


![Radiographic Features
▪ INTERNAL STRUCTURE; Totally radiolucent.
▪ However, long-standing cysts may have dystrophic calcification, which can give the internal
aspect a sparse, particulate appearance.
▪ Some cysts have septa, which produce multiple loculations separated by these bony walls or
septa.
▪ Cysts that have a scalloped periphery may appear to have internal septa
▪ EFFECTS ON SURROUNDING STRUCTURE
▪ Sometimes causing displacement and resorption of teeth. [Sharp and Curved]
▪ Cysts can expand the mandible, usually in a smooth, curved manner, and change the buccal or
lingual cortical plate into a thin cortical boundary.
▪ Cysts may displace the inferior alveolar nerve canal in an inferior direction or invaginate into
the maxillary antrum.](https://image.slidesharecdn.com/8-201017161631/85/Radiographic-Interpretation-of-Cyst-and-Cyst-like-Lesions-of-the-Jaws-4-320.jpg)





















































Radiographic Interpretation of Cyst and Cyst-like Lesions of the Jaws
- 1. Cysts and Cyst-Like Lesions Dr. Hadi Munib Oral and Maxillofacial Surgery Resident
- 2. Introduction ▪ Cyst is a pathologic cavity filled with fluid, lined by epithelium, and surrounded by a definite connective tissue wall. ▪ The cystic fluid either is secreted by the cells lining the cavity or derives from the surrounding tissue fluid. ▪ Cysts occur more often in the jaws than in any other bone ▪ Cysts are radiolucent lesions, and the prevalent clinical features are swelling, lack of pain (unless secondarily infected or is related to a non-vital tooth), ▪ Association with unerupted teeth, especially third molars.
- 3. Radiographic Features ▪ LOCATION ▪ Any location in the maxilla or mandible but are rare in the condyle and coronoid process. ▪ Odontogenic cysts are found most often in the tooth-bearing region. ▪ In mandible, they originate above the inferior alveolar nerve canal. ▪ Odontogenic cysts may grow into the maxillary antrum. ▪ PERIPHERY ▪ Well-Defined and corticated (fairly uniform, thin, radiopaque line). ▪ Secondary infection or a chronic state can change this appearance into a thicker, more sclerotic boundary or make the cortex less apparent. ▪ SHAPE; Round or oval, resembling a fluid-filled balloon. Some cysts may have a scalloped boundary.
- 4. Radiographic Features ▪ INTERNAL STRUCTURE; Totally radiolucent. ▪ However, long-standing cysts may have dystrophic calcification, which can give the internal aspect a sparse, particulate appearance. ▪ Some cysts have septa, which produce multiple loculations separated by these bony walls or septa. ▪ Cysts that have a scalloped periphery may appear to have internal septa ▪ EFFECTS ON SURROUNDING STRUCTURE ▪ Sometimes causing displacement and resorption of teeth. [Sharp and Curved] ▪ Cysts can expand the mandible, usually in a smooth, curved manner, and change the buccal or lingual cortical plate into a thin cortical boundary. ▪ Cysts may displace the inferior alveolar nerve canal in an inferior direction or invaginate into the maxillary antrum.
- 6. Radicular Cyst ▪ Periapical cyst, apical periodontal cyst, and dental cyst ▪ Epithelial cells (Malassez) in the periodontal ligament are stimulated to proliferate and undergo cystic degeneration by inflammatory products from a non-vital tooth. ▪ Clinical Features ▪ Most common type of cyst in the jaws. ▪ No symptoms unless secondary infection occurs. ▪ May feel bony and hard if the cortex is intact, crepitant as the bone thins, and rubbery and fluctuant if the outer cortex is lost. ▪ The incidence is greater in the third to sixth decades and shows a slight male predominance.
