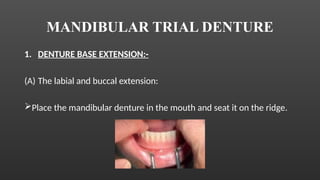
23. MANDIBULAR TRIAL DENTURE
1. DENTURE BASE EXTENSION:-
(A) The labial and buccal extension:
Place the mandibular denture in the mouth and seat it on the ridge.
24. To check for over extension :
Hold the denture in place with light pressure on occlusal surface of
teeth. Pull the cheek upward and inward . Relax the pressure on the
occlusal surface and observe if denture rises from the ridge. *
Adequate clearance of labial and buccal frenum
Note the bulk and shape of the buccal aspect of denture.
It should be in the form of gentle concavity looking outwards and
upwards.*
25. (B) LINGUAL EXTENSION:
Hold the denture in place with light pressure on the occlusal surface
of the teeth
Ask the patient to protrude his tongue sufficiently to moisten his lips
If the denture lifts at the back, it is over extended in the region of
lingual pouch
26. Next, ask the patient to touch the posterior most part of palate with
the tip of his tongue.
If denture lifts in the front, it is over extended in the region of lingual
frenum.
Avoid over trimming. *
28. (D) UNDER EXTENSION
Occurrence : less common
Greater coverage of area will ensure stability and retention.
Gap between the denture and functional position of surrounding
mucous membrane. *
29. 2. STABILITY:
Apply light pressure at right angles in the premolar and molar region
alternatively.
If the pressure on one side causes the denture to tilt and rise from
the ridge on the other side, it indicates that the teeth on which
pressure is applied are outside the ridge
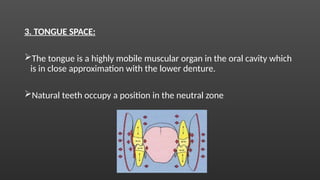
30. 3. TONGUE SPACE:
The tongue is a highly mobile muscular organ in the oral cavity which
is in close approximation with the lower denture.
Natural teeth occupy a position in the neutral zone
31. Artificial teeth also have to be arranged in neutral zone
Tongue being more mobile than the cheeks will cause greater
instability of the denture if the teeth are arranged lingual side of the
neutral zone than if they are on the buccal side of it.
If the tongue is cramped by the denture, lateral pressure will be
exerted – instability of denture as tongue moves
32. CRAMPED TONGUE:
CAUSES:
1. Posterior teeth set inside the ridge
2. Posterior teeth too broad bucco-lingually
3. Posterior teeth tilted lingually *
33. TEST FOR CRAMPED TONGUE:
1. Ask the patient to relax the tongue.
2. Make sure the denture is seated on the ridge.
3. Then ask the patient to raise the tongue
4. If the tongue is cramped then the denture will begin rise
immediately the tongue moves
34. HOW TO DIFFERENTIATE CRAMPED TONGUE AND OVER EXTENSION?
The immediate reaction of the denture tends to differentiate the
movement caused by cramped tongue from the movement caused
by lingual over extension.
Movement caused by lingual over extension occurs when the tongue
has risen some distance.
35. 4. LOWER OCCLUSAL PLANE:
To obtain maximum stability of lower denture, the occlusal plane of
the lower teeth should be very slightly below the bulk of tongue, so
that tongue performs the majority of its movements above the
denture and thus keep the denture down *
36. The posterior end of the occlusal plane should be at the level of the
anterior two-third of the retro molar pad
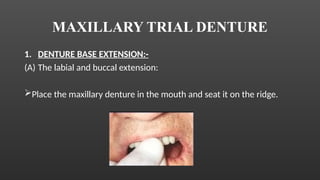
37. MAXILLARY TRIAL DENTURE
1. DENTURE BASE EXTENSION:-
(A) The labial and buccal extension:
Place the maxillary denture in the mouth and seat it on the ridge.
38. Light pressure on occlusal surface and move cheek in functional
movement – downward and inward
Check for over extension and under extension.
39. OVER EXTENSION:
Over extended flanges will stretch the sulcus tissue
Elastic recoil resulting in dislodgement of denture
Need adjustments till little or no movement occurs
Adequate clearance of frena (labial and buccal)
41. (B) Posterior extension:
Extension from one hamular notch to the other
Situated on the soft palate
If PPS is not done before, it can be done at this stage
42. 2. RETENTION:
It is noted that retention of trial denture is less than the processed
denture.
Looseness of upper trial denture makes it difficult to carry out
accurate assessment of occlusion.
Denture fixative can be used.
43. 3. STABILITY:
It is tested by applying pressure in a tissue ward direction with the ball of the index
finger in the premolar and molar regions on each side alternately.
This pressure must be directed at right angles to the occlusal surface where
displacement does occur.
