prostate ca 5.pptx RADIATION ONCOLOGY PROSTATE CARCINOMA
1. HOMI BHABHA CANCER HOSPITAL, SANGRUR
(A Unit of TATA MEMORIAL CENTRE, Mumbai)
C A NC E R I S C U R AB L E I F D E T E C T
ED E AR L Y
Address :- HBCH, Civil Hospital Campus , Sangrur (Punjab) -148001
Contact No.:- 01672-223910
2. SBRT in Prostate cancer
Guideline and Evidences
Prof. Rakesh Kapoor
Director
HBCH, Mullanpur and Sangrur,
Punjab
ACKNOWLEGEMENTS
Dr. Abhijit Das (Asst. Prof) HBCH,MULLANPUR & SANGRUR
Dr. Priyamveda Maitre (Asst. Prof)
HBCH,MULLANPUR&SANGRUR
3. Taking Advantage of Alpha by beta for prostate
Radiobiology
• Reported first by David Brenner and Eric j Hall in 1999
• Alpha by beta: Relationship between cellular proliferative status
and sensitivity to changes in fractionation
• Prostatic tumours contain exceptionally low proportions of
proliferating cells. Proliferation rate is described in terms of a population
doubling time, the Potential Doubling Time (Tpot).
• longest Tpots of any human tumors, from 15 to more than 70 days
• Alpha by beta is 1.5 (0.8,2.2)
Brenner DJ and Hall EJ: Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol
Biol Phys, 1999.
4. THREE LARGE REVIEWS
Scott Williams et al
Australia 2011
Jolyon Hendry et al
Manchester 2012
Dasu et al 2012 Sweden
•5063 patients from 6
institutes
•Utilized long term PSA
dynamics
•5969 patients from 7
institute
•11330 patients treated
with conv. Fractionation
•2838 patients treated
with hypo fractionation
Alpha by beta was 1.55
Gy (0.46-4.52Gy)
Alpha by beta was 1.4
Gy (0.9-2.2Gy)
Alpha by beta
calculated 0.6 to 1.7
Gy inclusive of all risk
patients
6. SBRT
• Potential to improve
1. Therapeutic window
2. Higher local control
3. Reduced toxicity
4. Better QOL
5. Shorter treatment course
6. Lower cost
7. SBRT
WHICH RISK GROUP ?
DOSE ?
OUTCOME ?
TOXICITY PROFILE? ACUTE AND LATE ?
TECHNICAL FEASIBILITY ?
8. Most elaborate guideline so far published based on
1. Retrospective series long follow up
2. Phase I/II studies
3. A few randomized trials
4. A guideline from ASTRO
Published in JCO 2018
NCCN guideline mentions about SBRT prostate
UK SABR consortium guideline on prostate
9. KQ3: Ultrahypofractionation to which risk patients ?
KQ4: Different ultrahypofractionation regimens compared with one another
Control, Quality of life, toxicity
KQ5: Different normal tissue constraints used in clinical trials
KQ6: Different treatment volumes used in clinical trials
KQ7: Moderate or ultrahypofractionation using image guided radiation
therapy (IGRT)
KQ8: Moderate or ultrahypofractionation using intensity modulated
radiation therapy (IMRT)
Key questions
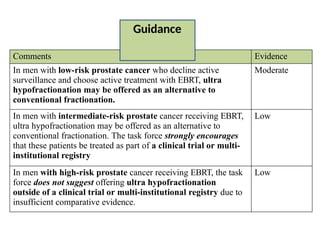
10. Comments Evidence
In men with low-risk prostate cancer who decline active
surveillance and choose active treatment with EBRT, ultra
hypofractionation may be offered as an alternative to
conventional fractionation.
Moderate
In men with intermediate-risk prostate cancer receiving EBRT,
ultra hypofractionation may be offered as an alternative to
conventional fractionation. The task force strongly encourages
that these patients be treated as part of a clinical trial or multi-
institutional registry
Low
In men with high-risk prostate cancer receiving EBRT, the task
force does not suggest offering ultra hypofractionation
outside of a clinical trial or multi-institutional registry due to
insufficient comparative evidence.