- 7. Radicular Cyst ▪ Radiographic Features ▪ Location. ▪ At the apex of a non-vital tooth ▪ Occasionally it appears at the opening of an accessory canal, or infrequently in a deep periodontal pocket. ▪ 60% are found in the maxilla, especially around incisors and canines. ▪ Well-defined cortical border and Radiolucent internal Structure ▪ Displacement/ Resorption of teeth ▪ Differential Diagnosis; Apical Granuloma ▪ Management
- 12. Healing Cyst
- 13. Residual Cysts ▪ Cyst that remains after incomplete removal of the original cyst; radicular cyst that may be left behind ▪ Clinical Features; Asymptomatic ▪ Radiographic Features ▪ Location. Found slightly more often in the mandible. ▪ In the mandible the epicenter is always above the inferior alveolar nerve canal ▪ A residual cyst has a cortical margin and is oval or circular. Radiolucent ▪ Effects on Surrounding Structures. can cause tooth displacement or resorption, invagination into the maxillary antrum or depress the inferior alveolar nerve canal
- 14. Residual Cyst ▪ Differential Diagnosis ▪ Solitary Bone Cyst ; below the mandibular canal ▪ Odontogenic Keratocyst. ▪ Management ▪ Surgical removal or marsupialization
- 15. Dentigerous Cyst ▪ Follicular cyst ▪ Forms around the crown of an unerupted tooth. ▪ An eruption cyst is the soft tissue counterpart ▪ Dentigerous cysts are the second most common type of cyst ▪ Unerupted tooth or supernumerary tooth. ▪ Around supernumerary teeth account for about 5% of all dentigerous cysts, most developing around a mesiodens in the anterior maxilla.
- 16. Dentigerous Cyst ▪ Radiographic Features ▪ Location; Most commonly the mandibular or maxillary third molar or the maxillary canine. ▪ Diagnostic point is that this cyst attaches at the CEJ. ▪ Lateral Dentigerous Cyst; beside the crown instead of above the crown. ▪ Cysts related to maxillary third molars often grow into the maxillary antrum ▪ Cysts attached to the crown of mandibular molars may extend a considerable distance into the ramus. ▪ Well-DefinedCortex with Radiolucent internal structure ▪ Effects on surrounding Structure; Resorption/ Displacement
- 17. Dentigerous Cyst ▪ Differential Diagnosis ▪ Hyperplastic Follicle; The size of the normal follicular space is 2 to 3 mm ▪ A cyst should be considered with any evidence of tooth displacement or considerable expansion of the involved bone ▪ Odontogenic Keratocyst; Does not expand the bone similar to Dentigerous, less likely to resorb teeth, and may attach further apically on the root ▪ Ameloblastic Fibroma ▪ Cystic Ameloblastoma ▪ SURGICAL REMOVAL
- 23. Buccal Bifurcation Cyst ▪ Mandibular Infected Buccal Cyst ▪ Inflammatory /Paradental cyst ▪ Epithelial cell rests in the periodontal membrane of the buccal bifurcation of mandibular molars ▪ A common sign is the lack of or a delay in eruption of a mandibular first or second molar. ▪ On clinical examination the molar may be missing or the lingual cusp tips may be abnormally protruding through the mucosa, higher than the position of the buccal cusps. ▪ The first molar is involved more frequently than is the second molar. ▪ The teeth are always vital. ▪ The age of detection is younger, within the first two decades for a BBC rather than the third decade with a paradental cyst of the third molar.
- 24. Buccal Bifurcation Cyst ▪ Radiographic Features ▪ Location. The mandibular first molar is the most common location followed by the second molar, occasionally is bilateral ▪ Periphery and Shape; Not readily apparent, and the lesion may be a very subtle radiolucent region superimposed over the image of the roots of the molar. ▪ In other cases the lesion has a circular shape with a well-defined cortical border. ▪ Internal Structure. The internal structure is radiolucent. ▪ Effects on Surrounding Structures. The most striking diagnostic characteristic of a BBC is the tipping of the involved molar ▪ The root tips are pushed into the lingual cortical plate of the mandible ▪ The occlusal surface is tipped toward the buccal aspect of the mandible
- 25. Buccal Bifurcation Cyst ▪ Differential Diagnosis ▪ Periodontal Abscess ▪ Langerhans’ Cell Histiocytosis ▪ Dentigerous Cyst ▪ Management; Removal by conservative Curettage ▪ The involved molar should not be removed. ▪ BBCs do not recur.
