





































































































































































































































































Unit 1; Gastro-Intestinal Disorders By Nursing Tutor-2.pptx
- 1. Gastrointestinal Disorders Unit-I Subject: AHN I Awal Sher Khan & Sohaib Ali Shah Faculty of Nursing Sciences Khyber Medical University 1
- 2. Learning Objectives By the end of the session learners will be able to: 1. Review the anatomy and physiology of gastrointestinal system (GIT) 2. Discuss the causes, pathophysiology and manifestation of the following GIT disorders 3. Discuss the diagnostic, medical and surgical management of the below mentioned disorders 4. Apply nursing process including assessment, planning, implementation and evaluation of care provided to the clients with GIT disorders 5. Develop a teaching plan for a client experiencing disorders of the GIT 2
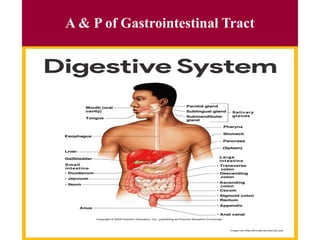
- 3. A & P of Gastrointestinal Tract 3
- 4. Disorders of mouth and esophagus • Stomatitis • Oral cancer/tumor • Salivary gland disorders • Gastro esophageal reflux disorder • Hiatal hernia • Achalasia • Diverticula • Esophageal cancer/tumor 4
- 5. Disorders of mouth and esophagus Stomatitis Inflammation of the mucous membrane of the mouth. It may be due to local lesion in the mouth, infection, nutritional deficiency, chemotherapy, immune suppression or a feature of a systemic disease. OR Stomatitis is inflammation of the mucosal tissue of the mouth (inner cheeks, tongue, lips, throat and gums etc.). 5
- 6. Sign and symptoms •swelling, •pain, •ulcerations, • excessive salivation, •halitosis, (bad breath) •sore mouth •In ability to chewing •bleeding •Bad smell 6
- 7. Causes of stomatitis •Infection: • Viruses: measles, primary herpes simplex. • Bacteria: streptococcus, diphtheria. • Fungus: Candida albicans . •Eruption stomatitis: associated with eruption of teeth. •Traumatic: cheek biters. •Local reactions: due to sensitivity to contact substances from foods. •Immunological impairment: in leukemias. •Drugs and poisons •Chemotherapy •Radiation therapy 7
- 8. Investigations •Oral swab culture •Physical examination • Learning Objectives 8
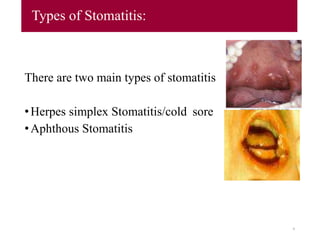
- 9. Types of Stomatitis: There are two main types of stomatitis •Herpes simplex Stomatitis/cold sore •Aphthous Stomatitis 9
- 10. Cont…. •Herpes simplex Stomatitis • Herpes simplex Stomatitis (cold sore/fever blister): • It is an externally common viral infection that produces characteristic blisters commonly called cold sore or fever blister. • It is caused by herpes simplex virus type I (HSV-1) predisposing factors of upper respiratory infections, excessive exposure to sunlight, food allergies, emotional stress and onset of menstruation. • The virus is harbored in a dormant (inactive) state by cells in the sensory nerve ganglia. • Reactivation of the virus can occur with emotional stress, fever, exposure to cold or ultraviolet rays. 10
- 11. 11 Cold Sore
- 12. Cont… • The lesions appear more common on the mucous membranous border junction of the lips in the form of small vesicles, which then erupt and form painful shallow ulcers. • Vesicle formation may be single or clustered. • Painful vesicles and ulceration of mouth, lips or edge of nose; may have prodromal itching or burning, fever, malaise, lymphadenopathy may occur. • Prodromal: relating to or denoting the period between the appearance of initial symptoms and the full development of a rash or fever. • Lymphadenopathy: A disease affecting the lymph nodes 12
- 13. /Pathophysiology of HSS • Etiology: HSV I (less commonly HSV II) Transmission: • via mucous membranes or open skin • Kissing • Fomites (e.g. shared towels, utensils) • Incubation: 2-20 days after contact. • Shedding: 48-60 hour duration (not longer than 96 hours) 13
- 14. Aphthous Stomatitis • Aphthous Stomatitis (cancer sore) it is recurrent and chronic form of infection secondary to systemic disease, trauma, stress or unknown causes. The cause remains unknown, an autoimmune base is suspected. Self-limited, they usually resolve within a few weeks, but they may recur in the same or a different location. • It produces well-circumscribed ulcers on the soft tissues of the mouth, including lips, tongue, insides of the cheeks, pharynx and soft palate. • Ulcers of the mouth and lips causing extreme pain, ulcers surrounded by erythematous base. • Painful small ulceration on oral mucosa heals in 1 to 3 weeks. 14
- 15. Risk Factors •Aging •Nutritional deficiency •Poor oral hygiene •Smoking •Alcohol •Specific chemotherapeutic agents •Bone marrow transplantation •Radiotherapy 15
- 16. 16
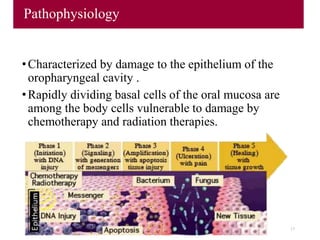
- 17. Pathophysiology •Characterized by damage to the epithelium of the oropharyngeal cavity . •Rapidly dividing basal cells of the oral mucosa are among the body cells vulnerable to damage by chemotherapy and radiation therapies. 17
- 18. Treatment •pain relief, • removal of causative factor, •oral hygiene with saline, Gentian violet, glycerin •Broad spectrum antibiotic in sever case •Anti fungal drugs i.e. Nystatin, Daktarin • soft bland diet •IV infusion in sever case 18
- 19. Nursing diagnosis •Pain related to lesion of mouth. •Alteration in nutrition less than body requirement related to ulceration in the mouth and chewing problem. •Alter sleep pattern related to pain secondary to stomatitis. •Difficulty in talking (dysphasia) related to blisters and sores on the tongue. 19
- 20. Nursing Intervention • Check for oral burning, pain, or change in tolerance to temperature. • Do oral examination noting evidence of lesions within the mouth and tongue. • Administer the respective medication. • Give analgesic to relieve from pain. • Advice soft food and avoid spicy food. • Do oral hygiene with soothing solution. • Administer topical medication e.g. nylstate and bonjela to relieve from pain to enhance sleep. 20
- 21. Oral cancer Oral cancer is a subtype of head and neck cancer, is any cancerous tissue growth located in the oral cavity. 21
- 22. Signs and symptoms •lesion, lump, or ulcer that do not resolve in 14 days located: •On the tongue, lip, or other mouth areas •Usually small •Most often pale colored, be dark or discolored •Early sign may be a white patch (leukoplakia) or a red patch (erythroplakia) on the soft tissues of the mouth •Usually painless initially •May develop a burning sensation or pain when the tumor is advanced 22
- 23. Cont… •Additional symptoms that may be associated with this disease: •Tongue problems •Swallowing difficulty •Mouth sores •Pain and paresthesia are late symptoms. •Feeling of something caught in the throat •Difficulty or pain with chewing or swallowing •Swelling in jaw •Voice changes •Pain in ear 23
- 24. Oral Cancer •Occurs most often in people over age 40 Symptoms •Sore that does not heal •Lump on lip or mouth •White or red patch on gum, tongue, or buccal mucosa •Unusual bleeding, numbness, or pain 24
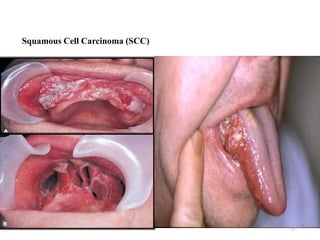
- 25. 25 Squamous Cell Carcinoma (SCC)
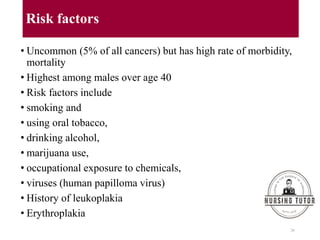
- 26. Risk factors • Uncommon (5% of all cancers) but has high rate of morbidity, mortality • Highest among males over age 40 • Risk factors include • smoking and • using oral tobacco, • drinking alcohol, • marijuana use, • occupational exposure to chemicals, • viruses (human papilloma virus) • History of leukoplakia • Erythroplakia 26
- 27. Pathophysiology a. Squamous cell carcinomas b. Begin as painless oral ulceration or lesion with irregular, ill- defined borders c. Lesions start in mucosa and may advance to involve tongue, oropharynx, mandible, maxilla d. Non-healing lesions should be evaluated for malignancy after one week of treatment 27
- 28. Investigation a. Elimination of causative agents b. Determination of malignancy with biopsy c. Determine staging with CT scans and MRI 28
- 29. Treatment 1. Surgery and/or 2. Radiation • Treatment usually involves surgery or radiation or both • Chemotherapy primarily used as an adjunctive procedure in advanced cases • Advanced lesions < 30% 5-year survival rate • 9 - 25% of patients develop additional mouth or throat cancer 3. Chemotherapy • Several drugs currently being used include: • Paclitaxel (Taxol, Bristol) • Methotrexate • Bleomycin • Cisplatin • 5-Fluorouracil 29
- 30. Nursing Diagnosis • Pain related to oral lesion or treatment • Imbalanced nutrition less than body requirements, related to inability to ingest adequate nutrients secondary to oral condition. • Risk for infection related to disease or treatment • Alter sleep pattern related to pain secondary to stomatitis. • Impaired verbal communication related to treatment 30
- 31. Nursing Intervention •Pain management •Oral hygiene •Preparation for surgery or radiation •Nutritional management •Post operative care and dressing •Symptomatic treatment. •Administration of chemotherapy •Monitoring of client response to any treatment •Emotional support to client and family •Care of symptom associated with treatment 31
- 32. Cont…. Health promotion: Teach risk of oral cancer associated with all tobacco use and excessive alcohol use Need to seek medical attention for all non-healing oral lesions (may be discovered by dentists); early precancerous oral lesions are very treatable Work out for following possible Nursing Diagnoses 1. Risk for ineffective airway clearance 2. Imbalanced Nutrition: Less than body requirements 3. Impaired Verbal Communication: establishment of specific communication plan and method should be done prior to any surgery 4. Disturbed Body Image 32
- 33. Salivary Glands disorder • The salivary glands make saliva and release it into the mouth. There are three pairs of relatively large, major salivary glands: • Parotid glands: Located in the upper part of each cheek, close to the ear. The duct of each parotid gland empties onto the inside of the cheek, near the molars of the upper jaw. • Submandibular glands: Under the jaw. They have ducts that empty behind the lower front teeth. • Sublingual glands: Beneath the tongue. They have ducts that empty onto the floor of the mouth. oIn addition to these major glands other minor salivary glands are scattered throughout the mouth and throat. 33
- 34. Cont…. 34
- 35. Classification of Salivary Glands disorder 1-Obstructions: this could be by calculi or cystic type (stone, mucocele, ranula) 2-Infections: viral (Mumps), bacterial (acute & chronic Sialadenitis) 3-Degenerative changes: Sjogren syndrome, radiation. 4-Functional disorders. 5- Neoplasms. 35
- 36. Investigations for salivary glands 1- Sialometery: measures the amount of saliva production in a certain time. 2- Sialochemistry: measures the composition of saliva. 3- Sialography: by introducing the iodine containing contrast media through the opening of the duct. 4- Sonography: Ultrasonic patterns when dealing with minor salivary glands. 5- Cytology: by aspiration. 6- Biopsy. 36
- 37. Cont…. Some of the most common salivary gland disorders include: Sialolithiasis Sialadenitis Viral infections Cysts Benign tumors Malignant tumors Sjogren's syndrome Sialadenosis 37
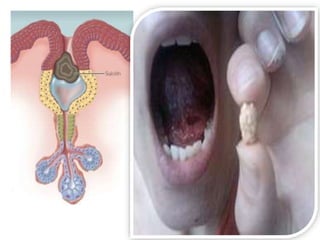
- 38. Sialolithiasis Sialolithiasis (salivary gland stones) Tiny, calcium-rich stones sometimes form inside the salivary glands. 70-90% of stones occur in the submandibular gland due to long twisted path of the duct & thick secretion of the gland. about 6% in parotid gland & 2% in sublingual gland & minor S.G. • Etiology: The exact cause of these stones is unknown. Some stones may be related to: • Dehydration, which thickens the saliva. • Decreased food intake, which lowers the demand for saliva. • Medications that decrease saliva production, including certain antihistamines, anti-hypertensive drugs and psychiatric medications. • Deposition of ca++ salt around a nidus of debris within the duct lumen 38
- 39. Cont…. • Some stones sit inside the gland without causing any symptoms. In other cases, a stone blocks the gland's duct, either partially or completely. When this happens, the gland typically is painful and swollen, and saliva flow is partially or completely blocked. This can be followed by an infection called sialadenitis. • Signs & Symptoms The most common symptom are dry mouth and a painful lump, usually in the floor of the mouth. Pain may worsen during eating. • Treatments • Gentle probing: If the stone is located near the end of the duct, the doctor may be able to press it out gently. • Therapeutic sialdenoscopy • Surgery: If stone are in deeper part • Shock wave treatment 39
- 40. 40
- 41. Sialadenitis Sialadenitis: (infection of a salivary gland) Sialadenitis is a painful infection. It is more common among elderly adults with salivary gland stones. Sialadenitis also can occur in infants during the first few weeks of life. •Etiology It is usually caused by bacteria. •Sign and symptoms: Symptoms may include: oA tender, painful lump in the cheek or under the chin. oIn severe cases, fever, chills and general weakness. 41
- 42. Cont…. Treatment Treatment includes: •Drinking fluids or receiving fluids intravenously •Antibiotics •Warm compresses on the infected gland •Encouraging saliva flow by chewing gums, sugarless candies or by drinking orange juice. •If these methods do not cure the infection, surgery can be done to drain the gland. 42
- 43. Viral infections Viral infections: Systemic (whole-body) viral infections sometimes settle in the salivary glands. This causes facial swelling, pain and difficulty in eating. The most common example is mumps. •Etiology These infections are caused by viruses. • Sign and symptoms The first symptoms often include: •Fever and poor appetite •Headache, •Muscle aches •Joint pain and malaise. 43
- 44. Cont…. •Treatment: These infections almost always go away on their own. Treatment focuses on relieving symptoms through: •Rest •Drinking fluids to prevent dehydration •Taking acetaminophen (Tylenol) to relieve pain and fever 44
- 45. Cysts Cysts: (tiny fluid-filled sacs) Babies sometimes are born with cysts in the parotid gland because of problems related to ear development before birth. Later in life, other types of cysts can form in the major or minor salivary glands. • Etiology They may result from traumatic injuries, infections, or salivary gland stones or tumors. • Sign and symptoms: A cyst causes a painless lump. It sometimes grows large enough to interfere with eating. • Treatment : A small cyst may drain on its own without treatment. Larger cysts can be removed using traditional surgery or laser surgery. 45
- 46. Benign tumors Benign tumors: (noncancerous tumors) Most salivary gland tumors occur in the parotid gland. The majority are benign. The most common type of benign parotid tumor usually appears as a slow-growing, painless lump at the back of the jaw, just below the earlobe. • Etiology Risk factors include radiation exposure and possibly smoking. • Sign and symptoms A slow-growing lump is the most common symptom. The lump is sometimes painful. This lump may be found in the cheek, under the chin, on the tongue or on the roof of the mouth. • Treatment Non cancerous tumors usually are removed surgically. In some cases, radiation treatments are given after surgery to prevent the tumor from returning. 46
- 47. Malignant tumors • Malignant tumors: (cancerous tumors) Salivary gland cancers are rare. They can be more or less aggressive. • Etiology The only known risk factors for salivary gland cancers are Sjogren's syndrome and exposure to radiation. Smoking also may play some role. • Sign and symptoms A slow-growing lump is the most common symptom. The lump is sometimes painful. This lump may be found in the cheek, under the chin, on the tongue or on the roof of the mouth. • Treatment Smaller, early stage, low-grade tumors often can be treated with surgery alone. However, larger, high-grade tumors usually require radiation following surgery. Tumors that cannot be operated are treated with radiation or chemotherapy. 47
- 48. Sjogren's syndrome • Sjogren's syndrome Sjogren's syndrome is a chronic autoimmune disorder. The body's immune defenses attack the salivary glands, the lacrimal glands (glands that produce tears), and occasionally the skin's sweat and oil glands. • Classification: Primary: xerostomia + xerophthalmia Secondary: xerostomia + xerophthalmia + C.T. disease usually rheumatoid arthritis. • Etiology Over activity of the immune system. • Sign and symptoms The main features of Sjogren's syndrome are swelling of the salivary glands, dry eyes and a dry mouth. • Immune system attacks parts of your own body by mistake. In Sjogren's syndrome, it attacks the glands that make tears and saliva. This causes a dry mouth and dry eyes. 48
- 49. Cont…. Treatment •The main symptom related to the salivary glands is a dry mouth. Options include: •Medication to stimulate more saliva secretion, such as pilocarpine (Salagen) and cevimeline (Evoxac). •Sugarless gum and candy to stimulate saliva production. •Avoiding medications that can make dry mouth worse. •Avoid smoking. •Good oral hygiene is must. People with Sjogren's have teeth and gum problems because of low saliva secretion. 49
- 50. Sialadenosis Sialadenosis (nonspecific salivary gland enlargement) Sometimes, the salivary glands become enlarged without evidence of infection, inflammation or tumor. This nonspecific enlargement is called sialadenosis. It most often affects the parotid gland. • Etiology Its cause remains unknown. • Sign and symptoms This condition typically causes painless swelling of the parotid glands on both sides of the face. • Treatment: Treatment is aimed at correcting any underlying medical problem. Once the medical problem improves, the salivary glands should shrink to normal size. 50
- 51. Medical Diagnosis • Medical history. • Smoking history. • Current medications. • Blood tests. • X-rays. • Magnetic resonance imaging (MRI). • Computed tomography (CT) scans. • Sialography. • Salivary gland biopsy. • Salivary function test. 51
- 52. Complications • Abscess of salivary gland. • Infection returns. • Spread of infection. • Facial nerve injury (Sialorrhea). • Hematoma. • Deformity. • Dry mouth (xerostomia). • Mumps. 52
- 53. Prevention • We can lower our risk of viral infections of the salivary glands. To do so, get immunized against mumps and influenza. • There are no specific guidelines to protect against other types of salivary gland disorders. However, it is helpful to: • Avoid smoking. • Eat a healthy diet. • Drink six to eight glasses of water daily to avoid dehydration. • Practice good oral hygiene, with regular tooth brushing and flossing. 53
- 54. Nursing Diagnosis • Low secretion of saliva related to stone in the salivary gland. • Dry mouth related to blockage of saliva. • Pain related to tumor & inflammation in the mouth. • Difficulty in eating related to painful lump in the mouth. • Poor appetite related to disease. • Fever related to infection of salivary gland. 54
- 55. Nursing Interventions • Give medication to stimulate more saliva secretion, such as pilocarpine (Salagen) and cevimeline (Evoxac). • Give sugarless gum and candy to stimulate saliva production. • Avoiding medications that can make dry mouth worse. • Provide analgesic to relief pain. • Administer tube feeding. • Give acetaminophen (Tylenol) to relieve fever. • Cold sponging to relieve from fever. 55
- 56. Gastroesophageal Reflux Disease (GERD) • Gastroesophageal reflux is the backward flow of gastric content into the esophagus. • People with asthma are at higher risk of developing GERD. Asthma flare-ups can cause the lower esophageal sphincter to relax, allowing stomach contents to flow back, or reflux, into the esophagus. • GERD common, affecting 15 – 20% of adults • 10% persons experience daily heartburn and indigestion 56
- 57. Pathophysiology • When you eat, food passes from the throat to the stomach through the esophagus. A ring of muscle fibers in the lower esophagus prevents swallowed food from moving back up. These muscle fibers are called the lower esophageal sphincter (LES). • When this ring of muscle does not close all the way, stomach contents can leak back into the esophagus. This is called reflux or gastroesophageal reflux. Reflux may cause symptoms. Harsh stomach acids can also damage the lining of the esophagus. • Gastroesophageal reflux results from transient relaxation or incompetence of lower esophageal sphincter, or increased pressure within stomach 57