Low
Guidance
11. Guidance
Comments Evidence
Ultra hypofractionated prostate EBRT of 3,500 to 3,625 cGy in 5
fractions of 700 to 725 cGy to the planning target volume
may be offered to low- and intermediate-risk patients with
prostate sizes less than 100 cm3. The key dose constraints in
KQ5B should be followed
Moderate
Five-fraction prostate ultra hypofractionation at doses
above 3,625 cGy to the planning target volume is not
suggested outside the setting of a clinical trial or multi-
institutional registry due to risk of late toxicity
Moderate
Five-fraction prostate ultra hypofractionation using consecutive
daily treatments is not suggested due to potential increased
risk of late urinary and rectal toxicity.
Low
13. KINGS ET AL 2013 POOLED ANALYSIS
Risk group N (%) 35Gy 36.25Gy 38-40Gy ADT use Follow up
Low 641 (58%) 254 (40%) 319 (50%) 68(11%) 50 (8%) 36
Interm. 334 (30%) 108 (32%) 188 (56%) 38 (11%) 49(15%) 30.5
High 125 (11%) 23(18%) 82 (66%) 20 (16%) 48(38% 23
(1) Overall long term bRFS were
excellent, 93% for all patients, and
95%, 84% and 81% for low-,
intermediate- and high-risk patients,
respectively (p < 0.001)
(2) No differences in bRFS were
observed with or without the use of
ADT (p = 0.71)
(3) No differences were observed as a
function of total dose (p = 0.17)
(4) In cohort of long term follow up of 5
years Trend is noted for the 5-year
bRFS was 93% for patients receiving
a dose 35 Gy vs. 100% for those
receiving P36.25 Gy
14. Low risk Interm risk High risk
5yr bRFS
(%)
P 5yr bRFS
(%)
P 5yr bRFS
(%)
P
ADT 96.8 97.2 82.5
NO ADT 95.1 0.46 79.2 0.17 80.2 0.5
DOSE 35GY 95.8 72.3 NE
DOSE
36.25GY
95 0.77 87.2 0.73 74.1 0.99
DOSE 38-
40GY
94.4 0.41 96.7 0.58 NE 1
5-year PSA relapse-free survival rates
Individual subgroup analysis
Dose change / ADT use does not have any relation (significant)
KINGS ET AL 2013 POOLED ANALYSIS
15. Other supportive Trials
Study n Dose ADT bRFS
Loblow et al 2017# 84 L 35 Gy in 5Fr 1% 98% (5yr)
Mcbride et al 45L 36.5-37.5Gy in 5 fr 0% 98% (3yr)
Madsen et al 40L 33.5Gy in 5 Fr -- 90% (4yr)
Bolzicco et al 41 L, 42 I,
17 H
35Gy in 5 fr 29% 3 yr 94%
Boike et al 45 (I,L) 45Gy 5Fr / 47.5Gy 5 Fr /
50Gy 5 fr
- 100%
Mantz et al 2014* 102 40Gy in 5fr over 2 weeks 100%
Zimmerman et al
2016*
80 45Gy in 9 fr 98%
Hannan et al 2016* 91 L & I 45-50 Gy in 5fr 17% 100% L
98% I
Musunuru et al 2016* 84 35Gy in 5 fr 99%
*Prospective Trials
#Propensity matched analysis
•Mostly low & intermediate risk
disease
•Use of higher dose
16. Note:
• Most studies includes low and intermediate risk patients
• Doses are variable. Most common dose 36.25 Gy in 5
fractions
• Some prospective trials uses higher doses >40Gy in 5
Fr.
• bRFS are comparable between studies
• Loblow et al 2017 : Propensity matched analysis For the
conventional and ultra hypofractionation patients, a
biochemical disease-free survival (bDFS) trend was seen
favouring Ultra hypofractionation prior to matching (P
= 0.08), which achieved significance following matching
(P = 0.001).
At six years, bDFS was 85.9% for conventional
fractionation and 100.0% for ultrahypofractionation for
the matched patients (P = 0.045).
17. Study n Dose Toxicity
Musunuru et
al 2016*
84 35Gy in 5 fr
40Gy in 5 Fr
1. A significant increase in late toxicity observed
at the 4,000 cGy level.