- 27. Keratocyst OdontogenicTumor ▪ Odontogenic Keratocyst and Primordial cyst ▪ WHO considered it a tumor in 2005 ▪ Now it’s considered a cyst; Epithelium lining ▪ InnateGrowth potential ▪ Keratinized and thin (4 – 8 cell layers thickness) ▪ Account for about one tenth of all cystic lesions in the jaws ▪ 2nd to 3rd Decades of life, slight male predominance ▪ Swelling, Pain if secondarily infected, Aspiration delivers a yellowish cheesy like material ▪ High Recurrence Rate
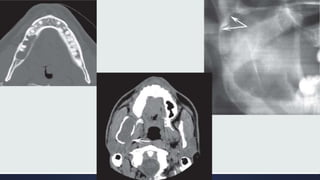
- 28. Keratocyst OdontogenicTumor ▪ Radiographic Features ▪ Location; Posterior body of the mandible (90% occur posterior to the canines) and ramus (more than 50%) ▪ The epicenter is located superior to the inferior alveolar nerve canal. ▪ Periphery and Shape; cortical border unless they have become secondarily infected. ▪ Internal Structure; Most commonly radiolucent. ▪ Effects on Surrounding Structures; Grows along the internal aspect of the jaws, causing minimal expansion
- 29. Keratocyst OdontogenicTumor ▪ Differential Diagnosis ▪ Dentigerous Cyst ▪ If several KOTs are found (which occurs in 4% to 5% of cases), these tumors may constitute part of a basal cell nevus syndrome. ▪ Management ▪ Enucleation and Curettage
- 33. Basal Cell Nevus Syndrome ▪ Gorlin - Goltz Syndrome ▪ Nevoid Basal Cell Carcinoma Syndrome ▪ Multiple Keratocysts ▪ Multiple Nevoid Basal Cell Carcinomas of the skin, ▪ Skeletal abnormalities; bifid rib (most common), agenesis, deformity, and synostosis of the ribs, kyphoscoliosis, vertebral fusion, polydactyly, shortening of the metacarpals, temporal and temporo-parietal bossing, minor hyper-telorism ▪ Central nervous system abnormalities ▪ Eye abnormalities
- 34. Gorlin-Goltz Syndrome ▪ Radiographic Features ▪ Location; the same as that of solitary KOTs, ▪ The multiple KOTs may develop bilaterally and can vary in size from 1 mm to several centimeters in diameter ▪ Other Radiographic Features ▪ Radiopaque line of the calcified falx cerebri may be prominent on the PA skull projection. ▪ Differential Diagnosis; Cherubism, Multiple Myeloma ▪ Management; More Aggressive
- 36. Lateral Periodontal Cyst ▪ Arise from epithelial rests in periodontium lateral to the tooth root. ▪ Usually is unicystic ▪ Botryoid odontogenic cysts; Cluster of small Cysts ▪ Clinical Features ▪ Asymptomatic and less than 1 cm in diameter. ▪ No apparent sexual predilection, and the age distribution extends from the second to the ninth decades ▪ If these cysts become secondarily infected, they will mimic a lateral periodontal abscess.
- 37. Lateral Periodontal Cyst ▪ Radiographic Features ▪ Location. A total of 50% to 75% of these cysts develop in the mandible, mostly in a region extending from the lateral incisor to the second premolar; Maxilla, between the lateral incisor and the cuspid. ▪ Periphery and Shape; Well-defined radiolucency with a prominent cortical boundary; Multilocular ▪ Effects on Surrounding Structures. ▪ Small cysts may efface the lamina dura of the adjacent root. ▪ Large cysts can displace adjacent teeth and cause expansion. ▪ Differential Diagnosis; Mental Foramen, Small Neurofibroma, Lateral RadicularCyst, Small Ameloblastoma ▪ Management
- 39. Glandular OdontogenicTumor ▪ Sialo-odontogenic cyst ▪ Arising from odontogenic epithelium with a spectrum of characteristics including salivary gland features such as mucus-producing cells. ▪ Slight female predominance, has an aggressive behavior and a tendency to recur after surgery. ▪ Radiographic Features ▪ Location; More commonly in the mandible and most often in the anterior mandible and in the maxilla, commonly the globule-maxillary region. ▪ Periphery and Shape. There is usually a cortical boundary that may be smooth or scalloped. ▪ Internal Structure; Unilocular and multilocular appearances ▪ Effects on Surrounding Structures. Perforation through the cortex and Displacement of teeth is a common feature. ▪ Differential Diagnosis; Ameloblastoma, KOT ▪ AggressiveTreatment
- 42. CalcifyingCystic OdontogenicTumor ▪ Calcifying odontogenic cyst ▪ Calcifying epithelial odontogenic cyst ▪ Gorlin cyst ▪ TheWorld Health Organization now categorizes this entity as a tumor. ▪ Uncommon, slow-growing, Painless, benign lesions. ▪ 2 peaks; First at 10 to 19 years of age and during the seventh decade ▪ Aspiration often yields a viscous, granular, yellow fluid. ▪ Most (75%) occur anterior to the first molar, especially associated with cuspids and incisors, where the cyst sometimes manifests as a pericoronal radiolucency. ▪ Occasionally (20% to 50% of cases) this tumor is associated with a tooth (most commonly a cuspid) and impedes its eruption.