Positive retention of finished denture *
CAUSES OF INSTABILITY
1. Warpage of denture base
2. Posterior teeth set buccal to the underlying alveolar ridge.
44. 4. ORIENTATION OF OCCLUSAL PLANE:
Proper orientation of occlusal plane is important for the following
reasons:
Patient aesthetics
Patient comfort
Chewing function
Balance of occlusion
45. NOTE :
Remove the upper denture from the mouth and immerse in cold water
for few seconds then place both dentures in the mouth.
46. BOTH DENTURES TOGETHER
Insert the lower denture first and then the upper denture.
Patient should be seated in an upright position
Patient head not supported by the head rest.
48. Verify first tooth contact in centric relation
(major issue)
ANTERIOR OPEN BITE POSTERIOR OPEN BITE
(BILATERAL)
POSTERIOR OPEN BITE
(UNILATERAL)
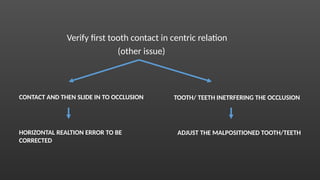
49. Verify first tooth contact in centric relation
(other issue)
CONTACT AND THEN SLIDE IN TO OCCLUSION TOOTH/ TEETH INETRFERING THE OCCLUSION
HORIZONTAL REALTION ERROR TO BE
CORRECTED
ADJUST THE MALPOSITIONED TOOTH/TEETH
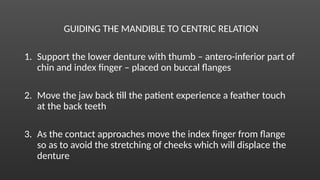
50. GUIDING THE MANDIBLE TO CENTRIC RELATION
1. Support the lower denture with thumb – antero-inferior part of
chin and index finger – placed on buccal flanges
2. Move the jaw back till the patient experience a feather touch
at the back teeth
3. As the contact approaches move the index finger from flange
so as to avoid the stretching of cheeks which will displace the
denture
51. Ask the patient to close slowly to achieve the first contact.
Repeat it 2-3 times till patient ensure light contact and we can see
the first contact
Close tightly and observe carefully for any shift
52. (A) VERIFICATION OF VERTICAL DIMENSION:
According to Winkler,
Patient is asked to count rapidly from 50-60
In a normal relationship, the lower lip should just touch the incisal
edges of the upper teeth.
The orthognathous or the prognathous jaw relation does not follow
this rule
53. When patient counts from one to ten, at the “six” and “seven”
sounds the maxillary and mandibular incisors are almost touching.
1. If at “six and seven,” the mandibular teeth are beyond maxilla –
maxillary teeth to be moved labially
2. If at “six and seven,” the mandibular teeth are too far lingual to
maxillary incisors – mandibular teeth are set too far to the lingual
3. If at “six and seven,” the incisors are too far – there may be too
much freeway space or interocclusal gap
54. According to Boucher,
The factors that govern the dentist’s final determination of this relation are:
1. Pre extraction records
2. Phonetics and esthetics
3. Amount of inter occlusal distance between the occlusal surfaces of the
teeth when mandible is at rest
4. Facial dimension and facial expression
5. Parallelism of the ridge
6. Amount of shrinkage of ridge
7. Inter arch distance
55. (B) VERIFICATION OF CENTRIC RELATION:
i. Intra oral observation of intercuspation of the teeth:
Guide the patient to centric relation.
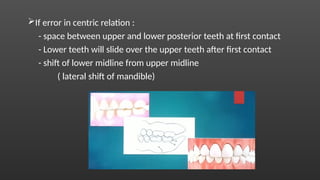
56. If error in centric relation :
- space between upper and lower posterior teeth at first contact
- Lower teeth will slide over the upper teeth after first contact
- shift of lower midline from upper midline
( lateral shift of mandible)
57. Interocclusal check record must be made to verify the relation
otherwise new centric relation should be made.
Keeping the vertical dimension same we have to repeat the
horizontal relation.
Mark the 2mm mark of overbite. *
58. ii. EXTRA ORAL ARTICULATOR METHOD
Purpose : to determine whether the position of teeth in the mouth is
same as that of the articulator
Aluwax bite registration material used
Waterbath of 135 F for 30seconds
63. (C) VERIFICATION OF ECCENTRIC RELATION
1. Focus is mainly – Protrusive records
Semi / Fully adjustable articulator
Gross error in horizontal jaw relation
64. Plaster interocclusal records are made
- anterior teeth arranged for esthetics – INCISAL GUIDANCE
(Adequate horizontal overlap needed – 6mm)
- ask the patient to bring mandible forward – edge to edge contact
65. Mount it to the articulator
Open up the centric lock
Check how the condyle is travelling on the path – check for accuracy.