2. Specifically, maximum late grade 2 GI toxicity
was identified in 8% at 35 Gy compared with
20% at 40 Gy (P = 0.012)
3. Maximum late grade 2 GU toxicity was seen in
5% at 35 Gy and 13% at 40 Gy (P = 0.02)
Hannan et al
2016*
91
L & I
45-50 Gy in
5fr
1. Incidence of acute grade 3 GI toxicity at 50 Gy =
1.6%
2. Late GI toxicity was identified as well at the
5,000 cGy level (6.6% grade 3 and 3.3% grade 4)
3. No late grade 3 or 4 toxicity at the 45 Gy level,
but late grade 3 GU toxicity was identified at
47.5 Gy (6.7% grade 3) and 50 Gy (4.9% grade 3
and 1.6% grade 4).
Other studies have shown that dose escalation do not differ by
bRFS and acute toxicity however late GI and GU toxicity >2 increase
at dose level 45Gy and 50 Gy
18. Randomized study
Hypo-RT-PC
42.7 Gy over 7 fractions
3 days per week
78Gy in 39 fractions
Primary end point: PSA relapse, clinical failure, or
both
Primary outcome: FFS
Secondary outcome: bDFS, cDFS, prostate
cancer-specific survival, OS, proportion of
patients achieving PSA response, time to change
of treatment, QOL and toxicity
19. • The 5-year failure-free survival which was comprised of 89% intermediate-risk patients
and 11% high-risk patients
•Almost identical in the treatment groups (84% in both groups; adjusted HR 1·002, 95% CI
0·758-1·325; log-rank p=0·99).
•Comparable to the outcome of the moderate hypo-fractionation trials.
FFS
Hypo-RT-PC
20. OUTCOME UHF (%) CF (%) P
GRADE2+GU 27.6 22.8 0.11
GRADE2+GI 9.4 5.3 0.23
2 YR GR 2 GU 5.4 4.6 0.59
2YR GR 2 GI 2.2 3.7 0.20
2 YR IMPOTENCE 34 34
QOL (PRO) AT 2 YEARS No diff
Acute bowel QOL Worse <3 months
1 year Urinary QOL Worse for UHF
Sexual QOL SAME
Acute deterioration in GI and GU toxicity
With long follow up late toxicity between UHF and CF is insignificant
Hypo-RT-PC
21. • Patient-reported
outcomes revealed
significantly higher levels of
acute urinary and bowel
symptoms in the UHF group
compared with the
conventional fractionation
group
• No significant increases in
late symptoms were found,
except for increased urinary
symptoms at 1-year follow-
up, consistent with the
physician-evaluated toxicity
Hypo-RT-PC
GU
GI
22. Kishan et al. 2019
• Report on 2142 patients from 10 institution
• 7-year OS
Low-risk disease was 91.4% (95% CI, 89.4%-93.0%)
Intermediate-risk disease was 91.7% (95% CI, 89.2%-93.6%).
Favorable intermediate-risk disease was 93.7% (95% CI, 91.0%-95.6%),
Unfavorable intermediate-risk disease was 86.5% (95% CI, 80.6%-90.7%)
• Some patients has completed 9 year survival.
Kishan et al 2019
23. Jackson et al, IJROBP, 2019
• Thirty-eight unique prospective series were identified comprising 6116 patients
• 92% :low risk , 78%-intermediate risk, and 38%-high risk
• 5- and 7-year bRFS rates were 95.3% and 93.7% respectively.
•Estimated late grade 3 genitourinary and gastrointestinal toxicity rates were 2.0% (95%
CI, 1.4%- 2.8%) and 1.1% (95% CI, 0.6%-2.0%), respectively.
•By 2 years post-SBRT, Expanded Prostate Cancer Index Composite urinary and bowel
domain scores returned to baseline.
•Increasing dose of SBRT was associated with improved biochemical control (P
= .018) but worse late grade 3 GU toxicity (P = .014).
25. Pace trial
PACE A
Potential surgical
candidates are randomised
between radical
prostatectomy and SBRT
(36.25 Gy in 5 fractions).
Slow Accrual
PACE B
Randomisation is between
standard radiotherapy
(78Gy in 39 fractions or
62Gy in 20 fractions) and
SBRT (36.35Gy in 5
fractions).
Primary outcome: freedom from biochemical or clinical failure.
