STEMI, N-STEMI, and Everything else
Download as PPT, PDF34 likes6,655 views

This document provides information on STEMI, NSTEMI, and STEMI mimics for paramedics. It discusses the importance of accurate 12-lead ECG interpretation for identifying STEMIs to reduce door-to-balloon times and improve outcomes. It outlines criteria for calling a "Code STEMI" to activate the cardiac catheterization lab as well as situations where a "Medical Stat" or routine transport would be more appropriate based on the 12-lead findings. The goal is to minimize false STEMI activations while still rapidly identifying true STEMIs.












































































































STEMI, N-STEMI, and Everything else
- 1. STEMI, N-STEMI, and everything else Ada County Paramedics Block Training April 2008
- 2. Contact Information Ada County Paramedics 5870 Glenwood Boise, ID 83714 Adaparamedics.org 208-287-2972
- 3. Credit where Credit is due: Ada County Paramedics: Douglas Jay for his donation of materials as well as time. Jason Creamer, and Jeremy Schabot, both for their time, and their tireless devotion to raising the bar for paramedics everywhere. For Donation of materials and motivation: Hilton Head F&R, SC: Tom Bouthillet, Lt./NREMT-P Witham Health Services, Indiana: Andrew J. Bowman, MSN, NREMT-P Chris Smith, NREMT-P
- 4. Focus Statement This block of training will focus on Improving STEMI recognition, improving EMS involvement in E2B/D2B programs, and minimizing false STEMI team activations
- 6. Terminology PH ECG/PH 12 lead: Pre-hospital ECG PCT: Pre-hospital Cardiac Triage STEMI: S-T segment Elevation Myocardial Infarction N-STEMI: Non S-T segment Elevation Myocardial Infarction D2B: Door to Balloon (PTCA) E2B: EMS to Balloon SRC: STEMI Receiving Center (Primary PCI capable with surgical capability)
- 7. All Hail the Great S-T Segment (or …all you wanted to know about the ST segment but didn’t know to ask…)
- 8. Understanding the ST segment
- 11. Measuring ST Changes Baseline is correctly determined by finding the T-P to T-P segment. (If TP not measureable, then preceeding P-R interval can be used.) ST changes are measured 0.08 sec after the “J-point”. Changes must be present in 2 or more leads of a “lead group” to be significant. ST elevation or depression of 1 mm or greater in frontal plane leads is considered significant. ST elevation or depression of 2mm or greater in precordial leads is considered significant. ST elevation of 0.5mm or greater in R precordial leads is considered significant.
- 12. T-wave Changes in Ischemia Appear within seconds of onset of AMI Appear over zone of ischemia May be tall and or deeply inverted depending on location of ischemia Symmetry is important finding in ischemia Are associated with prolonged QT interval Often associated with ST depression Rapidly revert to normal after anginal attack Persist in q-wave infarct.
- 13. T-Wave Changes in Ischemia Peaked, Symmetrical T-Waves
- 14. T-wave changes in Ischemia Inverted T-waves
- 15. T-Wave Changes In Ischemia Tall, symmetrical T-Waves With ST Elevation
- 16. ST Depression in Ischemia ST depression is a sign of myocardial ischemia and can appear in setting of ischemia from any cause. Onset is usually within first hour of AMI, or more rapidly in other causes of ischemia. Often associated with T-wave changes Can resolved rapidly with reversal of ischemia. May persist in setting of AMI. Mimics include: Coronary artery spasm, acute pericarditis, ventricular aneurysm.
- 17. Types of ST Depression
- 18. ST Elevation in AMI Abnormal ST elevation is an ECG sign of myocardial injury. Usually occur within 20-40minutes following onset of infarction. Changes in diastolic resting potential of injured cells causes downward shift of T-Q interval. As AMI progresses ST elevation begins returning to baseline, as Q waves and flipped T-waves develop. ST Elevation mimics: pericarditis, early repolarization, LVH with strain pattern.