66. 2. Lateral records
Displacement of ridge mucosa – difficult to make lateral records
Most semi adjustable articulator do not accept lateal eccentric
records
Hence, lateral interocclusal records for patients with complete
denture is not practical and are avoided
67. 2. EVENNESS OF OCCLUSAL PRESSURE:
Once the centric occlusion is checked and corrected, evenness of the
occlusion is checked next.
It frequently occurs that the teeth on one side occludes slightly before
the other ( molars before premolars)
This could be due to:
1. Pressure on the blocks heavier on one side than the other
2. Error in sealing models during articulation
3. warpage of base plates
68. To test the unevenness :
1. Place two pieces of celluloid strips between the teeth in the molar
region, one on each side
2. Ask the patient to close the mouth.
3. Try to pull out the strips with equal force
4. Any difference in the force required to remove the strips will readily
be appreciated.
69. Correction of unevenness of pressure :
1. Gently soften the wax supporting the teeth on the offending side
with a pin point flame.
2. Replace the dentures in the mouth and ask the patient to close the
mouth.
3. The teeth on the side of the heavy pressure will sink slightly until
the occlusion of the teeth on the opposite side arrests them.
70. 3. BALANCED OCCLUSION:
According to GPT-9,
“ the bilateral, simultaneous occlusal contact of the anterior and
posterior teeth in excursive movements”
71. With the teeth in lateral position of occlusion, insert the point of a
wax knife between the teeth on the balancing side
Try to separate them
If they separate, it means that the occlusion of teeth is due to
displacement of denture from the ridge
72. CAUSES:
1. Incorrect face-bow reading
2. Incorrect condylar path registration
If the error is slight – grind the occlusal surface of teeth
If the error is considerable – remount the models and reset the teeth.
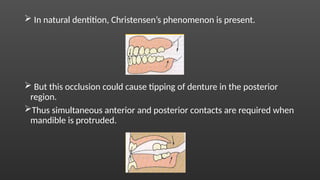
73. In natural dentition, Christensen’s phenomenon is present.
But this occlusion could cause tipping of denture in the posterior
region.
Thus simultaneous anterior and posterior contacts are required when
mandible is protruded.
74. 4. EVALUATION OF FACIAL AND FUNCTIONAL HARMONY WITH
ANTERIOR TEEH :
(A) MIDLINE:
Facial and dental midline must coincide
75. (B) ANTERIOR PLANE:
Incisal edges of the upper anterior must be set in harmony with the
lower lip
(C) LIP FORM:
76. Profile view of the patient
Check if the lip is adequately supported – not too protruded / not too
retruded
Well supported – the mucocutaneous border is up and wet line is
seen.
Contact should be between wet line to wet line and not
muco-cutaneous junction to muco-cutaneous junction
77. (D) PHONETCIS :
Sibilant ‘s’ :
- lip separate
- teeth separate
- air should flow through the space present to properly say ‘s’
78. Labiodental sound ‘f’ and ‘v’ :
- Tongue is in retruded position
- lower lip touches the upper teeth
Bilateral sound ‘p’ and ‘b’ :
- lips are in contact
- if patient cannot pronounce –
upper teeth protruded
79. (E) LIP LINE :
Refers to position of inferior border of upper lip during smile
formation and thereby determine the display of teeth and gingiva *
Ideally – gingiva margin and lip line should be congruent 1-2mm
3-4mm – gummy smile
80. (F) AMOUNT OF TOOTH VISIBILTY : Adequate visibility of the teeth
(G) CHARACTERIZATION : Can be done if it is reasonable and practical
(H) SHAPE, SIZE AND SHADE OF TEETH :
Harmony should exist with the facial type, gender and color of skin,
hair and eyes
81. 5. APPROVAL FROM PATIENT AND RELATIVES:
(A) PATIENT PREPARATION:
Patient needs time to relax and observe trial denture thoroughly.
82. Once the dentures are inserted in to the mouth, ask the patient to
stand in front of the mirror at a distance and observe.
After this make the patient sit on the chair and give a small mirror to
observe the denture more closely.
83. (B) OBSERVER PREPARATION:
They must be preconditioned for their responsibilities otherwise they
can sometimes do more harm than good.
Psychologically, if a person is asked to be the judge of a friend’s new
teeth, he/she will be over anxious to do the job.
By letting the observer know his/her limitation, much time is saved
and controversies are eliminated.
84. CONCLUSION
No stage in complete denture is anticipated with such mixed
emotions as in try in.
No stage is so significant to the future success or failure of the patient
to take dentures in his stride.
No stage has so much potential for making the person happy or
sinking him into the depths of despair.
85. REFERENCES
Boucher 9th
edition
Winkler 2nd
edition
Zarb – Bolender 12th
edition
H R B Fenn 2nd
edition
Removable partial denture framework try-in ,M.Ted Wong, DDS M.J. Calverley, DDS William
W. Nagy, DDS Show footnotes DOI:https://doi.org/10.1016/0022-3913(93)90181-M