- 58. Factors contributing to gastroesophageal reflux • Increased gastric volume (post meals) • Position pushing gastric contents close to gastroesophageal juncture (such as bending or lying down) • Increased gastric pressure (obesity or tight clothing) • Hiatal hernia 58
- 59. Cont.. • Normally the peristalsis in esophagus and bicarbonate in salivary secretions neutralize any gastric juices (acidic) that contact the esophagus; during sleep and with gastroesophageal reflux esophageal mucosa is damaged and inflamed; prolonged exposure causes ulceration, friable mucosa, and bleeding; untreated there is scarring and stricture. Manifestations • Heartburn after meals, while bending over, or recumbent and worse at night • May have regurgitation of sour materials in mouth, pain with swallowing • Chest pain • Nausea • Bloating, gas and belching • Sensation of lump in throat 59
- 60. 60
- 61. Cont.. Complications • Esophageal strictures, which can progress to dysphagia • Barrett’s esophagus: changes in cells lining esophagus with increased risk for esophageal cancer diagnosis • Esophagitis Diagnostic tests • Barium swallow (evaluation of esophagus, stomach, small intestine) • Upper GI endoscopy: direct visualization; biopsies may be done • 24-hour ambulatory pH monitoring (gold standard of GERD) • Esophageal motility studies/ Esophageal manometry, which measure pressures of esophageal sphincter and peristalsis 61
- 62. Cont.. Treatment • Life style changes • Diet modifications • Medications 62
- 63. Cont.. Medications • Antacids: for mild to moderate symptoms, e.g. Mucain, Tricel, Mylanta, Gaviscon • H2-receptor blockers: decrease acid production; given BID or more often, e.g. cimetidine, ranitidine, famotidine, nizatidine • Proton-pump inhibitors: reduce gastric secretions, promote healing of esophageal erosion and relieve symptoms, e.g. omeprazole (risek); lansoprazole (Prevacid) initially for 8 weeks; or 3 to 6 months • Promotility agent: enhances esophageal clearance and gastric emptying, e.g. metoclopramide (reglan) 63
- 64. Cont.. Surgery • Surgery indicated for persons not improved by diet and life style changes • Laparoscopic procedures to tighten lower esophageal sphincter • Open surgical procedure: Nissen fundoplication 64
- 65. Cont.. Dietary and Lifestyle Management • Elimination of acid foods (tomatoes, spicy, citrus foods, coffee) • Avoiding food which relax esophageal sphincter or delay gastric emptying (fatty foods, chocolate, peppermint, alcohol) • Maintain ideal body weight • Eat small meals and stay upright 2 hours post eating; no eating 3 hours prior to going to bed • Elevate head of the bed 6 – 8 inches to decrease reflux • No smoking • Avoiding bending and wear loose fitting clothing • Limit meal size and avoid heavy evening meal 65
- 66. Nursing Diagnosis • Imbalanced nutrition: less than body requirements related to inability to intake enough food because of reflux. • Acute pain related to irritated esophageal mucosa. • Imbalanced nutrition: more than body requirements related to eating to try to assuage pain. • Impaired tissue integrity related to esophageal exposure to gastric acid. • Nausea related to irritation of gastric mucosa secondary to Gastroesophageal Reflux Disease (GERD) 66
- 67. Nursing Management • Avoid factors that cause reflux • Stop smoking • Avoid acid or acid producing foods • Elevate HOB ~30° • Do not lie down 2 to 3 hours after eating • Patient teaching • Drug therapy • Evaluate effectiveness • Observe for side effects 67
- 68. Hiatal Hernia • Hiatal hernia also known as diaphragmatic hernia a condition in which a portion of the stomach or the lower part of the esophagus protrudes upward into the thoracic cavity through a defect in the wall of the diaphragm. 68
- 69. Cont.. Causes: • Loss of muscle strength and tone • Factors that cause increased intra-abdominal pressure (such as obesity or multiple pregnancies) • Congenital defects • Trauma 69
- 70. Cont.. Manifestations • Often no signs and symptoms unless there is reflux of stomach acid • Indigestion, belching, • substernal or epigastric pain • feelings of pressure after eating • Regurgitation of a hot, sour liquid coming into the throat or mouth • Nighttime coughing that may awaken the patient 70
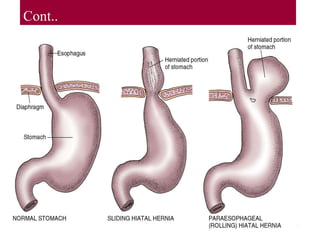
- 71. Cont.. Pathophysiology: • A defect in the wall of the diaphragm where the esophagus passes through Protrusion of part of the stomach or the lower part of the esophagus up into the thoracic cavity • Herniated portion often slides back beneath the diaphragm 71
- 72. Cont.. 72
- 73. Cont.. Diagnostic procedure: • History & P.E • UGI series or barium swallow • X-ray, CT or MRI • Endoscopy 73
- 74. Cont.. Medical management: • Weight reduction • Avoidance of tight-fitting clothes around the abdomen • Administration of antacids, H2-receptor antagonists, or proton pump inhibitors • Elevating the head of the bed 6 to 8 inches • Instructing the patient not to eat within 3 hours of going to bed • Limiting intake of alcohol, chocolate, caffeine, and fatty food, and avoiding smoking • Surgical correction of the hernia if bleeding or discomfort cannot be controlled. • Anchoring the lower esophageal sphincter by wrapping a portion of the stomach around it to anchor it in place 74
- 75. 75
- 76. Cont.. Nursing management: • Encouraging weight reduction if necessary • Reminding the patient to stay upright for 2 hours after eating and not to eat 3 hours before bedtime • Advising against lifting or moving heavy items • Using a wedge pillow to elevate the upper body if the head of the bed cannot be raised • Encouraging the patient to take prescribed H2-receptor antagonists or proton pump inhibitors at bedtime to prevent reflux and damage from acid entering the esophagus • Advising the patient to avoid foods that cause bloating, which increases abdominal pressure and may push the stomach upward through the diaphragmatic defect. 76
- 77. Cont.. Nursing Diagnosis for Hiatal Hernia • Risk for aspiration related to reflux of gastric contents and impaired esophageal sphincter function. • Acute pain related to esophageal inflammation and irritation caused by reflux of gastric contents. • Imbalanced nutrition: less than body requirements related to decreased oral intake and fear of eating due to pain and discomfort. • Anxiety related to symptoms and potential complications of GERD and hiatal hernia. • Risk for ineffective coping related to chronic illness and lifestyle changes required for disease management. 77
- 78. Cont.. Nursing Diagnosis for Hiatal Hernia • Ineffective self-health management related to lack of knowledge about disease process and treatment options. • Risk for impaired gas exchange related to decreased lung expansion due to upward displacement of the diaphragm in hiatal hernia. • Risk for injury related to potential complications of hiatal hernia such as bleeding or obstruction. • Disturbed sleep pattern related to nighttime symptoms of GERD and hiatal hernia. • Impaired swallowing related to esophageal inflammation and obstruction caused by hiatal hernia. 78
- 79. Achalasia • Achalasia is absent or ineffective peristalsis of the distal esophagus, accompanied by failure of the esophageal sphincter to relax in response to swallowing. Narrowing of the esophagus just above the stomach results in a gradually increasing dilation of the esophagus in the upper chest. 79
- 80. Cont.. Causes: • Idiopathic (unknown cause) in most cases • degeneration of the nerves in the esophagus • Dysfunction of (LES) • Inflammation of the esophageal muscles • Viral infections • Autoimmune disorders • Hereditary factors • Environmental factors such as exposure to chemicals or radiation 80
- 81. Cont.. Clinical Manifestations: • difficulty in swallowing both liquids and solids • sensation of food sticking in the lower portion of the esophagus • regurgitation, either spontaneously or intentionally • chest pain and heartburn (pyrosis). 81
- 82. Cont.. Diagnostic procedure: • X-ray studies • Barium swallow • computed tomography (CT) • endoscopy may be used for diagnosis; • however, the diagnosis is confirmed by manometry, a process in which the esophageal pressure is measured by a radiologist or gastroenterologist. 82
- 83. Cont.. Medical and Surgical management: • The patient should be instructed to eat slowly and to drink fluids with meals. • As a temporary measure, calcium channel blockers and nitrates have been used to decrease esophageal pressure and improve swallowing. • Injection of botulinum toxin (Botox) to quadrants of the esophagus via endoscopy has been helpful because it inhibits the contraction of smooth muscle. Periodic injections are required to maintain remission. • If these methods are unsuccessful, pneumatic (forceful) dilation or surgical separation of the muscle fibers may be recommended (Heller myotomy) 83
- 84. Cont.. Nursing Diagnosis: • Impaired Swallowing related to esophageal dysfunction and dysphagia manifested by difficulty swallowing solid and liquid foods, regurgitation, and chest pain. • Risk for Aspiration related to decreased lower esophageal sphincter (LES) function and difficulty swallowing manifested by coughing, choking, and respiratory distress. • Imbalanced Nutrition: Less than Body Requirements related to inadequate oral intake due to difficulty swallowing manifested by weight loss, poor oral intake, and malnutrition. • Anxiety related to fear of choking or complications related to the disease process manifested by restlessness, nervousness, and apprehension. 84
- 85. Cont.. Nursing Diagnosis: • Ineffective Coping related to chronic illness and its impact on daily activities manifested by poor self-care, social isolation, and decreased quality of life. • Risk for Injury related to fatigue, weakness, or impaired mobility manifested by falls, accidents, and decreased ability to perform activities of daily living. 85
- 86. Cont.. Nursing Intervention: • Nutrition management: ensure adequate nutrition and hydration, such as providing small, frequent meals and thickening liquids if needed. • Medication administration: Nurses may administer medications that help relax the LES. • Positioning: Positioning the patient in an upright position during and after meals can help reduce the risk of aspiration and improve digestion. • Patient education: about the disease process, the importance of adhering to treatment plans, and warning signs of complications such as weight loss or recurrent chest pain. 86
- 87. Cont.. Nursing Intervention: • Emotional support: Patients with achalasia may experience anxiety or depression due to their symptoms or difficulty swallowing. Nurses can provide emotional support, assess for any psychosocial issues, and refer the patient to appropriate resources such as counseling or support groups. • Monitoring for complications: Nurses should monitor for complications such as aspiration pneumonia, weight loss, or chest pain, and report any changes in the patient's condition to the healthcare team. 87
- 88. Diverticulum • Diverticulum is an outpouching of mucosa and submucosa through a weak portion of the musculature in the esophagus. • Zenker's diverticulum is the most common type, occurring in the upper area of the esophagus in people over 60. • Other types include midesophageal, epiphrenic, and intramural diverticula. 88
- 89. Cont.. Causes: • Improper functioning of the lower esophageal sphincter or motor disorders of the esophagus. • Age-related changes in the esophagus. 89
- 90. Cont.. Clinical Manifestations: • Difficulty swallowing, fullness in the neck, belching, regurgitation of undigested food, and gurgling noises after eating. • Undigested food regurgitation when in a recumbent position. • Halitosis and sour taste in the mouth. 90
- 91. Cont.. Diagnostic procedure: • Barium swallow to determine the exact nature and location of a diverticulum. • Manometric studies to rule out a motor disorder. • Esophagoscopy is usually contraindicated due to the danger of perforation of the diverticulum. 91
- 92. Cont.. Medical Management: • Management of symptoms such as dysphagia and chest pain. • Intramural diverticula usually regress after the esophageal stricture is dilated. Surgical Management: • Surgery is indicated if symptoms are troublesome and becoming worse. 92
- 93. Cont.. Nursing Diagnosis: • Impaired Swallowing related to pharyngoesophageal pulsion diverticulum as evidenced by difficulty swallowing, regurgitation of undigested food, and gurgling noises after eating. • Imbalanced Nutrition: Less Than Body Requirements related to pharyngoesophageal pulsion diverticulum as evidenced by weight loss, anorexia, and inadequate dietary intake. • Risk for Aspiration related to pharyngoesophageal pulsion diverticulum as evidenced by difficulty swallowing, regurgitation of undigested food, and coughing. • Anxiety related to surgical intervention for diverticulum as evidenced by verbalization of fears, restlessness, and increased heart rate. • Risk for Infection related to surgical intervention for diverticulum as evidenced by surgical wound site drainage, fever, and elevated white blood cell count. 93
- 94. Cont.. Nursing Management: • Diet: Patients with diverticulum should be advised to consume a high-fiber diet to prevent constipation and reduce the pressure on the diverticulum. Additionally, patients may need to avoid certain foods that can irritate the diverticulum, such as seeds, nuts, and popcorn. • Medications: Patients may need to take medications to manage symptoms such as pain, reflux, and constipation. Nurses should ensure that patients understand the correct dosage and potential side effects of these medications. 94
- 95. Cont.. Nursing Management: • Post-operative care: For patients who undergo surgery to remove a diverticulum, nurses should closely monitor the surgical incision for signs of infection or leakage. Patients may also require a nasogastric tube and may need assistance with maintaining proper nutrition and hydration during the post-operative period. • Education: Nurses should educate patients on the importance of following a high-fiber diet, staying well hydrated, and avoiding activities that can increase intra- abdominal pressure (such as heavy lifting or straining during bowel movements). Patients should also be advised to seek medical attention if they experience worsening symptoms or develop complications such as fever or severe abdominal pain. 95
- 96. Esophageal cancer/tumor • Cancer of the esophagus, also known as esophageal cancer, is a malignant tumor that develops in the tissues of the esophagus. • Esophageal cancer typically arises from the inner lining of the esophagus and can spread to nearby tissues and organs if not diagnosed and treated at an early stage. • There are two main types of esophageal cancer: Adenocarcinoma: Begins in glandular cells that lines the esophagus which produce and release mucus. It usually form in the lower part of esophagus near stomach and often caused by Barrett’s esophagus. Squamous cell carcinoma: Found in upper and middle section of esophagus and risk factor is smoking and alcohol ingestion. 96
- 97. 97
- 98. Cont.. Causes • Smoking. • Heavy alcohol consumption. • Chronic heartburn or acid reflux. • Gastroesophageal reflux disease (GERD) • Barrett's esophagus, a condition that sometimes develops in people with GERD. • Achalasia, a rare disorder of muscles in the lower esophagus. 98
- 99. Cont.. Manifestations • Progressive dysphagia (difficulty swallowing) • Hoarseness • Regurgitation of foods • Foul breath • Persistent cough • Dysphagia initially with solids, then with soft foods, and eventually even with liquids • Late occurrence of pain (substernal, epigastric, or back) with swallowing • Weight loss 99
- 100. Cont.. Diagnostic Procedures • Barium swallow with fluoroscopy may reveal a narrowed esophagus. • Definitive diagnosis is made through esophagogastroduodenoscopy (EGD) • Biopsy • Biomarker testing • Cytosponge is a new diagnostic test being introduced by NHS Scotland to identify important oesophageal conditions such as Barrett's oesophagus 100
- 101. Cont.. Medical Management: 1. Endoscopic ablative therapy (photodynamic therapy, radiotherapy ablation, endoscopic mucosal resection) 2. Radiofrequency ablation burns away abnormal cells using radiofrequency energy. 3. Photodynamic therapy uses medication to make damaged cells sensitive to light, which is then used to destroy them. 4. Endoscopic mucosal resection involves injecting a saline solution under the lining of abnormal tissue to facilitate its removal. 5. Palliative care for advanced stage cancer may include external beam radiation, chemotherapy, esophageal dilation, electrocoagulation, photodynamic therapy, and the insertion of expanding metal stents to relieve severe dysphagia. 101
- 102. Cont.. Surgical Management: • Esophagectomy (removal of sections of the esophagus) with reconstruction using part of the stomach is occasionally performed but carries multiple potential complications. 102
- 103. Cont.. Nursing Diagnosis: • Risk for Infection related to impaired swallowing and compromised immune system as evidenced by presence of fever, increased white blood cell count, signs of respiratory infection (e.g., cough, chest congestion). • Deficient Knowledge about the disease process, treatment options, and self-care measures as evidenced by patient or family member’s express confusion or lack of understanding about the disease, treatment options, or self-care instructions. • Disturbed Body Image related to changes in physical appearance and functional abilities as evidenced by expressions of dissatisfaction or discomfort with changes in body image, social withdrawal, low selfesteem. • Risk for Aspiration related to impaired swallowing and reflux as evidenced by coughing, choking, history of aspiration pneumonia, dyspnea. 103
- 104. Cont.. Nursing Diagnosis: • Impaired Swallowing related to tumor obstruction and/or radiation therapy as evidenced by difficulty swallowing (dysphagia), coughing or choking during eating or drinking, regurgitation, weight loss. • Imbalanced Nutrition: Less Than Body Requirements related to dysphagia and treatment-related side effects as evidenced by weight loss, decreased oral intake, malnutrition, fatigue, altered taste sensation. • Anxiety related to diagnosis, treatment, and prognosis as evidenced by restlessness, increased heart rate, nervousness, difficulty sleeping, verbal expressions of worry or fear. • Acute Pain related to esophageal inflammation, tumor invasion, or surgical interventions as evidenced by sharp or burning pain in the chest or upper abdomen, pain with swallowing or eating, pain at the surgical site. 104
- 105. Cont.. Nursing Interventions: • The intervention focuses on improving the patient's nutritional and physical condition before surgery, radiation therapy, or chemotherapy. • A high-calorie and high-protein diet, in liquid or soft form, is provided to promote weight gain if the patient can consume adequate food orally. • If oral intake is not possible, parenteral (intravenous) or enteral (tube feeding) nutrition is initiated. • The patient's nutritional status is monitored throughout the treatment process. • The patient is informed about the postoperative equipment that will be used, such as closed chest drainage, nasogastric suction, parenteral fluid therapy, and gastric intubation. 105
- 106. Cont.. Nursing Interventions: • After recovering from anesthesia, the patient is placed in a low Fowler's position and later in a Fowler's position to prevent reflux of gastric secretions. • Close observation is maintained for regurgitation, dyspnea, and the possibility of aspiration pneumonia. • The patient's temperature is monitored to detect any elevation that may indicate aspiration or fluid seepage into the mediastinum. • If jejunal grafting has been performed, the nurse checks the graft viability hourly for at least the first 12 hours. 106
- 108. Objectives: • At the end of this lecture the students will be able to: • Define Gastritis and types of Gastritis. • Elaborate etiology of Gastritis • Explain Pathophysiology of Gastritis • Sign and symptoms of Gastritis. • Discuss diagnosis , and medical management of Gastritis • Apply Nursing Process to the patients suffering from Gastitis
- 109. Gastritis: • Definition; • Gastritis is an inflammation, irritation or erosion of the stomach mucosa. • Gastritis is a condition that inflames stomach lining (the mucosa), causing belly pain, indigestion (dyspepsia), bloating and nausea. • Gastritis can come on suddenly (acute) or gradually (chronic).