Co- primary outcomes: Acute toxicity , gastrointestinal or
genitourinary toxic effects score up to 12 weeks after radiotherapy
Toxicity data
reported
26. GI MF UF
GR 1 264 (61%) 219(53%)
GR 2 49(11%) 42(10%)
GR 3 4(1%) 1(<1%)
GR 4 0 0
GU
GR 1 254(59%) 236(57%)
GR 2 111(26%) 86(21%)
GR 3 6(1%) 8(2%)
GR 4 1(<1%) 2(<1%)
Further data is awaited
1.Used IGRT: however preliminary data
does not show any toxicity difference in
Cyberknife vs LINAC.
2. Comparator arm was moderately
fractionated )in HYPO RT
PC
Bowel
adverse
event
Bladder
adverse
event
27. NRG –GU005 HEAT
70.2 Gy in 26 fractions VS. 36.25 Gy in 5
fractions to PTV
SBRT (5 fractions of 7.25 Gy) vs. hypo
fractionated IMRT (28 fractions of 2.5 Gy)
Primary outcome : Two-year failure rates
(biochemical or clinical failure, or positive
biopsy)
Primary outcome :
Toxicity
DFS
Secondary outcome:
Acute toxicity
QOL
Efficacy
Cost efficacy
Late toxicicty
Secondary outcome:
OS
QOL
Biochemical Failure
Local failure
These studies are about SBRT in low and intermediate risk prostate
However there are other trials in node positive and high risk
prostate
28. PRIME TRIAL ( Vedang Murthy et al; TMH Mumbai)
• Adenocarcinoma prostate localised to prostate and pelvic nodes : first trial
A. High-risk/very high-risk (High risk clinical stage T3a or Gleason score
8/Gleason grade group 4 or Gleason score 9 to 10/Gleason grade group 5,
prostate-specific antigen (PSA) >20ng/mL
B. Very high risk prostate cancer, that is, T3b/T4 or primary Gleason
pattern 5/Gleason grade group 5 or >4 cores, Gleason score 8 to 10/Gleason grade
group 4 or 5)
Prostate 68Gy in 25 Fr
Pelvis 50Gy in 25 Fr
On the basis of nodal
response to ADT 62.5Gy in
25 Fr
SBRT prostate 36.25Gy in 5Fr
Pelvis 25 Gy in 5 Fr
On the basis of nodal response
to ADT 30-35Gy in 25 Fr
Primary outcome : 4yr bRFS
Secondary outcome: Acute and late toxicity ascertaining to OS and prostate cancer
specific survival
QOL
Out of pocket expenditure in two arms
29. Initial data from TMH (prostate and gross node dose was 35-37.5 Gy in 5 alternate
day fractions. Node-positive patients received 25 Gy to pelvic nodal regions until the
common iliac nodes)
• No acute grade ≥ 3 GU or GI toxicity was noted.
• Acute grade 2 GU and GI toxicity were 12% and 3%, respectively.
• Late grade 3 GU and GI toxicity was 3% and 0%, respectively.
• There was no increase in acute or late gastrointestinal toxicity with prophylactic pelvic
nodal radiotherapy.
• Prior transurethral resection of prostate (n = 11) did not increase toxicity.
• At a median follow-up of 18 months, 97% patients were alive and 94% were
biochemically controlled.
• Another Propensity score matched analysis between TURP and Non -TURP patient
showed some modest increase in GU toxicities however it remains low with SBRT in
post-TURP patients. SBRT can be safely performed in carefully selected post-TURP
prostate cancer patients.
Early Results of Extreme Hypofractionation Using Stereotactic Body Radiation Therapy for High-risk, Very High-risk and Node-positive Prostate
Cancer. Vedang Murthy et al 2018
Safety of Prostate Stereotactic Body Radiation Therapy after Transurethral Resection of Prostate (TURP): A Propensity Score Matched Pair Analysis
Vedang murthy 2019
High risk and node positive ca prostate
30. SHORT TRIAL
• Phase I/II study
• Any Gleason score, T1-4 prostate with PSA <60ng/ml
• 35Gy in 5 Fr to primary and 25Gy in 5 Fr to pelvis
• Out of 30 patients, 20 patients are in high risk
• Urinary symptom score showed a clinically meaningful worsening from a
mean of 20/100 at baseline to 34/100 at the end of treatment (P <
0.001), but reduced to 24/100 at 6 months (P = 0.08).
• With a median follow-up of 41.5 months, two patients each reported
grade 2 late urinary and rectal toxicity.