- 19. Reciprocal Changes? Reciprocal ST segment depression: In the setting of STE AMI, ST segment depression located in leads distant from the infarction is termed reciprocal change or reciprocal ST segment depression. Reciprocal change is useful diagnostically — its presence strongly suggests AMI prognostically — patients with such a finding have larger infarcts, lower resultant ejection fractions, and higher rates of death. Sometimes hard to differentiate form ST depression
- 20. S-T changes and their location?
- 21. Cardiac Anatomy in Relation to Coronary Artery Right coronary artery Septal wall V 1 -V 2 Left anterior descending artery Anterior wall V 3 -V 4 Left main coronary artery Circumflex artery Lateral wall I, aVL, V 5 -V 6
- 22. Associations Between Changes on 12-Lead ECG and Cardiac Anatomy aVF inferior III inferior V 3 anterior V 6 lateral aVL lateral II inferior V 2 septal V 5 lateral aVR I lateral V 1 septal V 4 anterior
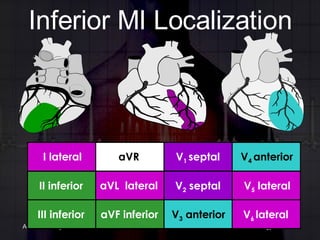
- 24. Inferior MI Localization aVF inferior III inferior V 3 anterior V 6 lateral aVL lateral II inferior V 2 septal V 5 lateral aVR I lateral V 1 septal V 4 anterior
- 27. Lateral MI Localization aVF inferior III inferior V 3 anterior V 6 lateral aVL lateral II inferior V 2 septal V 5 lateral aVR I lateral V 1 septal V 4 anterior
- 28. Lateral MI
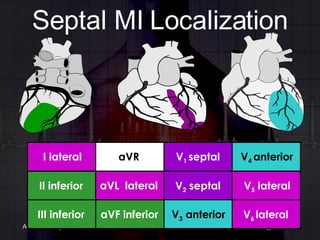
- 29. Septal MI Localization aVF inferior III inferior V 3 anterior V 6 lateral aVL lateral II inferior V 2 septal V 5 lateral aVR I lateral V 1 septal V 4 anterior
- 31. Inferior MI Localization aVF inferior III inferior V 3 anterior V 6 lateral aVL lateral II inferior V 2 septal V 5 lateral aVR I lateral V 1 septal V 4 anterior
- 32. Inferior MI
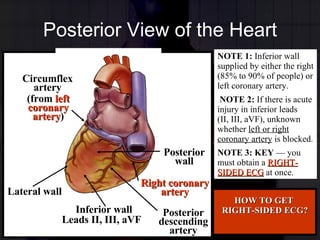
- 33. Posterior View of the Heart NOTE 1: Inferior wall supplied by either the right (85% to 90% of people) or left coronary artery. NOTE 2: If there is acute injury in inferior leads (II, III, aVF), unknown whether left or right coronary artery is blocked. NOTE 3: KEY — you must obtain a RIGHT-SIDED ECG at once. HOW TO GET RIGHT-SIDED ECG? Leads II, III, aVF (from left coronary artery ) Lateral wall Inferior wall Right coronary artery Posterior descending artery Posterior wall Circumflex artery
- 34. Right Ventricular Infarction Inferior lead changes RV infarction? Use lead V 4 R (ST elevation >1 mm) Clinical significance: Increased mortality Preload dependence Vasodilators ( Nitrates, MSO4 ) may cause severe hypotension What is management of RV infarction? Increase PRELOAD!! (FLUIDS)
- 35. STEMI, N-STEMI, and STEMI Mimics
- 36. Three “I”s Ischemia Injury Infarction
- 37. Spectrum of CAD No ST elevation ST elevation Unstable angina NSTEMI STEMI Stable angina Source (Photos): Davies MJ. Heart . 2000;83:361-366. CAD = coronary artery disease; NSTEMI = non-ST-segment elevation myocardial infarction; STEMI = ST-segment-elevation myocardial infarction. ACUTE CORONARY SYNDROMES
- 38. What is STEMI? S-T E levation M yocardial I nfarction Can we measure the ST segment accurately? What does the ST segment look like? WE CANT CALL A CODE STEMI IF WE DON’T KNOW HOW TO EVALUATE AN ST SEGMENT
- 39. N-STEMI? N-STEMI is an MI that does not show ST elevation You cannot call an N-STEMI a STEMI, regardless of how strongly you suspect the MI. You can call “Medical Stat” (Discussed later)
- 40. STEMI Mimics Things that make you go … HMMMM Things that look (at first glance) Like a STEMI or other MI pattern, but are NOT. Thinks that will cause you to INAPPROPRIATELY call a Code STEMI Increase “false positive rates” Still may be deadly serious conditions
- 41. The basics of doing the 12 lead
- 42. The Basic 12 Lead
- 43. Lead Placement for a Right-sided ECG
- 44. The Right Ventricular Leads
- 45. KEY POINT! BE SURE TO WRITE ON ECG THAT IT WAS A RIGHT SIDED ECG!