- 110. Cont'd • Gastritis is a general term for a group of conditions with one thing in common: inflammation of the lining of the stomach • In some cases, gastritis can lead to ulcers and an increased risk of stomach cancer. • Pangastritis; Inflammation of the whole stomach is called Pangastritis • Antral gastritis ;Inflammation of a part of stomach.
- 114. Types of Gastritis • Gastritis can broadly be divided into acute gastritis and chronic gastritis. • Acute gastritis Acute gastritis is a sudden inflammation of the lining of the stomach. •Acute gastritis can be divided in to; 1.Acute superficial gastritis 2.Erosive gastritis 3.Acute gastric ulceration
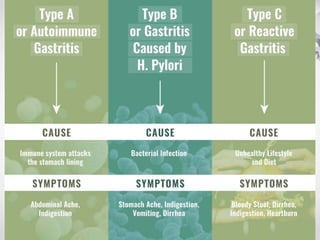
- 115. Cont'd • Chronic gastritis; inflammation of the lining of the stomach that occurs gradually and persists for a prolonged time. • Chronic gastritis can divided into: 1.TypeA chronic gastritis (autoimmune gastritis) 2.Type B chronic gastritis (chronic antral gastritis)
- 118. Etiology of Gastritis • Bacterial infections(.Hpylori): A bacteria that lives in the mucous lining of the stomach; without treatment, the infection can lead to ulcers, and in some people, stomach cancer. • Autoimmune Gastritis • Bile reflux: A backflow of bile into the stomach from the bile tract (that connects to the liver and gallbladder) • Regular use of pain relievers (NSAID) • Bile reflux disease • Stress • Alcohol addiction • Cocaine • Radiation and chemotherapy
- 120. Pathophysiology; • The gastric mucosa is protected from high acidity in stomach by mucous secretion. • Mucosal damage occur through; • Hypersecretion of acid • Reduction of mucus production • Generalized inflammation results
- 121. Pathophysiology;
- 122. Sign & Symptoms • Abdominal pain and burning, often in the upper center of the abdomen called the epigastric area • Bloating • Weight loss • Belching • Indigestion • Anorexia • Nausea with or without vomiting • Hiccups
- 123. Cont'd • Severe gastritis can lead to life-threatening symptoms including: • Severe chest pain • Feeling faint or short of breath • Severe abdominal pain • Sudden onset of bloody stools (blood may be red, black or tarry in texture) • Vomiting blood or black material (resembling coffee grounds)
- 126. Diagnosis of Gastritis; • Gastritis is diagnosed on the basis of medical history and physical examinations of the patient and the following tests: • Test for H pylori • Blood test • Stool test • Upper gastrointestinal X ray • Upper gastrointestinal endoscopy .An endoscope, a thin tube containing a tiny camera, is inserted through your mouth and down into your stomach to look at the stomach lining.
- 129. Medical treatment of Gastritis • T aking antacids and other drugs (such as proton pump inhibitors or H-2 blockers) to reduce stomach acid • Avoiding hot and spicy foods • For gastritis caused by H. pylori infection, your doctor will prescribe a regimen of several antibiotics plus an acid blocking drug (used for heartburn)
- 130. Cont'd • If the gastritis is caused by pernicious anemia, B12 vitamin shots will be given. • Eliminating irritating foods from your diet such as lactose from dairy or gluten from wheat • Once the underlying problem disappears, the gastritis usually does, too.
- 134. Nursing diagnosis for Gastritis • 1.Fluid And Electrolyte Imbalances related to inadequate intake, vomiting. • 2.Imbalanced Nutrition Less Than Body Requirements related to inadequate intake, anorexia. • 3. Impaired sense of comfort: acute pain related to gastric mucosal inflammation. • 4. Activity Intolerance related to physical weakness. • 5. Knowledge deficit related to lack of information.
- 135. Nursing Interventions • If thepatient is vomiting, give antiemetics. • Administer I.V. fluids as ordered to maintain fluid and electrolyte imbalance. • When the patient can tolerate oral feedings, provide a bland diet that takes into account his food preference. Restart feedings slowly. • Offer smaller, more frequent servings to reduce the amount of irritating gastric secretions. • Help patient identify specific foods that cause gastric upset and eliminate them from his diet.
- 136. Cont'd • Administer antacids and other prescribed medications as ordered. • If pain or nausea interferes with the patient’s appetite, administer pain medications or antiemetics about 1 hour before meals. • Monitor the patient’s fluid intake and output and electrolyte levels. • Assess the patient for presence of bowel sounds. • Monitor the patient’s response to antacids and other prescribed medications.
- 138. Nursing process • 1,Nursing Assessment for Gastritis • During the gathering health history, the nurse asked about the signs and symptoms in patients. • Does the patient have heartburn, can not eat, nausea or vomiting? • Does the patient have symptoms occur at any time, before or after meals?
- 139. Cont'd • Does the patient have symptoms associated with anxiety, stress, allergies, eating or drinking too much, or eating too fast? how the symptoms disappear? • Is there a history of previous gastric or stomach surgery? • Historical diet plus a new type of diet eaten for 72 hours, would help.
- 140. Cont'd • Full history is essential in helping nurses to identify whether excess dietary known, associated with current symptoms, whether others in the same patient has symptoms, whether the patient vomited blood, and if the elements are known to have ingested causes.
- 141. Nursing Diagnosis • Based on all the data assessment, nursing diagnosis is the major include the following: • Anxiety related to treatment. • Imbalanced Nutrition, Less Than Body Requirements related to inadequate nutrient input
- 142. Cont'd • Risk for Fluid Volume Deficit related to insufficient fluid intake and excessive fluid loss due to vomiting. • Knowledge Deficit r/t unfamiliarity with the disease process • Acute Pain related to gastric mucosal irritation.
- 143. Nursinh Care Plans for Gastritis • Imbalanced Nutrition: less than body requirements r/t insufficient absorption of nutrients • Expected Outcome: The patient can absorb an adequate amount of nutrients • Assessment and Intervention.Obtain the patient’s weight and other body measurements .
- 144. Cont'd • Admission weight serves as a baseline metric and helps guide. • Obtain information about the patient’s eating habits(Some food items can exacerbate the symptoms of gastritis. Acidic or citrus food items may worsen symptoms. ) • Place the patient NPO (nothing by mouth) in case of vomiting.
- 145. Cont'd • Discourage the patient from consuming spicy foods, caffeine, and alcohol. • Anticipate total parenteral nutrition (TPN). • Consult a dietitian if indicated. The patient might need an addition of supplements to compensate for insufficient nutrient intake. • Encourage small, frequent meals rather than three full meals.
- 146. Cont'd • 2 Risk for Fluid Volume Deficit: Risk factors: Vomiting; Decreased intake • Expected Outcome: The patient will have a stable fluid volume as evidenced by normal blood pressure, at least 30ml hourly urine output, and elastic skin turgor. • Assess for signs of dehydration. • Vital signs, especially blood pressure, urine output, and skin turgor.
- 147. Cont'd • Monitor how many times the patient vomits and note the amount of emesis each time. • Frequent vomiting causes fluid loss and can lead to dehydration. • Monitor the patient’s BP and HR. • Monitor electrolytes closely. • Frequent vomiting can cause a loss of electrolytes, especially potassium.
- 148. Cont'd • Monitor urine output hourly and note the color. • Provide oral care frequently. • Often patients are unable to eat or drink, which can leave the mouth dry. • Administer antiemetics as prescribed. • Antiemetics will reduce the feeling of nausea and vomiting and, therefore, the risk of insufficient fluid volume.
- 149. Cont'd • Monitor urine output hourly and note the color. • Provide oral care frequently. • Often patients are unable to eat or drink, which can leave the mouth dry. • Administer antiemetics as prescribed. • Antiemetics will reduce the feeling of nausea and vomiting and, therefore, the risk of insufficient fluid volume.
- 150. Cont'd • 3.Knowledge Deficit r/t unfamiliarity with the disease process • Expected Outcome: The patient will verbalize information about the causes, treatment, and prevention of gastritis • Assessment and Interventions: • Assess the patient’s knowledge about gastritis.
- 151. Cont'd • This information provides a baseline for further educational content. The patient might not be aware of the disease. • Teach about appropriate eating intervals and the types of food in case of a flare-up • Teach the patient not to take additional medication over the counter.
- 156. By the end of the session learners will be able to: Review the anatomy and physiology of gastrointestinal system (GIT) Define Peptic Ulcer disease. Discuss the causes, pathophysiology and manifestation of Peptic Ulcer disease. Discuss the diagnostic and medical and surgical management of Peptic Ulcer disease. Apply nursing management for patient with Peptic Ulcer disease. 5. Develop a teaching plan for a client experiencing Peptic Ulcer disease.
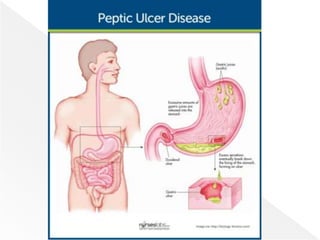
- 158. An Ulcer is … Erosion in the lining of the stomach or the first part of the small intestine, an area called the duodenum. Ulcers damage the mucosa of the alimentary tract, which extends through the muscularis mucosa into the sub mucosa or deeper.
- 159. A peptic ulcer is an excavation that forms in the mucosal wall of the stomach, in the pylorus, in the duodenum, or in the esophagus. The erosion of a circumscribed area may extend as deep as the muscle layers or through the muscle to the peritoneum. A peptic ulcer may be referred to as a gastric, duodenal, or esophageal ulcer, depending on its location.
- 160. Gastric ulcer. Gastric ulcer tend to occur in the lesser curvature of the stomach, near the pylorus. Duodenal ulcer. Peptic ulcers are more likely to occur in the duodenum than in the stomach. Esophageal ulcer. Esophageal ulcer occur as a result of the backward flow of HCl from the stomach into the esophagus
- 161. Ulcers that form in the stomach are called gastric ulcers; in the duodenum, they are called duodenal ulcers. Both types are referred to as peptic ulcers.
- 163. The gastroduodenal mucosal integrity is determined by protective (defensive) & damaging (aggressive) factors.
- 165. • Bicarbonate • Mucus layer • Prostaglandins • Mucosal blood flow • Epithelial renewal Defensive • Helicobacter pylori • NSAIDs • Pepsins • Bile acids • Smoking and alcohol Aggressive Mucosal damage erosions & ulcerations
- 166. Erosion. The erosion is caused by the increased concentration or activity of acid-pepsin or by decreased resistance of the mucosa. Damage. A damaged mucosa cannot secrete enough mucus to act as a barrier against HCl. Acid secretion. Patients with duodenal ulcers secrete more acid than normal, while patients with gastric ulcers tend to secrete normal or decreased levels of acid. Decreased resistance. Damage to the gastro duodenal mucosa results in decreased resistance to bacteria and thus infection from the H. pylori bacteria may occur.
- 167. • In the past it was believed lifestyle factors, such as stress and diet caused ulcers. Later, researchers determined that stomach acids -- hydrochloric acid and pepsin -- contributed to ulcer formation. • Today, research shows that most ulcers (80 percent of gastric ulcers and 90 percent of duodenal ulcers) develop as a result of infection with a bacterium called Helicobacter pylori (H. pylori). • It is believed that, although all three of these factors -- lifestyle, acid and pepsin, and H. pylori -- play a role in ulcer development, H. pylori is considered to be the primary cause.
- 169. Factors for the development of peptic ulcers include: Helicobacter pylori Research shows that most ulcers develop as a result of infection with bacterium called Helicobacter pylori (H. pylori). The bacterium produces substances that weaken the stomach's protective mucus and make it more susceptible to the damaging effects of acid and pepsin, as well as produce more acid.
- 170. Smoking: Studies show smoking increases the chances of getting an ulcer, slows the healing process of existing ulcers, and contributes to ulcer recurrence. Caffeine: Caffeine seems to stimulate acid secretion in the stomach, which can aggravate the pain of an existing ulcer. However, the stimulation of stomach acid cannot be attributed solely to caffeine
- 171. • Acid and pepsin It is believed that the stomach's inability to defend itself against the powerful digestive fluids, hydrochloric acid and pepsin, contributes to ulcer formation. • Nonsteroidal anti-inflammatory drugs (NSAIDs) These drugs (such as aspirin, ibuprofen, and naproxen sodium) make the stomach vulnerable to the harmful effects of acid and pepsin. They are present in many non-prescription medications used to treat fever, headaches, and minor aches and pains.
- 172. The following are the most common symptoms for ulcers, however, each individual may experience symptoms differently. Belching Nausea Vomiting Poor appetite Loss of weight Feeling tired and weak
- 173. Symptoms of ulcer may last for a few days, weeks, months, and may disappear only to reappear, often without an identifiable cause. Pain. As a rule, the patient with an ulcer complains of dull, gnawing pain or a burning sensation in the midepigastrium or the back that is relieved by eating. Pyrosis. Pyrosis (heartburn) is a burning sensation in the stomach and esophagus that moves up to the mouth.
- 174. Vomiting. Vomiting results from obstruction of the pyloric orifice, caused by either muscular spasm of the pylorus or mechanical obstruction from scarring. Constipation and diarrhea. Constipation or diarrhea may occur, probably as a result of diet and medications. Bleeding. 15% of patients may present with GI bleeding as evidenced by the passage of melena (tarry stools).
- 175. Bleeding. Perforation. Narrowing and obstruction.
- 176. Esophagogastroduodenoscopy. Confirms the presence of an ulcer and allows cytologic studies and biopsy to rule out H. pylori or cancer. Physical examination. A physical examination may reveal pain, epigastric tenderness, or abdominal distention. Barium study. A barium study of the upper GI tract may show an ulcer. Endoscopy. Endoscopy is the preferred diagnostic procedure because it allows direct visualization of inflammatory changes, ulcers, and lesions. Occult blood. Stools may be tested periodically until they are negative for occult blood.
- 177. Helicobacter pylori. Research has documented that peptic ulcers result from infection with the gram-negative bacteria H. pylori, which may be acquired through ingestion of food and water. H. pylori damage the mucous coating that protects the stomach and duodenum. Salicylates and NSAIDs. Encourages ulcer formation by inhibiting the secretion of prostaglandins. Various illnesses. Pancreatitis, hepatic disease, Crohn’s disease, gastritis, and Zollinger-Ellison syndrome are also known causes.
- 178. Excess HCl. Excessive secretion of HCl in the stomach may contribute to the formation of peptic ulcers. Irritants. Ingestion of milk and caffeinated beverages and alcohol also increase HCl secretion. These contribute by accelerating gastric emptying time and promoting mucosal breakdown. Blood type. Gastric ulcers tend to strike people with type A blood while duodenal ulcers tend to afflict people with type O blood.
- 179. Lifestyle changes: In the past, physicians advised people with ulcers to avoid spicy, fatty, or acidic foods. Smoking: Smoking has been shown to delay ulcer healing and has been linked to ulcer recurrence; therefore, people with ulcers should not smoke.
- 180. Medications: Physicians treat stomach and duodenal ulcers with several types of medications, including: H2-blockers to reduce the amount of acid the stomach produces by blocking histamine, a powerful stimulant of acid secretion. E.g. Cimetidine, Ranitidine, and Famotidine. Proton pump inhibitors to more completely block stomach acid production by stopping the stomach's acid pump -- the final step of acid secretion. E.g. Omeprazol.
- 181. • Mucosal protective agents to shield the stomach's mucous lining from the damage of acid, but do not inhibit the release of acid. E.g. Bismuth, Sucralfate • When treating H. pylori, these medications are often used in combination with antibiotics. • Antibiotics: The discovery of the link between ulcers and H. pylori resulted in a probable new treatment option -- antibiotics for patients with H. pylori.
- 182. H. pylori Therapy: • Triple therapy: Proton pump inhibitor Clarithromycin Amoxicillin.
- 183. At present, surgery is performed to treat ulcers. Types of surgery include: Vagotomy Pyloroplasty Antrectomy
- 184. Vagotomy: a surgical operation in which one or more branches of the vagus nerve are cut, typically to reduce the rate of gastric secretion (e.g. in treating peptic ulcers).
- 185. Pyloroplasty is surgery to widen the opening in the lower part of the stomach (pylorus) so that stomach contents can empty into the small intestine (duodenum). The pylorus is a thick, muscular area. When it thickens, food cannot pass through.
- 186. Surgical removal of the walls of an antrum, especially the antrum of the stomach.
- 187. Hemorrhage. Hemorrhage, the most common complication, occurs in 10% to 20% of patients with peptic ulcers in the form of hematemesis or melena. Perforation and penetration. Perforation is the erosion of the ulcer through the gastric serosa into the peritoneal cavity without warning, while penetration is the erosion of the ulcer through the gastric serosa into adjacent structures. Pyloric obstruction. Pyloric obstruction occurs when the area distal to the pyloric sphincter becomes scarred and stenosed from spasm or edema or from scar tissue that forms when an ulcer alternately heals and breaks down.
- 188. Pharmacologic therapy. Currently, the most commonly used therapy for peptic ulcers is a combination of antibiotics, proton pump inhibitors, and bismuth salts that suppress or eradicate the infection. Stress reduction and rest. Reducing environmental stress requires physical and psychological modifications on the patient’s part as well as the aid and cooperation of family members and significant others.
- 189. Smoking cessation. Studies have shown that smoking decreases the secretion of bicarbonate from the pancreas into the duodenum, resulting in increased acidity of the duodenum. Dietary modification. Avoiding extremes of the temperature of food and beverages and overstimulation from consumption of meat extracts, alcohol, coffee, and other caffeinated beverages, and diets rich in cream and milk should be implemented.
- 191. Assessment for a description of pain. Assessment of relief measures to relieve the pain. Assessment of the characteristics of the vomitus. Assessment of the patient’s usual food intake and food habits.
- 192. Acute pain related to the effect of gastric acid secretion on damaged tissue. Anxiety related to an acute illness. Imbalanced nutrition related to changes in the diet. Deficient knowledge about prevention of symptoms and management of the condition.