- 43. CCOT ▪ Differential Diagnosis; Dentigerous Cyst ▪ Adenomatoid OdontogenicTumor ▪ Ameloblastic Fibro-Odontoma ▪ Calcifying Epithelial OdontogenicTumor ▪ Management; Enucleation and curettage ▪ Periodic Follow-up
- 45. Nasopalatine Duct Cyst ▪ IncisiveCanalCyst ▪ Median PalatineCyst; Posteriorly involving the hard palate ▪ 10% of cysts in the jaws ▪ Remnants of the Nasopalatine Duct cells ▪ Males * 3 times ▪ Small, well-defined swelling just posterior to the palatine papilla. ▪ Palatal to Incisors area ▪ Heart-Shaped Radiolucency (> 6 mm)
- 48. Nasolabial/ Naso-Alveolar Cyst ▪ Small, it may produce a very subtle, unilateral swelling of the nasolabial fold and may elicit pain or discomfort. ▪ When large, it may bulge into the floor of the nasal cavity, causing some obstruction, flaring of the alae, distortion of the nostrils, and fullness of the upper lip. ▪ The age of detection ranges from 12 to 75 years, with a mean age of 44 years. ▪ About 75% of these lesions occur in females. ▪ Adjacent to the alveolar process above the apices of the incisors. ▪ MRI; SoftTissue ▪ Surgical Removal; Intra-Oral Approach
- 50. Dermoid Cysts ▪ Cystic form of a teratoma thought to be derived from trapped embryonic cells that are toti-potential. ▪ The resulting cysts are lined with epidermis and cutaneous appendages and filled with keratin or sebaceous material (and in rare cases with bone, teeth, muscle, or hair, in which case they are properly called teratomas). ▪ Clinical Features ▪ May develop at any time from birth, but they usually become clinically apparent between 12 and 25 years ▪ The swelling, which is slow and painless, can grow to several centimeters in diameter, ▪ If located in the neck or tongue, it may interfere with breathing, speaking, and eating.
- 51. Dermoid Cyst ▪ Location; About 10% or fewer arise in the head and neck ▪ Only 1% to 2% develop in the oral cavity; Of these, about 25% occur in the floor of the mouth and on the tongue. ▪ Periphery and Shape. Well-defined by more radiopaque soft tissue of this cyst compared with surrounding soft tissue, as seen inCT scans. ▪ Internal Structure; Radiolucent on conventional radiographs. ▪ Differential Diagnosis ▪ Ranula (unilateral or bilateral blockage ofWharton’s ducts),Thyroglossal duct cysts, cystic Hygromas, Branchial cleft cysts, cellulitis, tumors (lipoma and liposarcoma), and normal fat masses in the submental area. ▪ Management; Do not recur after surgical removal.
- 53. Simple Bone Cyst ▪ Traumatic bone cyst, hemorrhagic bone cyst, extravasation cyst, progressive bone cavity, solitary bone cyst, and unicameral bone cyst ▪ Cavity within bone that is lined with connective tissue. ▪ It may be empty, or may contain fluid. ▪ However, because it has no epithelial lining, it is not a true cyst. ▪ The lesion shows a male predominance of approximately 2 : 1. ▪ Multiple SBCs can develop, especially when the disorder occurs with cemento-osseous dysplasia. ▪ The occurrence of SBCs in cemento-osseous dysplasia is seen in an older population, with a mean age of 42 years, and with a female predominance of 4 : 1. SBCs are asymptomatic in most cases. ▪ Aspiration usually produces only a few milliliters of straw-colored or serous-anguineous fluid.
- 54. Simple Bone Cyst ▪ Location. Almost all SBCs are found in the mandible ▪ Periphery and Shape; May vary from a well-defined, delicate cortex to an ill-defined border that blends into the surrounding bone. ▪ Internal Structure; totally radiolucent ▪ Differential Diagnosis ▪ KOT ▪ Fibrous Dysplasia ▪ Management; Marsupialization and Curettage
- 59. References ▪ Chapter 21: Cysts and Cyst-Like Lesions of the Jaws
- 60. THANKYOU!