• The 3- and 4-year biochemical control rates were 96.7 and 87.9%,
respectively.
I Mallick et al 2020
31. TECHNIQUES
•Selecting a case
•Segmentation
•Treatment technique
•Image guidance
Selecting cases
1. Low or intermediate risk case
2. Prostate volume <100 CC however large prostate is not per se an
absolute contraindication
3. No prior irradiation / inflammatory bowel disease
4. Large TURP defects : SBRT not practiced
5. Obstructive urinary features e.g.: IPSS >20
32. 1. Bladder : Bladder protocol to reduce bowel toxicity but has inherent
reproducibility issue (usual practice).
2. Empty bladder is more reproducible.
• Rectal contour : Empty rectum is the norm. Liberal use of laxative is practiced
along with low motility low gas forming diet.
• Other interventions :
I. Rectal balloons: Rectal balloons increase the high dose irradiated area along
with
superior part which may get higher dose
II. Rectal hydro gel spacer: It may be used to facilitate more distance between
prostate and rectum
• Simulation :
1. CT simulation with 2.5 mm cuts
2. Planning MRI T2W : co registered with prostate
Simulation
33. Segmentation
• MRI fusion assisted segmentation
Extra prostatic spread , SV invasion are better appreciated
Better OAR delineation – urethra, penile bulb
Over estimation of prostate can be prevented
• CTV : Low risk : Prostate
Intermediate risk : prostate and proximal SV
High risk : poorly representated (Prostate and node)
• PTV : Most common 5 mm isotropic margin with 3 mm posterior in rectal
interface.
• Nodes : Nodal contour up to L5-S1
34. Planning parameters:
Goals:
1. Prescription dose should cover a minimum of 95% of the PTV.
2. Minimum dose within the PTV (0.03 cc in size) must be ≥95% of the prescribed dose.
3. For IMRT, the maximum dose within the PTV is 7% above the prescribed dose (a point
of 0.03 cc).
4. For Cyber knife, the max dose allowed within the PTV is 20% above the prescribed
dose (a point of 0.03cc)
5. The prescription doses must not occur outside of the PTV. Any hotspots should be
manipulated to avoid the prostate-rectal and prostate-bladder interfaces as defined
by the CTV.
6. Acceptable Variation: Cases in which this small volume of at least 0.03cc receives a
minimum dose that is <95% but >93% or a maximum dose that is >107% and <110% of
the prescribed dose.
35. ASTRO guideline
Normal tissue constraints (At least two dose-volume constraint points
for rectum and bladder should be used for moderately or ultra-
hypofractionated EBRT: one at the high-dose end (near the total dose
prescribed) and one in the mid-dose range (near the midpoint of the
total dose).
*Prime Study Protocol
*Murthy V, et al. BMJ Open 2020
36. • IGRT is advisable (ASTRO)
• Studies have used different techniques and machines
- (Outcome is not different among 3D / CYBERKNIFE/ IGRT)
- Yu Wen Li et al 2014 compared treatment plans between non-isocentric
plans in cyberknife vs. Isocentric Rapidarc : differences are evident
attributable to different machines.
Rapid arc compared to Cyber knife showed
1. Better dose conformity,
2. Better adjacent
3. Organ sparing
4. Better dose fall off profile as it has FFF
5. Less MU
6. Less time
37. Prostate localization & motion management
• Intra fraction and inter fraction motion
- Happens due to rectal distension and variable bladder filling, cystitis
feature, long treatment time
• Image guidance:
1. Gold fiducials : Intra prostatic gold fiducials helpful in image matching by 2D (e.g.:
Exactrac, EPID) and 3D (e.g.: CBCT , Helical tomo MV imaging) method.
2. Magnetic transponders : Real-time tracking by Calypso beacon transponders
3. Trans abdominal ultrasound system: To confirm the prostate position along other
OAR position.


















































![management of advanced cervical cancer [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/managementofadvancedcervicalcancerautosaved-230926014710-62f747b3-thumbnail.jpg?width=560&fit=bounds)




















