- 193. Relief of pain. Reduced anxiety. Maintenance of nutritional requirements. Knowledge about the management and prevention of ulcer recurrence. Absence of complications.
- 194. Administer prescribed medications. Avoid aspirin, which is an anticoagulant, and foods and beverages that contain acid-enhancing caffeine (colas, tea, coffee, chocolate), along with decaffeinated coffee. Encourage patient to eat regularly spaced meals in a relaxed atmosphere; obtain regular weights and encourage dietary modifications. Encourage relaxation techniques
- 195. Assess what patient wants to know about the disease, and evaluate level of anxiety; encourage patient to express fears openly and without criticism. Explain diagnostic tests and administering medications on schedule. Interact in a relaxing manner, help in identifying stressors, and explain effective coping techniques and relaxation methods. Encourage family to participate in care, and give emotional support.
- 196. Assess for faintness or dizziness and nausea, before or with bleeding; test stool for occult or gross blood; monitor vital signs frequently (tachycardia, hypotension, and tachypnea). Insert an indwelling urinary catheter and monitor intake and output; insert and maintain an IV line for infusing fluid and blood. Monitor laboratory values (hemoglobin and hematocrit). Insert and maintain a nasogastric tube and monitor drainage; provide lavage as ordered. Monitor oxygen saturation and administering oxygen therapy. Place the patient in the recumbent position with the legs elevated to prevent hypotension, or place the patient on the left side to prevent aspiration from vomiting.
- 197. Note and report symptoms of penetration (back and epigastric pain not relieved by medications that were effective in the past). Note and report symptoms of perforation (sudden abdominal pain, referred pain to shoulders, vomiting and collapse, extremely tender and rigid abdomen, hypotension and tachycardia, or other signs of shock).
- 198. Assist the patient in understanding the condition and factors that help or aggravate it. Teach patient about prescribed medications, including name, dosage, frequency, and possible side effects. Also identify medications such as aspirin that patient should avoid. Instruct patient about particular foods that will upset the gastric mucosa, such as coffee, tea, colas, and alcohol, which have acid-producing potential. Encourage patient to eat regular meals in a relaxed setting and to avoid overeating. Explain that smoking may interfere with ulcer healing; refer patient to programs to assist with smoking cessation.
- 199. Alert patient to signs and symptoms of complications to be reported. These complications include hemorrhage (cool skin, confusion, increased heart rate, labored breathing, and blood in the stool), penetration and perforation (severe abdominal pain, rigid and tender abdomen, vomiting, elevated temperature, and increased heart rate), and pyloric obstruction (nausea, vomiting, distended abdomen, and abdominal pain).
- 200. Relief of pain. Reduced anxiety. Maintained nutritional requirements. Knowledge about the management and prevention of ulcer recurrence. Absence of complications.
- 202. Gastric Carcinoma Subject: AHN I Sohaib Ali Shah Faculty of Nursing Sciences Khyber Medical University 202
- 203. Gastric Cancer • The incidence of stomach cancer in the United States has been decreasing, but it still causes a significant number of deaths annually. • More common in individuals over 40 years of age • Men have a higher incidence of gastric cancer than women. • The incidence of gastric cancer is higher in Japan, where mass screening programs have been implemented for early detection. • The prognosis for gastric cancer is generally poor, as most patients are diagnosed with metastases already present. 203
- 204. 204
- 205. Causes • Chronic stomach inflammation • Barrett's esophagus • Pernicious anemia • Achlorhydria • Gastric ulcers • H. pylori infection • Genetics • Food preservatives such as nitrates • Diet high in smoked, highly salted, or spiced foods 205
- 206. Manifestations •Early symptoms, such as pain relieved with antacids, can resemble those of benign ulcers. •Progressive disease may manifest with symptoms such as: anorexia (loss of appetite) dyspepsia (indigestion) weight loss abdominal pain Constipation Anemia nausea and vomiting 206
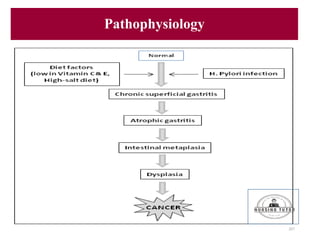
- 207. Pathophysiology 207
- 208. Diagnostic Procedure • Physical examination: Usually not helpful as most gastric tumors are not palpable. • Ascites: Apparent if the cancer cells have metastasized to the liver. • Endoscopy • Barium x-ray examination • Computed tomography (CT) scan • Bone scan • Liver scan • Complete x-ray examination of the GI tract 208
- 209. Medical & Surgical Management • Surgical removal: The only successful treatment for gastric carcinoma is the removal of the tumor. Cure is possible if the tumor is localized to the stomach and can be completely excised. • Palliative surgery: If the tumor has spread beyond resectable areas, palliative surgery may be performed to alleviate symptoms caused by obstruction or dysphagia. • Subtotal gastrectomy • Total gastrectomy • Chemotherapy • Pre-surgical chemotherapy • Radiation therapy • Tumor marker assessment • Learning Objectives 209
- 210. 210
- 211. Nursing Diagnosis • Imbalanced Nutrition: Less Than Body Requirements related to anorexia, altered taste sensation, and effects of cancer treatment. • Acute Pain related to tumor growth, invasion, or surgery. • Anxiety related to the diagnosis of gastric cancer, fear of treatment, or uncertainty about the future. • Risk for Infection related to impaired immune function secondary to cancer and/or treatment. • Risk for Imbalanced Fluid Volume related to vomiting, anorexia, and inadequate intake. • Disturbed Body Image related to changes in physical appearance due to cancer and treatment. • Fatigue related to the disease process, anemia, or cancer treatments. 211
- 212. Nursing Interventions Reduce Anxiety: • Provide a relaxed, non-threatening atmosphere for the patient to express fears, concerns, and anger • Encourage family support and positive coping measures • Advise patient about procedures and treatments • Suggest talking to a support person (e.g., spiritual advisor) Promote Optimal Nutrition: • Encourage small, frequent portions of non-irritating foods • Provide high-calorie food supplements with vitamins A and C and iron • Monitor intake, output, and daily weight • Assess for signs of dehydration and metabolic abnormalities • Administer antiemetics as prescribed 212
- 213. Nursing Interventions Relieve Pain: • Administer analgesics as prescribed • Assess the effectiveness of pain management • Suggest non-pharmacologic pain relief methods Provide Psychosocial Support: • Help the patient express fears, concerns, and grief • Answer patient's questions honestly and encourage participation in treatment decisions • Recognize mood swings and defense mechanisms • Reassure patients and family members that emotional responses are normal 213
- 214. Cont.. • Offer emotional support and involve family members and significant others • Make the services of healthcare professionals available if needed • Project an empathetic attitude and spend time with the patient 214
- 215. Irritable Bowel Syndrome (IBS) a functional disorder of intestinal motility (abnormal contractions) IBS results in a change in motility related to the neurologic regulatory system, infection or irritation, or a vascular or metabolic disturbance. It occurs more commonly in women than in men Causes: The cause of IBS is unknown, but various factors are associated with the syndrome, including heredity, psychological stress, a diet high in fat stimulating or irritating foods, alcohol consumption, and smoking. Manifestations: Symptoms of IBS vary in intensity and duration and include altered bowel patterns (constipation, diarrhea, or a combination of both), pain, bloating, abdominal distention. Abdominal pain is often relieved by defecation. Diagnostic Procedure: Stool studies, contrast x-ray studies, proctoscopy, barium enema, colonoscopy, manometry, electromyography Medical Management: Restriction and gradual reintroduction of foods that are possibly irritating, a healthy, high-fiber diet, exercise, stress reduction or behavior-modification programs, hydrophilic colloids, 2 1 5 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 216. antidiarrheal agents, antidepressants, anticholinergics, calcium channel blockers are some of the options to manage IBS symptoms. Nursing Process: Assessment: Gather information about the client's medical history, including any diagnoses or medications they are taking. Conduct a physical assessment of the client's abdomen, including any signs of distention, tenderness, or palpable masses. Assess the client's bowel habits, including frequency, consistency, and any associated symptoms such as abdominal pain or bloating. Explore the client's diet and exercise habits, as well as any stressors or triggers that may exacerbate their symptoms. Assess the client's mental health status, including any history of anxiety or depression. Diagnosis: Impaired bowel function related to Irritable Bowel Syndrome, as evidenced by altered bowel habits, abdominal pain, and bloating. Anxiety related to fear of unpredictable bowel habits and social embarrassment, as evidenced by reports of anxiety and avoidance of social situations. Planning: Collaborate with the client to develop a plan of care that includes dietary modifications, stress management techniques, and medications as appropriate. Encourage the client to keep a food diary to help identify trigger foods and adjust their diet accordingly. Educate the client on the importance of regular exercise and its positive effect on bowel function and stress reduction. Refer the client to a mental health professional or support group to address anxiety and provide coping strategies. Implementation: 2 1 6 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 217. Encourage the client to increase their intake of fiber-rich foods and drink plenty of water to improve bowel function. Educate the client on stress management techniques such as deep breathing, meditation, or progressive muscle relaxation. Administer medications as ordered, such as antispasmodics or antidepressants. Provide emotional support and reassurance to help alleviate anxiety and social embarrassment. Encourage the client to continue keeping a food diary to track progress and adjust their diet as needed. Encouraging regular meals, slow and thorough chewing, and adequate fluid intake, without taking fluid with meals, Discouraging alcohol use and cigarette smoking. Evaluation: Assess the client's bowel function and symptom relief on an ongoing basis, and adjust the plan of care as needed. Monitor the client's mental health status and refer for additional support as necessary. Encourage the client to maintain a healthy lifestyle and follow-up with their healthcare provider as recommended. Evaluate the effectiveness of the nursing interventions in promoting symptom relief and improving the client's quality of life. 2 1 7 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 218. Hernias: A hernia occurs when a segment of the intestine protrudes through a defect in the muscular wall of the abdomen, causing a lump or swelling. Types on basis of location: The most common types of hernias are umbilical, inguinal (Inguinal hernias are more common in men), and femoral hernias. Hernias can also form at an old abdominal surgical incision. In a reducible hernia, the protruding organ can be pushed back into place. In an irreducible/incarcerated hernia, the protruding organ is tightly wedged outside the cavity and cannot be pushed back. If the blood supply to the protruding organ is cut off, the hernia is considered to be strangulated or incarcerated. Causes: The most common contributing factors in the development of a hernia are straining to lift heavy objects, chronic cough, Chronic constipation, straining to void or pass stool, ascites. 2 1 8 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 219. Manifestations: A hernia presents as an abnormal pouching, a "lump," or local swelling out from the abdominal wall or in the groin area. Discomfort or pain may accompany the hernia, which worsens when pressure is applied to the area. When pressure is removed, the swelling disappears. An incarcerated hernia can cause intestinal obstruction, which is a medical emergency. Diagnostic procedures: Physical examination is the primary diagnostic tool. Imaging tests like ultrasound, CT scan, or MRI may also be used. Medical management: Conservative treatment may include wearing a truss or support garment to reinforce the weakened cavity wall and prevent protrusion of the intestines. However, surgery is the definitive treatment for hernias. Surgical management: The surgical procedure used in the treatment of a hernia is called a herniorrhaphy. The defect in the muscle is closed with sutures, and if the area of weakness is very large, a hernioplasty is done. In this procedure, some type of strong synthetic material is sewn over the defect to reinforce the area. Nursing Process: Assessment: Obtain a detailed health history to identify any risk factors for hernias such as obesity, smoking, chronic cough, and chronic constipation. Perform a physical examination to assess for the presence of a hernia, its location, size, and type (reducible or irreducible). Assess for signs and symptoms of complications such as pain, nausea, vomiting, fever, and abdominal distention. Obtain diagnostic tests such as ultrasound or CT scan to confirm the diagnosis. Diagnosis: 2 1 9 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 220. Risk for Complications related to hernia and potential for bowel obstruction or strangulation. Acute Pain related to hernia or surgical intervention. Anxiety related to surgical intervention and recovery process. Planning: Maintain a safe environment for the client and monitor for complications. Provide education about the condition, risk factors, and prevention measures. Administer pain medications as ordered and monitor for pain relief. Provide emotional support and coping strategies to reduce anxiety related to surgery. Prepare the client for surgery and postoperative care. Implementation: Monitor for signs of complications such as pain, nausea, vomiting, and abdominal distention. Administer pain medications as ordered and provide comfort measures such as ice packs and repositioning. Educate the client about postoperative care such as wound care, activity restrictions, and signs of complications. The patient is cautioned not to do heavy lifting, pulling, or pushing that increases intra-abdominal pressure. Lifting restrictions are usually implemented for 1 to 2 weeks. Patient is instructed to support the site with the hand if coughing or sneezing. Provide emotional support and coping strategies such as deep breathing exercises and guided imagery to reduce anxiety related to surgery. Prepare the client for surgery by providing information about the procedure, anesthesia, and recovery process. Evaluation: Monitor the client's response to interventions and adjust care plan as necessary. Evaluate pain relief and monitor for signs of complications. Assess the client's understanding of the condition and postoperative care. Evaluate the effectiveness of emotional support and coping strategies in reducing anxiety related to surgery. 2 2 0 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 221. Monitor the client's progress toward recovery and provide additional interventions as needed. Intestinal obstruction caused by blockage that prevents normal flow of intestinal contents. Two types of obstruction: mechanical and functional. Mechanical obstruction can be caused by intraluminal or mural obstruction, examples include adhesions, hernias, and tumors. Functional obstruction can be caused by muscular or neurological disorders. Obstruction can be partial or complete and severity depends on the location and degree of occlusion and vascular supply to bowel wall. Small intestine is more commonly affected, with adhesions being the most common cause, followed by hernias and neoplasms. Other causes include intussusception, volvulus (ie, twisting of the bowel), and paralytic ileus. Large bowel obstruction occurs less frequently and is most commonly found in the sigmoid colon with causes such as carcinoma, diverticulitis, inflammatory bowel disorders, and tumors. Small bowel obstruction (SBO) 2 2 1 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 222. Small bowel obstruction (SBO) is a blockage that occurs in the small intestine, which prevents the normal passage of intestinal contents. causes adhesions, hernias, tumors, intussusception volvulus. Manifestations: The accumulation of intestinal contents, fluid, and gas above the obstruction leads to abdominal distention, vomiting, dehydration hypovolemic shock. Diagnosis physical examination, imaging studies, such as abdominal x-rays. Laboratory studies (ie, electrolyte studies and a complete blood cell count) reveal a picture of dehydration, loss of plasma volume, and possible infection. Medical management involves decompression of the bowel through a nasogastric or small bowel tube. Before surgery, intravenous therapy is necessary to replace the depleted water, sodium, chloride, and potassium. Surgery is necessary in cases of complete bowel obstruction or strangulation. The complexity of the surgical procedure depends on the duration of the obstruction and the condition of the intestine. Nursing management for a nonsurgical patient with SBO involves maintaining the function of the nasogastric tube, monitoring fluid and electrolyte balance, assessing nutritional status, and evaluating improvement in symptoms. 2 2 2 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 223. The nurse should report any discrepancies in intake and output, worsening of pain or abdominal distention, and increased nasogastric output. If the patient's condition does not improve, the nurse prepares them for surgery. After surgical repair of SBO, nursing care is similar to that for other abdominal surgeries, o including monitoring vital signs, o assessing for signs of infection or bleeding, o monitoring the functioning of the nasogastric tube, o and encouraging ambulation and deep breathing exercises. o Pain management, wound care, and monitoring for potential complications Large bowel obstruction occurs when the large intestine is blocked, leading to the accumulation of intestinal contents, fluid, and gas proximal to the obstruction. If the blood supply to the colon is disturbed, intestinal strangulation and necrosis can occur, which is life-threatening. Symptoms develop and progress slowly, and patients may experience constipation, marked abdominal distension, crampy lower abdominal pain, fecal vomiting. Diagnosis based on symptoms x-ray studies, and barium studies are contraindicated. Medical management involves colonoscopy to untwist and decompress the bowel, cecostomy for poor surgical risks, rectal tube to decompress an area lower in the bowel, 2 2 3 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 224. Surgical Surgical resection to remove the obstructing lesion, temporary or permanent colostomy, or ileoanal anastomosis if the entire large colon needs to be removed. Nursing Process: Assessment: Collect subjective and objective data from the client, such as abdominal pain or cramping, nausea, vomiting, constipation or diarrhea, bloating, and distension. Monitor vital signs, including blood pressure, pulse rate, respiratory rate, and temperature. Assess bowel sounds, frequency, and character of bowel movements. Review the client's medical history, including any previous episodes of intestinal obstruction, surgery, or chronic medical conditions. Perform a physical exam to assess for abdominal tenderness, rebound tenderness, guarding, and palpable masses. Diagnosis: Impaired Gas Exchange related to decreased oxygenation secondary to abdominal distension and pain Acute Pain related to abdominal distension and increased intraluminal pressure Risk for Deficient Fluid Volume related to vomiting, diarrhea, and/or inadequate oral intake Risk for Imbalanced Nutrition: Less Than Body Requirements related to inadequate oral intake or bowel obstruction Planning: Administer oxygen therapy as needed to maintain adequate oxygenation and respiratory function. Administer pain medications as prescribed and monitor their effectiveness. 2 2 4 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 225. Monitor fluid intake and output and administer intravenous fluids as prescribed to maintain hydration and electrolyte balance. Collaborate with the dietitian to develop a nutrition plan that meets the client's needs and restrictions. Prepare the client for diagnostic tests or surgical interventions as needed. Implementation: Administer oxygen therapy as prescribed and monitor respiratory status. Administer pain medications as prescribed and monitor their effectiveness. Administer intravenous fluids as prescribed and monitor fluid and electrolyte balance. Provide small, frequent meals and snacks that are easy to digest and low in fiber. Encourage the client to ambulate and engage in other activities to promote bowel motility. Educate the client and family about the condition, treatment, and ways to prevent future episodes. Providing emotional support and comfort Preoperative teaching, postoperative wound care and nursing care. Evaluation: Monitor the client's response to treatment, including vital signs, pain level, fluid and electrolyte balance, and bowel function. Modify the care plan as needed based on the client's progress and response to treatment. Evaluate the client's understanding of the condition, treatment, and self-care measures. Provide follow-up care and referrals as needed, such as for dietary counseling or physical therapy. 2 2 5 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 226. Hemorrhoids Hemorrhoids are swollen and inflamed veins located in the lower anal canal i-e rectum and anus. They can occur internally or externally and are a common condition that affects many people. Internal hemorrhoids Above the internal sphincter are called internal hemorrhoids, occur above the dentate line within the anal canal and are covered by mucous membrane. They are not visible from the outside and can be difficult to diagnose without the use of an anoscope or proctoscope. Symptoms of internal hemorrhoids may include bleeding during bowel movements, itching, and prolapse. External hemorrhoids appearing outside the external sphincter are called external hemorrhoids occur below the dentate line and are covered by skin. They can be seen and felt as a lump or swelling around the anus. Symptoms of external hemorrhoids may include pain, swelling, and itching around the anus. 2 2 6 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 227. Causes: Constipation, obesity, prolonged standing or sitting Shearing of the mucosa during defecation Increased pressure in the hemorrhoid tissue due to pregnancy Enlargement of the prostate, uterine fibroids, and rectal tumors Chronic liver disease with portal hypertension Manifestations: Itching and pain Bright red bleeding with defecation Severe pain from inflammation and edema caused by thrombosis (ischemia and necrosis) in external hemorrhoids Internal hemorrhoids are not usually painful until they bleed or prolapse when they become enlarged. Diagnostic procedure: Visual examination of the anal area (DRE) anoscopy, sigmoidoscopy, or colonoscopy Medical management: Good personal hygiene and avoiding excessive straining during defecation High-residue diet that contains fruit and bran along with an increased fluid intake Hydrophilic bulk-forming agents such as psyllium and mucilloid Warm compresses, sitz baths, analgesic ointments and suppositories, astringents (eg, witch hazel), and bed rest Surgical management: scleropathy (injection of a solution that causes the vessel to dry up and disintegrate), 2 2 7 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 228. cryotherapy (freezing), photocoagulation (burning), infrared coagulation (IRC) Rubber-band ligation procedure Cryosurgical hemorrhoidectomy Hemorrhoidectomy or surgical excision Nursing Process: Assessment: Obtain a thorough health history, including any history of hemorrhoids, bowel habits, and medication use. Perform a physical examination, including a visual inspection of the anus and rectum, to assess for the presence of hemorrhoids. Assess for signs and symptoms of hemorrhoids, such as bleeding, itching, pain, and swelling. Assess the client's ability to manage bowel movements and perform personal hygiene. Diagnosis: Risk for constipation related to pain and discomfort associated with hemorrhoids Risk for impaired skin integrity related to itching and scratching Acute pain related to inflammation and swelling of hemorrhoids Planning: Provide education to the client on proper bowel habits and personal hygiene practices to prevent further irritation and inflammation of hemorrhoids. Administer medications as ordered for pain and discomfort. Use sitz baths or warm compresses to help reduce swelling and discomfort. 2 2 8 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 229. Monitor for signs of bleeding and infection. Implementation: Encourage the client to consume a high-fiber diet and increase fluid intake to promote regular bowel movements. Administer stool softeners or laxatives as ordered to prevent straining during bowel movements. Apply topical medications, such as hydrocortisone cream or witch hazel, to relieve itching and inflammation. Instruct the client on proper hygiene practices, including gentle wiping after bowel movements and the use of moistened wipes or a bidet. Encourage the client to avoid prolonged sitting or standing, which can worsen hemorrhoid symptoms. Administer oxygen therapy as needed to maintain adequate oxygenation and respiratory function in cases of severe bleeding or shock. Educate the patient about warm compresses, sitz baths, analgesic ointments and suppositories, astringents (eg, witch hazel), and bed rest Monitor for bleeding, infection, and pain after surgical procedures. Evaluation: Monitor the client's response to treatment and adjust interventions as needed. Evaluate the client's ability to manage bowel movements and perform personal hygiene practices. Assess for signs of bleeding or infection and report to the healthcare provider as needed. Provide ongoing education and support to the client to prevent future episodes of hemorrhoids. 2 2 9 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 230. Colorectal cancer a common cancer that affects the colon and rectum. Colorectal cancer, also known as colon cancer or rectal cancer. It typically develops slowly over a period of several years, starting as a non-cancerous growth called a polyp that can become cancerous over time. Colorectal cancer is one of the most common types of cancer, and early detection through screening can greatly improve treatment outcomes. Causes: The exact cause of the disease is unknown Several risk factors have been identified, including age, family history of colon cancer, inflammatory bowel disease, and polyps. Adenocarcinoma is the most common type of colorectal cancer, and it may start as a benign polyp that becomes malignant and invades and destroys normal tissues, eventually spreading to other parts of the body. Manifestations: include a change in bowel habits, blood in the stools, unexplained anemia, anorexia, weight loss, and fatigue. Diagnostic procedures include fecal occult blood testing, barium enema, proctosigmoidoscopy, and colonoscopy. Carcinoembryonic antigen (CEA) studies may also be performed to predict prognosis. Medical Treatment 2 3 0 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 231. for colorectal cancer depends on the stage of the disease and typically involves surgery to remove the tumor, supportive therapy, adjuvant therapy, which may include chemotherapy, radiation therapy, immunotherapy, or multimodality therapy. Adjuvant therapy delays tumor recurrence and increases survival time for patients who receive it. Surgical Treatment includes segmental resection with anastomosis, abdominoperineal resection with permanent sigmoid colostomy, temporary colostomy followed by segmental resection and anastomosis, permanent colostomy or ileostomy, and construction of a coloanal reservoir called a colonic J pouch. 2 3 1 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 232. Nursing Process Assessment: 1. Obtain the client's medical history, including any previous cancer treatments, medications, and surgical interventions. 2. Assess the client's symptoms, such as changes in bowel habits, rectal bleeding, abdominal pain, anemia, weight loss, or fatigue. 3. Evaluate the client's nutritional status, including their dietary habits, appetite, and weight. 4. Assess the client's psychological and emotional well-being, including any anxiety, depression, or coping mechanisms. 5. Evaluate the client's understanding of their diagnosis, treatment plan, and potential side effects. Diagnosis: 1. Impaired bowel elimination related to colorectal cancer as evidenced by changes in bowel habits, rectal bleeding, and abdominal pain. 2. Imbalanced nutrition: less than body requirements related to the effects of cancer and its treatment as evidenced by weight loss, anemia, and altered dietary habits. 3. Anxiety related to diagnosis and treatment of colorectal cancer as evidenced by the client's verbalization of worry and apprehension. Planning: 1. The client will maintain normal bowel elimination through interventions such as increasing fiber and fluid intake, as well as adhering to the prescribed bowel regimen. 2. The client will achieve a stable weight and balanced nutrition through interventions such as nutritional counseling, encouraging small frequent meals, and monitoring for signs of malnutrition. 3. The client will demonstrate a decrease in anxiety through interventions such as providing emotional support, allowing for the expression of feelings, and promoting relaxation techniques. 2 3 2 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 233. Implementation: 1. Collaborate with the healthcare team to develop and implement the prescribed treatment plan, which may include surgery, chemotherapy, radiation therapy, or a combination of these interventions. 2. Provide education on healthy dietary habits, including increasing fiber and fluid intake, and avoiding foods that may aggravate bowel symptoms. 3. Administer medications as prescribed, including pain medications, anti-nausea medications, and other symptom management medications. 4. Monitor for and manage potential side effects of treatment, such as fatigue, nausea, vomiting, diarrhea, and constipation. 5. Patients with colorectal cancer are at risk for developing infections due to impaired immune function. The nurse should closely monitor the patient for signs and symptoms of infection, such as fever, chills, and increased white blood cell count. 6. Provide emotional support and counseling to the client and their family members throughout the treatment process. 7. Patients with colorectal cancer may experience discomfort and distress due to their disease and treatment. The nurse should provide comfort measures, such as positioning, relaxation techniques, and emotional support, to help alleviate these symptoms. 8. Encourage the client to participate in support groups, counseling services, or other community resources to address their emotional and psychological needs. Evaluation: 1. Assess the effectiveness of interventions aimed at maintaining normal bowel elimination, stable weight, and balanced nutrition. 2. Monitor for improvements in the client's anxiety levels, as well as their ability to cope with the diagnosis and treatment of colorectal cancer. 2 3 3 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 234. 3. Reassess the treatment plan and modify as needed based on the client's response and progress toward their goals. 2 3 4 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 235. antidiarrheal agents, antidepressants, anticholinergics, calcium channel blockers are some of the options to manage IBS symptoms. Nursing Process: Assessment: Gather information about the client's medical history, including any diagnoses or medications they are taking. Conduct a physical assessment of the client's abdomen, including any signs of distention, tenderness, or palpable masses. Assess the client's bowel habits, including frequency, consistency, and any associated symptoms such as abdominal pain or bloating. Explore the client's diet and exercise habits, as well as any stressors or triggers that may exacerbate their symptoms. Assess the client's mental health status, including any history of anxiety or depression. Diagnosis: Impaired bowel function related to Irritable Bowel Syndrome, as evidenced by altered bowel habits, abdominal pain, and bloating. Anxiety related to fear of unpredictable bowel habits and social embarrassment, as evidenced by reports of anxiety and avoidance of social situations. Planning: Collaborate with the client to develop a plan of care that includes dietary modifications, stress management techniques, and medications as appropriate. Encourage the client to keep a food diary to help identify trigger foods and adjust their diet accordingly. Educate the client on the importance of regular exercise and its positive effect on bowel function and stress reduction. Refer the client to a mental health professional or support group to address anxiety and provide coping strategies. Implementation: Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 236. Appendicitis: The appendix is a small, finger-like appendage attached to the cecum. It fills with food and empties into the cecum, but its small lumen and inefficient emptying make it prone to obstruction and infection i-e (Appendicitis) Pathophysiology: Appendicitis occurs when the appendix becomes inflamed and edematous due to factors such as fecaliths, tumors, or foreign bodies. This leads to increased intraluminal pressure and severe abdominal pain localized in the right lower quadrant. Eventually, the inflamed appendix fills with pus. Causes: Obstructions such as fecaliths, tumors, or foreign bodies that lead to inflammation and infection. Infection of the gastrointestinal tract can sometimes spread to the appendix, leading to appendicitis. Inflammation of the gastrointestinal tract, such as in conditions like Crohn's disease or ulcerative colitis, can increase the risk of developing appendicitis. Trauma to the abdomen, such as a blunt injury or abdominal surgery, can trigger appendicitis. 2 3 6 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 237. Manifestations: Vague epigastric or periumbilical pain that progresses to right lower quadrant pain Accompanied by low-grade fever, nausea, vomiting, and loss of appetite. Local tenderness at McBurney's point and rebound tenderness may be present. Patient may rest with the right thigh drawn up. Extending the leg causes pain. Diagnostic Procedures: Physical examination, laboratory tests (elevated white blood cell count, neutrophil count) imaging studies (abdominal x-ray films, ultrasound, CT scans) that reveal signs of appendicitis. Medical Treatment: Prior to surgery, antibiotics and intravenous fluids are administered to correct or prevent fluid imbalance and dehydration. Analgesics are given for pain relief. Surgical Treatment: Appendectomy is performed as soon as possible to reduce the risk of appendix perforation. It can be done under general or spinal anesthesia with a low abdominal incision or through laparoscopy. Nursing Process: Assessment: 2 3 7 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 238. Perform a comprehensive physical assessment, including vital signs, pain assessment, and abdominal examination to assess for localized tenderness, rebound tenderness, and rigidity. Obtain a detailed health history, including the onset and progression of symptoms, past medical history, and any associated factors. Review laboratory and diagnostic test results, such as complete blood count, to assess for elevated leukocyte and neutrophil counts. Assess the client's level of pain, nausea, and other associated symptoms. Evaluate the client's understanding of the condition and provide an opportunity for them to express concerns and ask questions. Diagnosis: Acute pain related to inflammation and distention of the appendix. Risk for infection related to appendiceal obstruction and inflammation. Deficient knowledge related to the diagnosis, treatment, and postoperative care of appendicitis. Planning: Ensure pain management by administering prescribed analgesics, providing comfort measures, and promoting rest. Prevent infection by administering prescribed antibiotics and monitoring vital signs for signs of systemic infection. Educate the client and family about appendicitis, treatment options, and the importance of postoperative care. Collaborate with the healthcare team to prepare the client for surgery, including obtaining informed consent, completing preoperative assessments, and providing necessary preoperative instructions. 2 3 8 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 239. Prepare the client for potential surgical intervention, including the insertion of intravenous lines and fasting prior to surgery. Implementation: Preparing the patient for surgery involves administering intravenous fluids to replace fluid loss, promote renal function Administering antibiotic therapy to prevent infection. If there is evidence or likelihood of paralytic ileus, a nasogastric tube may be inserted. Enema administration is avoided to prevent perforation. Postoperative Care: After surgery, the patient is placed in a semi-Fowler position to reduce tension on the incision and abdominal organs, which helps reduce pain. Pain relief is achieved through the administration of opioids, typically morphine sulfate. Oral fluids are gradually introduced once tolerated, while intravenous fluids are given to patients who were dehydrated before surgery. Food is provided based on the patient's desires and tolerance on the day of surgery. Discharge may be possible on the day of surgery if the patient's temperature is within normal limits, there is no undue discomfort in the operative area, and the appendectomy was uncomplicated. Discharge teaching is crucial and includes instructions to make a follow-up appointment for suture removal, incision care, activity guidelines, and resumption of normal activities within 2 to 4 weeks. In cases where there is a possibility of peritonitis, a drain may be left in place at the incision site, and patients at risk for complications are 2 3 9 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 240. closely monitored for signs of intestinal obstruction or secondary hemorrhage. Secondary abscesses may develop in the pelvis, under the diaphragm, or in the liver, leading to an elevated temperature, increased pulse rate, and leukocyte count. Prior to discharge, the nurse educates the patient and family on incision care, dressing changes, and irrigations as prescribed. A home care nurse may be involved in assisting with care, monitoring for complications, and assessing wound healing. Evaluation: Assess the effectiveness of pain management interventions by monitoring the client's pain level and evaluating their response to analgesics. Monitor vital signs and laboratory values to determine the client's response to antibiotic therapy and identify any signs of infection. Evaluate the client's understanding of the condition and their ability to manage postoperative care through verbalization and demonstration of wound care techniques. Assess the client's surgical outcomes, including wound healing, absence of complications, and return of normal bowel function. Seek feedback from the client and family to evaluate their satisfaction with the provided care and address any additional concerns. 2 4 0 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 241. Peritonitis Peritonitis is inflammation of the peritoneum, the membrane lining the abdominal cavity and covering the abdominal organs. Causes: bacterial infection from gastrointestinal (GI) tract or internal reproductive organs in women. injury or trauma inflammation that extends from organs outside the peritoneal area, such as the kidney. Other common causes of peritonitis o appendicitis, o perforated ulcer, o diverticulitis, o bowel perforation, and it can also be associated with abdominal surgeries and peritoneal dialysis. Clinical manifestations diffuse pain initially, which becomes localized and intense near the site of inflammation. Abdominal tenderness, distention, rigidity, rebound tenderness, nausea, vomiting, 2 4 1 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 242. and diminished peristalsis may also be present. Increased temperature, pulse rate, and leukocyte count are common. Diagnostic findings elevated leukocyte count, possible low hemoglobin and hematocrit levels, altered electrolyte levels, abdominal x-ray showing air and fluid levels, CT scan revealing abscess formation, peritoneal aspiration with culture and sensitivity studies to identify causative organisms. Medical management Fluid, colloid, and electrolyte replacement is a primary focus of medical management in peritonitis. Analgesics are prescribed for pain management Antiemetics are given to alleviate nausea and vomiting. Intestinal intubation and suction are used to relieve abdominal distention and promote intestinal function. Fluid accumulation in the abdominal cavity can restrict lung expansion and lead to respiratory distress. Oxygen therapy via nasal cannula or mask is used to ensure adequate oxygenation. Massive antibiotic therapy is initiated early to treat the infection. Surgical objectives involve removing infected material and addressing the underlying cause. Surgical treatments may include excision (e.g., removal of the appendix), resection with or without anastomosis (e.g., intestine), repair (e.g., perforation), and drainage (e.g., abscess). 2 4 2 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 243. In cases of extensive sepsis, a fecal diversion may be necessary. Nursing Process: Assessment: Gather subjective data: Obtain medical history, assess symptoms, inquire about recent trauma. Collect objective data: Perform physical examination, monitor vital signs, assess for dehydration and respiratory distress. Diagnosis: Acute Pain related to inflammation and distention of the peritoneum. Deficient Fluid Volume related to fluid shifting into the peritoneal cavity. Risk for Infection related to bacterial invasion and peritoneal contamination. Impaired Gas Exchange related to abdominal distention and pressure on the diaphragm. Imbalanced Nutrition: Less Than Body Requirements related to decreased oral intake and metabolic demands. Planning: Goal: Relieve pain and discomfort. Goal: Restore and maintain fluid balance. Goal: Prevent infection and promote wound healing. Goal: Ensure adequate oxygenation and respiratory function. Goal: Meet nutritional needs. Implementation: 2 4 3 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 244. Administer prescribed analgesics, provide positioning for comfort, apply heat or cold therapy, and encourage relaxation techniques. Administer intravenous fluids, monitor fluid intake and output, assess for dehydration, and monitor electrolyte levels. Administer broad-spectrum antibiotics, monitor temperature and signs of infection, ensure aseptic wound care, and promote hygiene practices. Administer oxygen therapy as needed, monitor respiratory status, encourage deep breathing and coughing exercises, and optimize lung expansion. Collaborate with the dietitian to provide a well-balanced diet, administer enteral or parenteral nutrition if necessary, and monitor weight and nutritional markers. Educate the client and family about the condition, medications, dietary modifications, wound care, hygiene practices, and the importance of follow-up appointments. Evaluation: Assess pain relief and response to analgesics. Monitor fluid balance, urine output, and electrolyte levels. Evaluate effectiveness of antibiotic therapy and monitor for signs of infection. Evaluate respiratory status, oxygen saturation, and signs of distress. Monitor nutritional status, weight, and intake to address deficiencies. 2 4 4 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 245. Inflammatory Bowel Disease (Ulcerative Colitis and Crohn Disease) Inflammatory bowel disease (IBD) includes ulcerative colitis (UC) and Crohn's disease. 2 4 5 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 246. Causes: Genetic predisposition UC is three times more common than Crohn's disease. Higher prevalence among the Jewish population. Immunologic activity is believed to play a role in both conditions, as anticolon antibodies are often present in the blood. In ulcerative colitis, acute attacks can be triggered by infections and emotional tension. Factors such as environmental triggers, genetics, immune system dysfunction, and alterations in gut microbiota are implicated in IBD development. Manifestations: Attacks of diarrhea that may be bloody and contain mucus Abdominal pain with cramping Malaise (general feelings of discomfort or unease) Fever during flare-ups Weight loss Stool color dependent on the location and severity of bleeding (black, tarry stool with slow bleeding; reddish stool with frequent diarrhea) Flare-ups triggered by physical or emotional stress Periods of remission after flare-ups (lasting from weeks to decades) Some patients experience only one attack, while others have recurring symptoms Serious intestinal hemorrhage with fluid and electrolyte imbalances in some cases 2 4 6 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 247. Diagnostic Procedures: patient's medical history and symptoms. Colonoscopy, flexible sigmoidoscopy, mucosal biopsy, barium enema, stool analysis may be performed to confirm the diagnosis. Medical Treatment: Treatment for ulcerative colitis (UC) and Crohn's disease varies based on the severity and frequency of symptoms. Conservative medical treatment approaches include: Administration of antidiarrheal drugs to control diarrhea. Long-term sulfasalazine therapy, which is an anti-inflammatory medication. Medications to relieve abdominal cramps. The recommended diet for UC and Crohn's disease consists of low-fat, low-fiber foods that are high in protein and calories. Small frequent feedings are recommended. Some patients benefit from lactose avoidance. Corticosteroids are used for moderate to severe cases to reduce inflammation. Fluid replacement may be necessary during acute attacks. Blood transfusions are given when anemia is present. Oral 5-aminosalicylic acid (5-ASA) derivatives, such as olsalazine sodium (Dipentum), are useful alternatives for patients who cannot tolerate sulfasalazine. Budesonide (Entocort) is used to help control disease in the ileum. 2 4 7 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 248. For patients with advanced disease who are not surgical candidates, medications such as azathioprine, 6-mercaptopurine, methotrexate, levamisole, or cyclosporine may be used to help control the disease. Infliximab (Remicade), a monoclonal antibody against tumor necrosis factor, has a high response rate of over 80% for Crohn's disease but only about a 50% success rate for UC. It is administered intravenously according to a specific protocol. Certolizumab pegol (Cimzia) is a drug specifically for patients with moderate to severe Crohn's disease who have not responded to conventional treatments. Surgical Treatment: Surgical intervention is considered as an alternative treatment for some patients with UC and Crohn's disease. The surgical procedure typically involves the removal of the affected portion of the bowel, often through proctocolectomy. In UC, patients may be candidates for alternative surgical options such as: Ileal reservoir (Kock pouch): This procedure involves creating a reservoir from the ileum, allowing the patient to have control over waste discharge. A collection pouch is not necessary, and the patient uses a catheter to empty the reservoir. Ileoanal anastomosis: This procedure allows the patient to retain control over the anal sphincter for voluntary defecation. It eliminates the need for an external pouch or bag for waste collection. 2 4 8 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 249. These alternative procedures are not typically performed for Crohn's disease because as the disease progresses, the area of the reservoir can become involved and affected by the disease. Nursing Management: Assessment: Gather comprehensive health history, including previous diagnoses, symptoms, and treatment of IBD. Perform a physical examination, with a focus on the abdomen, noting any tenderness, distention, or masses. Assess vital signs, including temperature, heart rate, blood pressure, and respiratory rate. Monitor laboratory values, such as complete blood count, electrolytes, and inflammatory markers. Assess the client's nutritional status, fluid balance, and bowel elimination patterns. Evaluate the client's emotional well-being and coping strategies related to living with a chronic illness. Diagnosis: Acute/chronic pain related to intestinal inflammation. Imbalanced nutrition: less than body requirements related to malabsorption and increased metabolic demands. Risk for fluid volume deficit related to diarrhea. Anxiety related to the unpredictable nature of IBD and its impact on daily life. 2 4 9 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 250. Planning: Collaborate with the client to establish realistic goals and expectations for managing pain, improving nutrition, maintaining fluid balance, and reducing anxiety. Develop an individualized care plan with specific interventions to address each nursing diagnosis. Educate the client about the importance of adhering to prescribed medications, dietary modifications, and self-care strategies. Involve the client's family or support system in the planning process to enhance understanding and support. Implementation: Administer prescribed analgesics and monitor the client's response to pain management interventions. Provide nutritional counseling, including a low-fat, low-fiber diet, and encourage small, frequent meals. Monitor fluid intake and output, offer oral rehydration solutions, and provide intravenous fluids as necessary. Teach stress reduction techniques, such as deep breathing exercises and guided imagery, to help alleviate anxiety. Educate the client on the importance of medication compliance and regular follow-up appointments. Evaluation: Assess the client's pain level and document the effectiveness of pain management interventions. Monitor the client's nutritional status and document improvements in weight, appetite, and laboratory values. 2 5 0 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 251. Evaluate the client's fluid balance and document resolution of fluid volume deficit. Assess the client's anxiety levels and document any changes in coping strategies and overall emotional well-being. Review the client's progress towards achieving the established goals and make necessary adjustments to the care plan. 2 5 1 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 252. Anorectal Abscess: An anorectal abscess is a localized collection of pus that forms in the anal or rectal area due to an infection. It occurs when an anal gland becomes obstructed, leading to a retrograde infection and subsequent abscess formation. Causes: The obstruction of anal glands is the primary cause of anorectal abscesses. This can be due to various factors, such as trauma, inflammation, or infections. People with certain conditions, including regional enteritis (Crohn's disease) or immunosuppressive conditions like AIDS, are more susceptible to developing anorectal abscesses. Manifestation: Localized pain, tenderness, and swelling in the anal or rectal area. Redness and warmth around the affected area. Fever, lower abdominal pain and systemic signs of infection in deeper abscesses. Foul-smelling discharge or pus may be present. Diagnostic Procedure: Primarily based on clinical examination. Evaluate the symptoms, perform a physical examination of the anal and rectal area, and assess for signs of infection. imaging studies (ultrasound, MRI) may be recommended to determine the extent and location of the abscess. 2 5 2 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 253. Medical Management: Palliative medical management aims to provide temporary relief and includes: Sitz baths: Soaking the affected area in warm water can help reduce pain and promote healing. Analgesics: Pain medications may be prescribed to alleviate discomfort. Surgical Management: Prompt surgical intervention is the preferred treatment for anorectal abscesses. The surgical management involves the following procedures: Incision and Drainage: The abscess is surgically incised and drained to remove the accumulated pus. Fistula Excision: If a fistula (an abnormal connection between the abscess and surrounding tissues) is present or suspected, it is excised during the abscess drainage procedure. In some cases, a separate procedure may be required to remove the fistulous tract. Wound Care: Following surgical drainage, the wound may be packed with gauze to promote healing by granulation. Antibiotics may be prescribed to prevent or treat infection. Anal Fistula: An anal fistula is a small, tubular tract that extends from an opening located near the anus. It forms as a result of an infection or other factors and creates a passage between the anal canal and the skin surrounding the anus. Causes: Anal fistulas are commonly caused by infections that originate from an anal gland or anorectal abscess. Other possible causes include trauma, fissures (tears in the lining of the anus), inflammatory bowel disease (such as Crohn's disease), or radiation therapy. Manifestation: 2 5 3 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 254. 3 Constant leakage of pus or stool from the cutaneous opening near the anus. Passage of flatus (gas) or feces from the vagina or bladder, depending on the path of the fistula tract. Discomfort, pain, swelling, or redness around the anus. Recurrent infections or abscesses in the anal area. Diagnostic Procedure: Physical Examination: A healthcare professional will conduct a physical examination of the anal area to assess for the presence of an opening, signs of infection, and other associated symptoms. Probing: A probe may be used to determine the course and depth of the fistula tract. Imaging Studies: In some cases, imaging tests such as MRI or endoanal ultrasound may be recommended to obtain detailed information about the fistula's anatomy and to assess any associated complications. Medical Management: Antibiotics: Prescribed to treat or prevent infection. Pain medication: To alleviate discomfort. Stool softeners: To prevent constipation and ease bowel movements. Surgical Management: Surgery is the primary treatment for anal fistulas. The surgical management involves: Fistulectomy: The recommended surgical procedure, which involves the excision (removal) of the fistulous tract. The lower bowel is emptied with prescribed enemas before the surgery. During surgery, the fistula tract is identified by probing or injecting a colored solution (e.g., methylene blue) to aid in visualization. The fistula is either dissected out (removed) or laid open (incised) along its entire length. Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 255. 4 Wound care: Following surgery, the wound is packed with gauze to aid healing, and appropriate wound care instructions are provided. Anal Fissure: An anal fissure refers to a longitudinal tear or ulceration in the lining of the anal canal, typically near the anal opening. Causes: Trauma and increased pressure on the anal canal Passing large, hard stools that stretch and tear the anal lining. Persistent tightening of the anal sphincter muscles, often related to stress, anxiety, or chronic constipation. Childbirth trauma. Overuse of laxatives that can lead to diarrhea and irritation of the anal area. Manifestation: Severe pain during and after bowel movements. Burning or stinging sensation in the anal area. Bright red blood on the stool or toilet paper. Itching or discomfort around the anus. In some cases, a small skin tag (sentinel pile) may develop near the fissure. Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 256. Diagnostic Procedure: Physical Examination: Anoscopy: In some cases, an anoscope (a small instrument) may be used to visualize the inside of the anal canal and confirm the diagnosis. Medical Management: Conservative medical management is the first-line treatment for anal fissures and includes: Stool Softeners: To prevent straining and facilitate easier bowel movements. Fiber Supplements: Increasing fiber intake helps soften the stool and promote regular bowel movements. Increased Fluid Intake: Drinking plenty of water helps prevent constipation. Sitz Baths: Soaking the anal area in warm water several times a day to relieve pain and promote healing. Topical Medications: Over-the-counter or prescribed creams or ointments containing local anesthetics or vasodilators may be used to reduce pain and promote healing. Surgical Management: Lateral Internal Sphincterotomy: This procedure involves making a small incision in the internal anal sphincter muscle to relieve pressure and promote healing. Fissurectomy: In some cases, the fissure itself may be removed surgically. Advancement Flap: This procedure involves moving healthy tissue from the anal canal to cover the fissure and promote healing. Nursing Management for Anorectal abscess, anal fistula & anal fissure: Assessment Gather information about the client's medical history, including any previous diagnoses or treatments related to anal fistula, anal fissure, or anorectal abscess. 2 5 6 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 257. Conduct a thorough physical assessment, focusing on the anal and rectal area, noting any signs or symptoms such as pain, swelling, redness, discharge, or bleeding. Assess the client's bowel habits, including any difficulties with defecation, constipation, or diarrhea. Inquire about the client's pain level, description of pain, and any factors that aggravate or alleviate the pain. Assess the client's overall health status, including any underlying medical conditions, immunosuppression, or history of inflammatory bowel disease. Evaluate the client's emotional well-being, noting any anxiety or stress related to the condition. Diagnosis: Impaired tissue integrity related to the presence of anal fistula, anal fissure, or anorectal abscess. Acute or chronic pain related to the anal fistula, anal fissure, or anorectal abscess. Risk for infection related to the presence of anal fistula, anal fissure, or anorectal abscess. Disturbed body image related to the nature and location of the condition. Deficient knowledge regarding self-care measures and management of anal fistula, anal fissure, or anorectal abscess. Planning: Collaborate with the healthcare team to establish goals and expected outcomes, such as: Promote wound healing and tissue integrity. Manage pain effectively. Prevent infection and promote wound healing. Address emotional and psychosocial needs. Educate the client about self-care measures and management. Implementation: 2 5 7 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 258. Provide wound care and hygiene management, such as sitz baths, gentle cleansing of the affected area, and application of prescribed topical medications. Administer prescribed medications, including analgesics, stool softeners, antibiotics, or other medications as ordered. Collaborate with the healthcare team to arrange for surgical interventions, such as fistulectomy, sphincterotomy, or excision of abscess. Assist the client with pain management techniques, such as positioning, application of heat or cold packs, and relaxation techniques. Educate the client about dietary modifications, including increased fiber intake and adequate fluid intake to prevent constipation. Provide emotional support and counseling to address any body image concerns or emotional distress associated with the condition. Monitor and assess the client's wound healing, pain level, and signs of infection, reporting any changes or concerns to the healthcare provider. Teach the client about self-care measures, including wound care, medication administration, signs and symptoms of complications, and when to seek medical attention. Evaluation: Assess the client's progress toward achieving the established goals and expected outcomes. Determine the effectiveness of the implemented interventions in promoting wound healing, managing pain, preventing infection, addressing emotional needs, and enhancing the client's knowledge and self-care abilities. Modify the care plan as necessary based on the client's response to treatment and ongoing assessment. 2 5 8 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 259. Pancreatitis inflammation of the pancreas, which can be acute or chronic. It is often caused by obstruction of the pancreatic duct from gallstones or backflow of bile into the pancreatic duct. Acute Pancreatitis Acute pancreatitis can range from mild and self-limiting to severe and rapidly fatal. Mild acute pancreatitis is characterized by edema and inflammation confined to the pancreas, with minimal organ dysfunction. Return to normal usually occurs within 6 months for mild acute pancreatitis. The mortality rate for severe acute pancreatitis and its systemic complications can be 50% or higher. Chronic pancreatitis Chronic pancreatitis is characterized by progressive destruction of the pancreas, both structurally and functionally. Repeated attacks of pancreatitis lead to the replacement of pancreatic cells with fibrous tissue, causing an increase in pressure within the pancreas. 2 5 9 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 260. Etiology Self-digestion by its own proteolytic enzymes, mainly trypsin 5% of gallstone patients develop pancreatitis Long-term alcohol (60% CP) Other less common causes include o bacterial or viral infection (such as mumps), o spasm and edema of the ampulla of Vater, o blunt abdominal trauma, o peptic ulcer disease, o ischemic vascular disease, o hyperlipidemia, o hypercalcemia, and certain medications. after pancreatic surgery or instrumentation, in some cases, the cause may be idiopathic or hereditary. Manifestations: Severe abdominal Abdominal pain and tenderness, as well as back pain Typically, the pain is felt in the midepigastrium and may be diffuse and difficult to localize. Pain occur 24 to 48 hours after a heavy meal or alcohol consumption, and is worsened by meals and unrelieved by antacids. Abdominal distention, a poorly defined palpable abdominal mass, and decreased peristalsis may accompany the pain. Vomiting that does not relieve the pain or nausea is frequently present. Abdominal guarding and a rigid or board-like abdomen as ominous signs. Ecchymosis (bruising) in the flank or around the umbilicus may indicate severe pancreatitis. Nausea, vomiting, fever, jaundice, mental confusion, and agitation are common symptoms. Hypotension, tachycardia, cyanosis, cold and clammy skin, and acute renal failure may occur due to hypovolemia and shock caused by fluid loss into tissues and the peritoneal cavity. 2 6 0 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar Muhammad . e pancreas. eatitis. hest) may reduced p a i n
- 261. Respiratory distress, hypoxia, diffuse pulmonary infiltrates, dyspnea, tachypnea, abnormal blood gas values, myocardial depression, hypocalcemia, hyperglycemia, and disseminated intravascular coagulopathy (DIC) can also occur in acute pancreatitis. Panic attack even not relieved by opioids (CP). The frequency, duration, and severity of pain attacks increase (CP). Weight loss, malabsorption (CP). Steatorrhea (CP). Calcification of the pancreas (CP). Diagnostic Procedure: Patient's history of abdominal pain, presence of known risk factors, physical examination findings Serum amylase and lipase levels are commonly used in diagnosing acute pancreatitis. While not be significantly elevated in (CP). Elevated WBCs, and hypocalcemia Transient hyperglycemia, glucosuria, and elevated serum bilirubin levels may occur in some patients. X-ray studies may be performed to differentiate pancreatitis from other similar conditions and detect pleural effusions. Ultrasound and contrast-enhanced computed tomography (CT) scans are used to visualize the pancreas, identify an increase in its diameter, and detect pancreatic cysts, abscesses, or pseudocysts (AP & CP). Hematocrit and hemoglobin levels are monitored to assess for bleeding. Peritoneal fluid may be collected through paracentesis or peritoneal lavage to measure increased levels of pancreatic enzymes. Stool characteristics in patients with pancreatic disease often include bulky, pale, and foul-smelling stools with a higher fat content. (ERCP) is rarely used for (AP) while useful in (CP). A glucose tolerance test. In chronic pancreatitis, serum amylase levels and the white blood cell count may, unlike in acute pancreatitis. Medical management NPO: All oral intake is withheld to prevent pancreatic stimulation and secretion of pancreatic enzymes. 2 6 1 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 262. Parenteral nutrition: It is usually necessary, especially in debilitated patients, to provide adequate nutrition and manage the metabolic stress associated with acute pancreatitis. Nasogastric suction: Used to relieve nausea, vomiting, abdominal distention, and paralytic ileus. It also removes hydrochloric acid to prevent pancreatic stimulation. Histamine-2 (H2) antagonists: Prescribed to decrease pancreatic activity by inhibiting HCl secretion. Pain management: Adequate pain medication, such as meperidine (Demerol), is essential to provide pain relief and minimize restlessness. Morphine derivatives are often avoided due to concerns about sphincter of Oddi spasm. Antiemetic agents: Prescribed to prevent vomiting. Intensive care: Close monitoring in the intensive care unit is necessary. Fluid and blood loss correction and maintenance of adequate fluid volume are essential to prevent renal failure. Hemodynamic monitoring and arterial blood gas monitoring are initiated. Antibiotics may be prescribed if infection is present, and insulin may be required for hyperglycemia. Respiratory care: Aggressive respiratory care is needed due to the risk of diaphragm elevation, pulmonary infiltrates, effusion, and atelectasis. Close monitoring of arterial blood gases, humidified oxygen, and mechanical ventilation may be necessary. Biliary drainage: Placement of biliary drains and stents in the pancreatic duct through endoscopy can be performed to reestablish drainage of the pancreas, reducing pain and promoting weight gain. For Chronic Pancreatitis Endoscopy, performed in specialized centers, can be used to remove pancreatic duct stones and stent strictures, helping manage pain and relieve obstruction. Management of abdominal pain and discomfort focuses on nonopioid methods to control pain. Emphasizing the importance of avoiding alcohol and other trigger foods is crucial in managing pain and discomfort. 2 6 2 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 263. Diabetes mellitus resulting from pancreatic islet cell dysfunction is treated with diet, insulin, or oral antidiabetic agents. The risk of severe hypoglycemia with alcohol use should be highlighted. Pancreatic enzyme replacement therapy is indicated for patients with malabsorption and steatorrhea. Surgical Intervention: Diagnostic laparotomy: Surgery may be performed to assist in the diagnosis of pancreatitis. It involves making an incision in the abdomen to visually inspect the pancreas and surrounding structures. Pancreatic drainage: Surgery may be done to establish drainage of the pancreas. This is especially important if there is a pseudocyst or abscess present. Drains may be placed to facilitate the removal of fluid or infected material. Resection or débridement: In cases of severe necrotizing pancreatitis, surgical intervention may be required to remove or débride (clean) the necrotic pancreatic tissue. This is done to prevent the spread of infection and reduce complications. For Chronic Pancreatitis Pancreaticojejunostomy (Roux-en-Y) allows drainage of pancreatic secretions into the jejunum, providing pain relief in a majority of patients. Other surgical procedures may include revision of the sphincter of the ampulla of Vater, internal drainage of pancreatic cysts, insertion of stents, wide resection of the pancreas, or a Whipple resection (pancreaticoduodenectomy). Autotransplantation or implantation of pancreatic islet cells is attempted to preserve endocrine function after total pancreatectomy. Nursing Management: Assessment Obtain a detailed medical history, including any previous episodes of pancreatitis, alcohol consumption, gallstone disease, and other risk factors. 2 6 3 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 264. Assess the client's current symptoms, such as abdominal pain (location, intensity, duration), vomiting, fever, jaundice, weight loss, and changes in bowel movements. Monitor vital signs, including temperature, heart rate, blood pressure, and respiratory rate. Perform a thorough physical examination, focusing on abdominal tenderness, guarding, distension, and signs of systemic complications like respiratory distress or hypotension. Diagnosis Acute Pancreatitis: Acute pain related to pancreatic inflammation and edema. Risk for imbalanced fluid volume related to vomiting and potential hypovolemic shock. Risk for impaired skin integrity related to frequent vomiting and poor nutrition. Chronic Pancreatitis: Chronic pain related to recurrent inflammation and fibrosis. Imbalanced nutrition: less than body requirements related to anorexia, fear of eating, and malabsorption. Risk for impaired skin integrity related to malabsorption and impaired wound healing. Planning Acute Pancreatitis: Alleviate pain using nonopioid analgesics, positioning, and relaxation techniques. Administer intravenous fluids to maintain hydration and prevent shock. Monitor and manage electrolyte imbalances. Chronic Pancreatitis: Administer pancreatic enzyme replacement therapy (PERT) to aid digestion and manage malabsorption. 2 6 4 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 265. Promote a high-calorie, low-fat diet to meet nutritional needs and prevent weight loss. Educate the client about the importance of avoiding alcohol and trigger foods that exacerbate symptoms. Provide emotional support and counseling to help the client cope with chronic pain and lifestyle changes. Implementation Acute Pancreatitis: Administer prescribed pain medications and monitor their effectiveness. Monitor vital signs regularly and assess for signs of fluid imbalance or complications. Collaborate with the healthcare team to manage complications like respiratory distress or hypocalcemia. Provide clear liquids and progress to a low-fat diet as tolerated. Chronic Pancreatitis: Administer PERT with meals and snacks to aid digestion and absorption. Monitor the client's weight and nutritional status regularly. Educate the client on dietary modifications, such as consuming small, frequent meals and avoiding fatty foods. Encourage the client to adhere to the prescribed medication regimen and attend follow-up appointments. Evaluation Assess the client's response to pain management interventions and evaluate the effectiveness of pain relief. Monitor fluid balance and assess for improvements in hydration status. Evaluate the client's adherence to dietary modifications and assess for improvements in weight and nutritional status. Provide ongoing support and education to the client and evaluate their understanding and ability to manage their condition effectively. Collaborate with the healthcare team to monitor and manage any complications or exacerbations of the condition 2 6 5 Prepared by: Muhammad Ziad Lecturer INS-KMU Peshawar
- 266. Pancreatic Cancer Pancreatic cancer is a malignant disease that originates in the cells of the pancreas, an organ located in the abdomen. It is characterized by the uncontrolled growth of abnormal cells within the pancreas, leading to the formation of tumors. Pancreatic cancer can be classified into different types, with the most common form being pancreatic ductal adenocarcinoma. The location of the pancreas behind other organs makes it challenging for healthcare providers to visually or manually detect tumors during routine examinations. Due to late detection and rapid spread, pancreatic cancer is often challenging to treat effectively. Causes: No one knows the exact causes of pancreatic cancer. Studies have found the following risk factors: Age: over the age of 60. Smoking: three times higher risk Diabetes: Gender: More in men Ethnicity: African Americans have more Family history Chronic pancreatitis Certain chemicals in the workplace A diet high in fat may increase Manifestations: Pancreatic cancer is sometimes called a "silent disease". Pain in the upper abdomen or upper back Yellow skin and eyes, and dark urine from jaundice Weakness Loss of appetite Nausea and vomiting Weight loss 2 6 6 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 267. These symptoms are not sure signs of pancreatic cancer. Only a doctor can diagnose the cause of a person's symptoms. Diagnostic Procedures: Physical exam -- The doctor examines the skin and eyes for signs of jaundice. The doctor then feels the abdomen to check for changes in the area near the pancreas, liver, and gallbladder. The doctor also checks for ascites, an abnormal buildup of fluid in the abdomen. Lab tests -- The doctor may take blood, urine, and stool samples to check for bilirubin and other substances. CT scan (Computed tomography) Ultrasonography -- Transabdominal ultrasound: To make images of the pancreas, the doctor places the ultrasound device on the abdomen and slowly moves it around. EUS (Endoscopic ultrasound): ERCP (endoscopic retrograde cholangiopancreatography) – PTC (percutaneous transhepatic cholangiography) Biopsy Medical & Surgical Management: Resectable and localized tumors in the head of the pancreas may require extensive surgical procedures for removal. Definitive surgical treatment is often not possible due to extensive tumor growth and probable metastases. Palliative measures are commonly used for treatment in such cases. Radiation therapy and chemotherapy (fluorouracil and gemcitabine) may be considered, despite pancreatic tumors being resistant to standard radiation therapy. Intraoperative radiation therapy (IORT) may be utilized during surgery to deliver a high dose of radiation to the tumor while minimizing damage to surrounding tissues. IORT can also help alleviate pain. Interstitial implantation of radioactive sources has been used, but it carries a high rate of complications. A largebiliary stent may be inserted percutaneously or through endoscopy to relieve jaundice. 2 6 7 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 268. Nursing Management: Assessment (A): Gather comprehensive information about the client's medical history, including previous diagnoses, treatments, and surgeries related to pancreatic carcinoma. Perform a thorough physical assessment, focusing on signs and symptoms of the disease, such as jaundice, weight loss, anorexia, and abdominal pain. Assess the client's pain level using a standardized pain assessment tool. Evaluate the client's nutritional status and assess any nutritional deficiencies or challenges. Assess the client's emotional and psychological well-being, including their coping mechanisms and support systems. Diagnosis (D): Pain related to pancreatic carcinoma and associated symptoms. Imbalanced nutrition: less than body requirements related to anorexia and weight loss. Impaired skin integrity related to prolonged jaundice and potential complications. Anxiety and fear related to the diagnosis and prognosis of pancreatic carcinoma. Planning (P): 2 6 8 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 269. 4 Collaborate with the healthcare team to develop an individualized care plan based on the client's specific needs and preferences. Set goals and expected outcomes in collaboration with the client and their family, aiming to manage pain, improve nutritional intake, maintain skin integrity, and address emotional well-being. Identify appropriate interventions and treatments to achieve the established goals, such as pain management strategies, nutritional counseling, skin care protocols, and psychosocial support. Implementation (I): Administer prescribed pain medications as per the client's pain management plan, monitoring for effectiveness and side effects. Collaborate with a dietitian to develop a personalized nutrition plan that addresses the client's nutritional needs, preferences, and any dietary restrictions. Implement measures to promote skin integrity, including regular assessment, turning and repositioning, and providing appropriate skin care products. Provide emotional support and counseling to address anxiety and fears related to the diagnosis and prognosis. Encourage the involvement of support groups or counseling services. Evaluation (E): Continuously monitor and reassess the client's pain levels and adjust pain management interventions accordingly. Regularly evaluate the client's nutritional status and make modifications to the nutrition plan as needed. Assess the client's skin condition for any signs of breakdown or improvement and modify interventions accordingly. Monitor the client's emotional well-being and assess their coping mechanisms to determine the effectiveness of the psychosocial support provided. P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 270. 5 Pancreatic cysts A pancreatic pseudocyst is a collection of fluid enclosed by a fibrous wall, which develops as a complication of acute pancreatitis or pancreatic trauma. It is termed a "pseudocyst" because it lacks an epithelial lining, unlike true cysts. Pancreatic abscess, on the other hand, is a localized collection of pus within or near the pancreas. Causes: Most commonly acute pancreatitis. Also occur as a result of chronic pancreatitis, pancreatic trauma (such as injury or surgery), or as a complication of pancreatic duct obstruction or leakage. Pathophysiology & Manifestations: During acute pancreatitis, inflammation and necrosis of pancreatic tissue can lead to the formation of pseudocysts. These pseudocysts usually develop within 4-6 weeks after the initial insult. They can grow in size and cause compression on surrounding structures, leading to symptoms such as abdominal pain, nausea, vomiting, early satiety, and weight loss. In some cases, a pancreatic pseudocyst can become infected, resulting in a pancreatic abscess. Infection can occur through the spread of bacteria from the gastrointestinal tract or hematogenous dissemination. Diagnostic Procedure: Endoscopic Ultrasound (EUS), computed tomography (CT), MRI and (ERCP). P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 271. Blood tests i-e CBC, LFTs, C-reactive protien Medical Management: Observation and supportive care: Small, asymptomatic pseudocysts may resolve spontaneously and require only observation and supportive measures such as pain management, nutritional support, and close monitoring. Antibiotics: If infection is suspected or confirmed in a pseudocyst or abscess, broad-spectrum antibiotics are administered to cover common pathogens until culture results are available. Percutaneous Drainage: Image-guided percutaneous drainage is a minimally invasive procedure where a catheter is inserted into the pseudocyst or abscess under imaging guidance to drain the fluid and relieve symptoms. This is typically performed when the pseudocyst is symptomatic or infected. Surgical Management: Internal Drainage: Surgical internal drainage is considered for large, symptomatic pseudocysts or those that fail percutaneous drainage. It involves creating a communication between the pseudocyst and the gastrointestinal tract (cystogastrostomy or cystojejunostomy) to allow drainage of the fluid. Pancreatic Necrosectomy: In severe cases of infected pancreatic necrosis or abscess, surgical removal of the necrotic tissue (necrosectomy) may be necessary. Distal Pancreatectomy: In some situations, if the pseudocyst or abscess is located in the tail of the pancreas, surgical removal of the distal portion of the pancreas (distal pancreatectomy) may be performed. 2 7 1 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 272. Nursing Management: Assessment: Gather comprehensive data about the client's medical history, including any previous episodes of pancreatitis or pancreatic trauma. Assess the client's current symptoms, such as abdominal pain, nausea, vomiting, weight loss, and signs of infection. Perform a physical examination to assess the abdomen for distension, tenderness, and presence of a palpable mass. Monitor vital signs, laboratory values (including amylase levels), and imaging reports (ultrasound, CT scan) to obtain a clear understanding of the client's condition. Assess the client's emotional and psychosocial well-being, as a pancreatic pseudocyst/abscess can be distressing and impact their quality of life. Diagnosis: Risk for Infection related to pancreatic pseudocyst/abscess. Acute Pain related to inflammation and compression caused by the pseudocyst/abscess. Imbalanced Nutrition: Less Than Body Requirements related to anorexia, early satiety, and weight loss. Anxiety related to the diagnosis, uncertainty, and potential complications. Planning: Establish goals and outcomes in collaboration with the client and healthcare team, such as: The client will remain free from signs and symptoms of infection. The client will experience effective pain management. The client's nutritional status will be improved and maintained. The client will demonstrate reduced anxiety and increased coping mechanisms. Intervention: 2 7 2 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 273. Monitor vital signs regularly, paying attention to signs of infection (e.g., fever, elevated white blood cell count) or deterioration in the client's condition. Administer prescribed analgesics and assess pain relief. Use a pain scale to monitor the client's pain level and adjust pain management strategies accordingly. Collaborate with the healthcare team to provide nutritional support, including consulting with a dietitian to develop a tailored dietary plan that meets the client's needs. Implement measures to reduce anxiety, such as providing emotional support, educating the client about the condition and treatment, and involving them in the decision-making process. Educate the client and their family about signs of infection, the importance of adhering to prescribed medications, and the need for follow-up appointments. Evaluation: Continuously assess the client's response to interventions, including pain relief, signs of infection, nutritional status, and psychological well- being. Evaluate whether the client's goals and outcomes have been met or if modifications to the care plan are necessary. Collaborate with the healthcare team to determine the next steps in managing the client's pancreatic pseudocyst/abscess, which may include further interventions, follow-up imaging, or referral to a specialist if needed. Provide ongoing support and education to the client and their family to promote self-care and understanding of the condition. 2 7 3 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 274. Hepatic abscess A hepatic abscess is a localized collection of pus within the liver parenchyma. It is usually caused by a bacterial infection and can lead to significant liver dysfunction if not treated promptly. Causes: The most common cause of hepatic abscess is bacterial infection, typically resulting from: Biliary tract infection: Spread of infection from the biliary system, such as in cases of cholecystitis or cholangitis. Portal vein sepsis: Infection spreads from the gastrointestinal tract via the portal vein. Direct extension: Infection spreads from nearby organs, such as the appendix or colon. Systemic infection: Bacteria can disseminate through the bloodstream to the liver, often seen in cases of endocarditis or intra-abdominal infections. Pathophysiology and Manifestations: Infection: Bacteria gain entry to the liver and cause an inflammatory response, leading to abscess formation. Abscess development: Pus accumulates within the liver, forming a cavity. Symptoms: Manifestations may include fever, abdominal pain, hepatomegaly (enlarged liver), weight loss, jaundice, and general signs of infection such as fatigue and malaise. Diagnostic Procedures: Imaging: Abdominal ultrasound, computed tomography (CT) scan, or magnetic resonance imaging (MRI) can identify the presence and location of the abscess. 2 7 4 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 275. Blood tests: Complete blood count (CBC) may show elevated white blood cell count, while liver function tests may reveal abnormal liver enzymes. Medical Management: Antibiotic therapy: Broad-spectrum antibiotics are usually prescribed to cover a wide range of bacteria until the specific pathogen is identified. Percutaneous drainage: A procedure in which a needle or catheter is inserted into the abscess to drain the pus and relieve symptoms. Supportive care: Intravenous fluids, pain management, and management of complications such as sepsis or liver failure. Surgical Management: Surgical drainage: In cases where percutaneous drainage is not possible or unsuccessful, open surgical drainage may be necessary to remove the abscess. Abscess resection: In some cases, a portion of the liver containing the abscess may need to be surgically removed. Nursing Management: Assessment: Gather comprehensive medical history and assess current symptoms of the client with hepatic abscess, including fever, abdominal pain, hepatomegaly, and signs of infection. Perform physical examination and monitor vital signs. Review diagnostic reports such as ultrasound, CT scan, and blood tests. Diagnosis: Risk for Infection related to hepatic abscess. Acute Pain related to inflammation and pressure within the liver. Imbalanced Nutrition: Less Than Body Requirements related to anorexia and weight loss. Impaired Physical Mobility related to abdominal pain and discomfort. 2 7 5 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 276. Planning: Collaborate with the client and healthcare team to establish goals and outcomes. Intervention: Monitor vital signs regularly and assess for signs of infection or deterioration in the client's condition. Administer prescribed antibiotics and assess the effectiveness of the treatment. Administer prescribed analgesics and assess pain relief. Collaborate with the healthcare team to provide nutritional support and consult with a dietitian to develop a tailored dietary plan. Assist the client in finding comfortable positions and provide measures to alleviate abdominal pain. Provide education and support to the client and family regarding the management of hepatic abscess, including medication adherence and the importance of follow-up appointments. Evaluation: Continuously assess the client's response to interventions, including pain relief, signs of infection, nutritional status, and physical mobility. Evaluate whether the client's goals and outcomes have been met or if modifications to the care plan are necessary. Collaborate with the healthcare team to determine the next steps in managing the client's hepatic abscess, which may include further interventions or surgical management if needed. Provide ongoing support and education to the client and their family to promote self-care and understanding of the condition. 2 7 6 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 277. Cancer of the liver Cancer of the liver, specifically hepatocellular carcinoma (HCC), is the most common type of primary liver cancer. It is typically associated with chronic liver disease, such as cirrhosis, hepatitis B and C infections, and exposure to certain toxins. Other types of primary liver cancer include cholangiocellular carcinoma and combined hepatocellular and cholangiocellular carcinoma. Pathophysiology involves the uncontrolled growth of malignant cells in the liver tissue. Chronic liver disease and inflammation contribute to genetic mutations and abnormal cell proliferation, leading to the formation of tumors. These tumors can grow rapidly and metastasize to other organs. Manifestations pain in the right upper quadrant or epigastrium, weight loss, anorexia, anemia, hepatomegaly, and jaundice (if larger bile ducts are occluded). Ascites may also develop if tumor nodules obstruct the portal veins or spread to the peritoneal cavity. Diagnostic procedures clinical assessment, physical examination, laboratory tests (elevated liver enzymes, alpha-fetoprotein levels), 2 7 7 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 278. imaging studies (x-rays, liver scans, CT scans, ultrasound, MRI), and biopsy to confirm the tumor's histology. 2 7 8 P r e p a r e d b y : M u h a m m a d Z i a d L e c Medical management includes surgical resection of the tumor if possible, but this is often limited due to underlying cirrhosis. Radiation therapy, including external beam radiation or targeted radiation therapy using radioactive isotopes, may be used. Chemotherapy is also employed to improve quality of life and prolong survival, either systemically or through regional infusion. Percutaneous biliary drainage may be performed to bypass biliary ducts obstructed by tumors. Laser hyperthermia has been used to treat hepatic metastases. Immunotherapy i-e lymphocytes with antitumor reactivity are administered to the patient with hepatic cancer. Transcatheter arterial embolization (block blood flow) Ultrasound-guided injection of alcohol (cause dehydration of tumor) Surgical Management: Surgical resection is the treatment of choice when HCC is confined to one lobe of the liver and the function of the remaining liver is considered adequate for postoperative recovery. Lobectomy Cryosurgery Liver Transplantation. Nursing Management: Assessment: Gather comprehensive data about the client's medical history, including the presence of chronic liver disease, hepatitis B or C infections, exposure to toxins, and any previous treatments for liver cancer.
- 279. Assess the client's current symptoms, such as pain in the right upper quadrant, weight loss, anorexia, jaundice, and signs of liver dysfunction. Perform a physical examination to assess the abdomen for hepatomegaly, ascites, and any surgical incisions or drainage tubes. Monitor vital signs, laboratory values (liver function tests, tumor markers), and imaging reports to obtain a clear understanding of the client's condition. Assess the client's emotional and psychosocial well-being, as a diagnosis of liver cancer can be distressing and impact their quality of life. Diagnosis: Acute Pain related to surgical incisions, tumor growth, and invasive procedures. Imbalanced Nutrition: Less Than Body Requirements related to anorexia, weight loss, and metabolic abnormalities. Risk for Infection related to impaired immune function and potential surgical complications. Anxiety related to the diagnosis, treatment procedures, and uncertainty about the future. Planning: Collaborate with the healthcare team to establish goals and outcomes, such as effective pain management, improved nutritional status, prevention of infection, and reduced anxiety. Involve the client and their family in the care planning process to ensure their participation and understanding of the treatment plan. Intervention: Administer analgesics, monitor nutrition, prevent infection, provide emotional support and education, and teach about medication adherence and symptom recognition. After surgery for liver cancer, closely monitor the patient for potential complications such as vascular complications, respiratory dysfunction, and liver dysfunction. 2 7 9 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 280. Pay attention to metabolic abnormalities and consider a constant infusion of 10% glucose in the first 48 hours to prevent a sudden drop in blood glucose levels. Due to possible extensive blood loss, administer blood transfusions and intravenous fluids as necessary. Provide constant and close monitoring and care for the patient during the first 2 or 3 days, similar to postsurgical care for abdominal and thoracic surgeries. For patients undergoing cryosurgery, closely monitor for hypothermia, hemorrhage, or bile leak. Take measures to minimize myoglobinuria, such as hydration, diuresis, and possibly medications like allopurinol. If the patient is receiving chemotherapy or radiation therapy for symptom relief, consider the possibility of discharging them home while still undergoing these treatments. Patients may have a biliary drainage system in place when discharged home. Provide extensive teaching to ensure the patient's active participation in their care and educate the family on their role in home care. Evaluation: Continuously assess the client's response to interventions, including pain relief, nutritional status, prevention of infection, and psychological well-being. Evaluate whether the client's goals and outcomes have been met or if modifications to the care plan are necessary. Collaborate with the healthcare team to determine the next steps in managing the client's liver cancer, which may include further treatments, palliative care, or referral to supportive services. Provide ongoing support and education to the client and their family to promote self-care, coping mechanisms, and understanding of the disease and treatment options. 2 8 0 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 281. Cirrhosis of the liver a chronic disease characterized by the replacement of normal liver tissue with diffuse fibrosis, leading to disruption of liver structure and function. There are three main types of cirrhosis: Alcoholic cirrhosis: This is the most common type and is caused by chronic alcoholism and excessive alcohol consumption over a prolonged period. Postnecrotic cirrhosis: It occurs as a late result of a previous episode of acute viral hepatitis. Broad bands of scar tissue develop in the liver as a result. Biliary cirrhosis: This type is less common and is associated with chronic biliary obstruction and infection (cholangitis) that leads to scarring around the bile ducts. Causes: The main causes of cirrhosis include chronic alcohol abuse, chronic viral hepatitis (such as hepatitis B and C), 2 8 1 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 282. non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH), autoimmune hepatitis, genetic and inherited liver diseases, chronic bile duct diseases, as well as certain medications, toxins, and other factors. Other factors that can contribute to cirrhosis include exposure to certain chemicals (such as carbon tetrachloride), chronic infection with schistosomiasis, and certain genetic disorders. Pathophysiology: In cirrhosis, the liver undergoes progressive fibrosis, leading to disruption of its normal architecture. The scar tissue replaces healthy liver cells and affects the functioning of the liver. The areas primarily involved in cirrhosis are the portal and periportal spaces, where inflammation occurs, bile ducts become blocked, and new bile channels form surrounded by scar tissue. Manifestations: Intermittent jaundice (yellowing of the skin and eyes) and fever. Enlarged liver initially, which later becomes small and nodular due to the development of scar tissue. Portal hypertension leading to complications such as ascites (fluid accumulation in the abdomen), splenomegaly (enlarged spleen), and the development of gastrointestinal varices (enlarged blood vessels) that can rupture and cause bleeding. Edema, particularly in the lower extremities. Vitamin deficiencies, anemia, and poor nutritional status. 2 8 2 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 283. Mental deterioration and hepatic encephalopathy. Diagnostic Evaluation: Liver function tests: Measure levels of enzymes, bilirubin, albumin, and clotting factors. Imaging studies: Ultrasound, CT scan, MRI, and radioisotope liver scans provide information about liver size, blood flow, and obstruction. Liver biopsy: A tissue sample is obtained for examination to confirm the diagnosis and assess the extent of liver damage. Arterial blood gas analysis: May reveal ventilation-perfusion imbalances and hypoxia. Medical Management: Medications may be prescribed to relieve gastric distress and minimize the risk of gastrointestinal bleeding. Vitamins and nutritional supplements can help improve the patient's nutritional status. Diuretics: Potassium-sparing diuretics may be used to reduce ascites. Dietary modifications: A well-balanced diet is important, and alcohol consumption must be avoided. Colchicine: Preliminary studies suggest that colchicine, an anti- inflammatory agent, may improve survival in patients with mild to moderate cirrhosis by reversing fibrotic processes. Surgical Management: In advanced cases of cirrhosis, liver transplantation may be considered as a definitive treatment option. This involves replacing the damaged liver with a healthy liver from a donor. Nursing Management: Assessment (A): Obtain a detailed medical history, including information about alcohol consumption, viral hepatitis, and other potential causes of cirrhosis. Assess the client's current symptoms, such as jaundice, fatigue, abdominal pain, and fluid retention. 3 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 284. Monitor vital signs, including blood pressure, heart rate, and respiratory rate. Perform a physical examination, paying particular attention to signs of liver dysfunction, such as an enlarged liver, abdominal distension, and peripheral edema. Conduct laboratory tests, including liver function tests, complete blood count, coagulation profile, and viral hepatitis screening. Assess the client's nutritional status and dietary intake. Diagnosis (D): Impaired liver function related to cirrhosis as evidenced by abnormal liver function tests and clinical manifestations. Risk for fluid volume excess related to compromised liver function and fluid retention. Activity intolerance related to fatigue and decreased energy levels. Knowledge deficit regarding disease process, treatment, and self-care management. Planning (P): Collaborate with the healthcare team to develop an individualized care plan. Set goals and outcomes that are realistic and measurable, focusing on symptom management, prevention of complications, and client education. Prioritize interventions based on the client's immediate needs and potential risks. Ensure the availability of necessary resources and equipment for the planned interventions. Implementation (I): Monitor vital signs, including blood pressure, heart rate, and respiratory rate, to detect any changes indicating worsening liver function. Administer medications as prescribed, such as diuretics for fluid management and medications to support liver function. Provide a balanced diet with appropriate modifications, including a low- sodium diet and adequate protein intake. 2 8 4 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 285. Educate the client and their family about the importance of abstaining from alcohol and maintaining a healthy lifestyle. Assist with activities of daily living and encourage periods of rest to manage fatigue and conserve energy. Monitor and manage complications such as ascites, gastrointestinal bleeding, and hepatic encephalopathy. Provide emotional support and counseling to the client and their family, addressing their concerns and coping strategies. Evaluation (E): Regularly assess the client's response to interventions, including symptom improvement, stabilization of liver function, and prevention of complications. Review laboratory results to determine if liver function tests are within the desired range. Evaluate the client's understanding of the disease process and self-care management through verbalization and demonstration. Modify the care plan as necessary based on the client's progress and changing needs. Collaborate with the healthcare team and involve the client in decision- making regarding ongoing care and future treatment options. 2 8 5 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 286. CHOLELITHIASIS Overview Gallstones are small, pebble-like substances that develop in the gallbladder. The gallbladder is a small, pear-shaped sac located below your liver in the right upper abdomen. Gallstones form when liquid stored in the gallbladder hardens into pieces of stone-like material. The two types of gallstones are cholesterol stones and pigment stones. Cholesterol stones are usually yellow-green and are made primarily of hardened cholesterol. They account for about 80 percent of gallstones. Pigment stones are small, dark stones made of bilirubin. Gallstones can be as small as a grain of sand or as large as a golf ball. The gallbladder can develop just one large stone, hundreds of tiny stones, or a combination of the two. Symptoms: gallbladder “attack Steady pain in the right upper abdomen that increases rapidly and lasts from 30 minutes to several hours Pain in the back between the shoulder blades Pain under the right shoulder Notify your doctor if you think you have experienced a gallbladder attack. Although these attacks often pass as gallstones move, your gallbladder can become infected and rupture if a blockage remains. People with any of the following symptoms should see a doctor immediately: Prolonged pain—more than 5 hours Nausea and vomiting Fever—even low-grade—or chills Yellowish color of the skin or whites of the eyes Clay-colored stools 2 8 6 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 287. Many people with gallstones have no symptoms; these gallstones are called “silent stones.” Highest risk: Women—especially women who are pregnant, use hormone replacement therapy, or take birth control pills People over age 60 American Indians Mexican Americans Overweight or obese men and women People who fast or lose a lot of weight quickly People with a family history of gallstones People with diabetes People who take cholesterol-lowering drugs Diagnostic Procedure: Ultrasound exam—the most sensitive and specific test for gallstones. Computerized tomography (CT) scan. Cholescintigraphy (HIDA scan). The patient is injected with a small amount of nonharmful radioactive material that is absorbed by the gallbladder, which is then stimulated to contract. The test is used to diagnose abnormal contraction of the gallbladder or obstruction of the bile ducts. Endoscopic retrograde cholangiopancreatography (ERCP). Blood tests. Blood tests may be performed to look for signs of infection, obstruction, pancreatitis, or jaundice. Medical Treatment: Nonsurgical approaches are used only in special situations—such as when a patient has a serious medical condition preventing surgery— and only for cholesterol stones. Stones commonly recur within 5 years in patients treated non-surgically. Oral dissolution therapy. Drugs made from bile acid are used to dissolve gallstones. The drugs ursodiol (Actigall) and chenodiol (Chenix) work best for small cholesterol stones. Months or years of treatment may be necessary before all the stones dissolve. Both 2 8 7 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 288. Prepared by: Muhammad Ziad Lectu 8 rer INS-KMU Peshawar drugs may cause mild diarrhea, and chenodiol may temporarily raise levels of blood cholesterol and the liver enzyme transaminase. Contact dissolution therapy. This experimental procedure involves injecting a drug directly into the gallbladder to dissolve cholesterol stones. The drug—methyl tert-butyl ether—can dissolve some stones in 1 to 3 days, but it causes irritation and some complications have been reported. The procedure is being tested in symptomatic patients with small stones. Medications to avoid Fenofibrate Gemfibrozil Surgical Management: Cholecystectomy Nearly all cholecystectomies are performed with laparoscopy. If gallstones are present in the bile ducts, the physician—usually a gastroenterologist—may use endoscopic retrograde cholangiopancreatography (ERCP) to locate and remove them before or during gallbladder surgery. Occasionally, a person who has had a cholecystectomy is diagnosed with a gallstone in the bile ducts weeks, months, or even years after the surgery. The ERCP procedure is usually successful in removing the stone in these cases.
- 289. CHOLECYSTITIS refers to the inflammation of the gallbladder, which can be caused by various factors such as gallstones (calculous cholecystitis) or other conditions that obstruct the flow of bile, as well as in the absence of gallstones (acalculous cholecystitis). Causes: Calculous Cholecystitis: This is the most common form of cholecystitis and occurs when a gallstone obstructs the cystic duct, leading to bile accumulation in the gallbladder. Common risk factors in the development of calculous cholecystitis (cholelithiasis) include female gender, increasing age, obesity, pregnancy, family history, genetic factors, and oral contraceptive use. Acalculous Cholecystitis: This form of cholecystitis occurs without gallstones and is often associated with conditions such as major surgeries, severe trauma, burns, cystic duct obstruction, torsion, primary bacterial infections, and multiple blood transfusions. Common risk factors in the development of acalculous cholecystitis include AIDS, diabetes mellitus, major surgery, burns, sepsis, and long term total parenteral nutrition use Pathophysiology: In calculous cholecystitis, o a gallstone obstructs the cystic duct, preventing the normal flow of bile. o The trapped bile initiates a chemical reaction, causing autolysis and edema in the gallbladder wall. o This leads to compression of blood vessels in the gallbladder, compromising its blood supply. o If left untreated, gangrene and perforation of the gallbladder can occur. o Secondary bacterial infection may also develop. 2 8 9 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 290. Acalculous cholecystitis is thought to result from a combination of factors, o including alterations in fluid and electrolyte balance, changes in regional blood flow, bile stasis (reduced gallbladder contraction), and increased viscosity of bile. Manifestations: Severe pain, tenderness, and rigidity in the upper right abdomen, which may radiate to the midsternal area or right shoulder. Nausea and vomiting. Fever and chills. Jaundice (in severe cases or if there is common bile duct obstruction). Murphy's sign: Pain worsens upon deep inspiration while the examiner palpates the right upper quadrant. Diagnostic Approaches: Medical History and Physical Examination: The characteristic symptoms and signs, as well as risk factors, can provide important diagnostic clues. Laboratory Tests: Blood tests may show elevated levels of white blood cells, bilirubin, liver enzymes, and inflammatory markers. Imaging Studies: Ultrasonography is usually the initial imaging modality of choice to visualize gallstones, gallbladder wall thickening, or signs of inflammation. Other imaging techniques such as CT scan, MRI, or hepatobiliary scintigraphy (HIDA scan) may be used in specific cases. Medical Management: Pain Management: Analgesics are used to alleviate pain. Antibiotics: Broad-spectrum antibiotics are prescribed to treat or prevent infection. NPO (nothing by mouth) Status: Oral intake is withheld to rest the gallbladder and reduce stimulation of bile secretion. Intravenous Fluids: Fluids are administered to maintain hydration and electrolyte balance. 2 9 0 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 291. Surgical Management: Cholecystectomy: Surgical removal of the gallbladder is the definitive treatment for acute and chronic cholecystitis. It can be performed laparoscopically (minimally invasive) or through an open approach. Percutaneous Cholecystostomy: In critically ill patients or those with high surgical risks, a tube is inserted through the skin and into the gallbladder to drain the infected fluid. Nursing Management for Cholecystitis and Cholelithiasis Assessment: Gather comprehensive data about the client's health status, medical history, and symptoms related to Cholecystitis and Cholelithiasis. Assess vital signs, pain levels, and any signs of complications such as jaundice, fever, or abdominal distension. Conduct a thorough physical examination, including an abdominal assessment and assessment of bowel sounds. Review laboratory results, including liver function tests and imaging studies such as ultrasound or CT scan. Diagnosis: Analyze the assessment data to identify actual and potential nursing diagnoses specific to the client's condition. Examples of nursing diagnoses for Cholecystitis and Cholelithiasis may include: Acute Pain related to gallbladder inflammation and presence of gallstones. Risk for Infection related to biliary obstruction or surgical interventions. Imbalanced Nutrition: Less than Body Requirements related to impaired digestion and fat malabsorption. Planning: Set measurable and achievable goals in collaboration with the client. Develop a comprehensive care plan to address the identified nursing diagnoses and prioritize the client's needs. 2 9 1 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 292. Establish interventions that promote pain management, infection prevention, nutritional support, and patient education regarding the condition, treatment options, and lifestyle modifications. Coordinate with the interdisciplinary healthcare team for surgical interventions or other necessary medical treatments. Implementation: Execute the planned interventions based on the established care plan. Administer prescribed medications, including analgesics, antibiotics, and other medications to manage symptoms and prevent complications. Provide physical and emotional support; allow the patient to verbalize his feelings about the condition, and discuss appropriate coping strategies Preoperative nursing interventions ◆Monitor the patient for abdominal pain in the right upper quadrant that may radiate to the right shoulder ◆ Check the skin and conjunctivae for jaundice Postoperative nursing interventions ◆Monitor vital signs every 1 to 2 hours for 4 to 8 hours and then every 4 hours to detect fl uid imbalances, hemorrhage, or shock ◆Monitor bowel sounds every 4 hours and bowel output to determine return of GI functions ◆ Check the wound area for signs of bleeding and inflammation ◆Change the wound dressing as needed; the wound may be left uncovered if no drainage is present ◆Monitor drainage from the T tube, if present; a T tube is used if gallstones were in the common bile duct because it lets bile pass into the small intestine and decreases duct inflammation ◆Administer an opioid analgesic every 4 hours as needed and I.V. antibiotics every 6 to 8 hours as prescribed to maintain comfort and prevent infection 2 9 2 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 293. ◆Make sure the patient maintains nothing-by-mouth status as prescribed; administer I.V. fl uids (up to 3,000 mL daily) to maintain fl uid balance, also monitor fl uid intake and output every 8 hours ◆Start giving the patient clear liquids, then progress to a regular diet as prescribed; fat restrictions may be lifted because gallbladder removal increases the patient’s tolerance to fatty foods ◆Help the patient sit on the bed or in a chair and ambulate as prescribed to promote recovery from the surgery ◆ Record pertinent data in the patient’s chart for continuity of care Evaluation: Assess the effectiveness of the implemented interventions in achieving the established goals. Monitor the client's progress and evaluate changes in pain levels, infection status, nutritional status, and overall well-being. Modify the care plan as needed based on the client's response and any new developments. Continuously communicate with the client, their family, and the healthcare team to ensure coordinated care and address any concerns or questions. 2 9 3 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 294. Gallbladder cancer Gallbladder cancer is relatively rare and often difficult to diagnose in its early stages. It tends to be aggressive and has a poor prognosis. The main types of gallbladder cancer are adenocarcinoma (most common) and squamous cell carcinoma. Causes: The exact cause of gallbladder cancer is unclear, but several risk factors have been identified: Gallstones: Chronic inflammation: Gender: more common in women Age: over the age of 60. Ethnicity: Native Americans, Hispanics, and individuals from South Asia Obesity Pathophysiology The pathophysiology of gallbladder cancer involves the growth of malignant cells within the gallbladder's tissues. These cancer cells can invade nearby structures, such as the liver or bile ducts, and spread to distant organs (metastasis). Manifestations: Abdominal pain, particularly in the upper right quadrant or epigastric region. Jaundice (yellowing of the skin and eyes) due to obstruction of the bile ducts by the tumor. Unexplained weight loss and loss of appetite. Nausea, vomiting, and digestive disturbances. Abdominal mass or palpable lump. Bloating, indigestion, and discomfort. 2 9 4 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 295. Fever, chills, and signs of infection if the bile ducts become blocked or infected. Enlarged liver (hepatomegaly) or ascites (accumulation of fluid in the abdominal cavity) in advanced stages. Diagnostic Methods: To diagnose gallbladder cancer, various tests and procedures may be used, including: Imaging studies: Ultrasound, CT scan, MRI, or PET scan to visualize the gallbladder and surrounding structures. Blood tests: Liver function tests, tumor markers (such as CA 19-9), and complete blood count to assess overall health and detect any abnormalities. Biopsy: Tissue samples may be obtained through fine-needle aspiration, endoscopic procedures (such as ERCP or EUS), or during surgery to confirm the presence of cancer and determine its type. Medical and Surgical Management: The management of gallbladder cancer depends on the stage of the disease and the individual's overall health. Treatment options may include: Surgery: The primary treatment for early-stage gallbladder cancer involves removing the gallbladder (cholecystectomy) and potentially nearby lymph nodes. In more advanced cases, surgical resection of affected liver segments or bile ducts may be necessary. Chemotherapy: Systemic chemotherapy drugs may be used before or after surgery to kill cancer cells, shrink tumors, or manage symptoms. Radiation therapy: High-energy radiation is used to destroy cancer cells and may be given before or after surgery, or as palliative treatment to relieve symptoms. Palliative care: In cases where the cancer is advanced and curative treatment is not possible, palliative care focuses on symptom management, pain relief, and improving quality of life. 2 9 5 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 296. Nursing Management: Assessment: Collect comprehensive data about the client's medical history, including previous surgeries, presence of risk factors, and symptoms related to gallbladder cancer. Perform a physical examination to assess the client's general health status, including vital signs, abdominal assessment, and any signs of jaundice or weight loss. Conduct a psychosocial assessment to evaluate the client's emotional well-being and their support system. Gather relevant diagnostic test results, such as imaging studies and laboratory tests. Diagnosis: Acute Pain related to tumor invasion and inflammation. Imbalanced Nutrition: Less Than Body Requirements related to anorexia, nausea, and weight loss. Risk for Infection related to impaired immune system and invasive procedures. Planning: Establish goals and expected outcomes in collaboration with the client, focusing on addressing the identified nursing diagnoses. Develop a comprehensive care plan that includes interventions aimed at managing pain, maintaining nutrition, preventing complications, and supporting the client emotionally. Implementation: Administer prescribed medications for pain management, nausea control, and other symptoms as needed. Collaborate with the healthcare team to provide appropriate nutrition and dietary counseling, considering the client's specific needs and restrictions. Educate the client and their family about the disease process, treatment options, and potential side effects. 2 9 6 P r e p a r e d b y : M u h a m m a d Z i a d L e c
- 297. Assist in coordinating and facilitating referrals to supportive services, such as oncology specialists, palliative care, or social services. Provide emotional support and establish a therapeutic relationship to address the client's fears, anxiety, and coping mechanisms. Evaluation: Regularly assess the client's response to interventions and treatments, including pain level, nutritional status, and emotional well-being. Modify the care plan as necessary based on the client's changing needs or treatment outcomes. Collaborate with the healthcare team to monitor the effectiveness of cancer treatment and adjust interventions accordingly. Continuously evaluate the client's understanding of their condition and their ability to manage symptoms and make informed decisions. 2 9 7 P r e p a r e d b y : M u h a m m a d Z i a d L e c