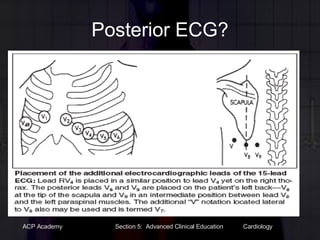
- 46. Posterior ECG?
- 47. The importance of serial 12 leads
- 49. STEMI MIMICS
- 51. Most common causes of STEMI mistakes RBBB/LBBB Pericarditis LVH Electrolyte Imbalances Drug Effects
- 52. Bundle Branch/Fascicular Blocks LBBB always indicates cardiac disease or injury. Just not always ACUTE injury Just not always MI, other “Mimics” can also cause BBB “ Making the diagnosis of acute infarction in the presence of left bundle-branch block can be problematic…” PROBLEM: Patients with (suspected new) LBBB tend to be REALLY BAD MI’s.
- 53. Bundle Branch/Fascicular Blocks Right Bundle Branch Block Do not rely on presence of “rabbit ears” for diagnosis of RBBB. Will miss many RBBBs.
- 54. AMI with BB? AMI should be no problem RBBB does not change S-T segment alterations LBBB can make things more interesting
- 55. Again with the serial ECGs??? Even though the LBBB makes initial ST evaluation difficult, the serial changes noted make this diagnostic for MI.
- 58. STEMI Mimics Pericarditis No reciprocal changes. There will only be S-T elevation, no depression. The myocardium is not involved. No changes will be noted to the QRS complex. Changes isolated to the S-T-T waves
- 61. STEMI Mimics Pericardial Effusion Distinctive pattern Changing polarity of Q-R-S
- 63. STEMI Mimics Hyperkalemia Progressive changes to de- & repolarization T wave peaks, then widens/flattens PR interval prolongs, and P wave flattens QRS widens also
- 64. Potassium Level: 6.1 mEq/L
- 65. Potassium Level: 7.2 mEq/L
- 66. Potassium Level: 9.1 mEq/L
- 67. STEMI Mimics Hypokalemia ST depression with prominent U-waves Prolonged repolarization T waves flatten Can mimic reciprocal changes
- 68. Potassium Level: 2.5 mEq/L
- 69. Potassium Level: 1.5 mEq/L
- 70. Potassium Level: 0.9 mEq/L
- 71. STEMI Mimics Cardiac Glycosides-Digoxin Digitalis effect-”scooped” ST segment Anti-dysrhythmic agents Based on where they work QT prolongation is common Psychotropic agents (i.e.TCA’s) Increase QRS duration Lengthen QT interval
- 75. STEMI Mimics Well, Kinda anyway Pacemakers
- 77. The Problem Research has recognized that half of patients with myocardial infarction do not arrive early enough (90 minutes) to PCI… Door to Balloon time <90 minutes is a class I Intervention in STEMI Numerous strategies to improve the “Door to Balloon” time have evolved.
- 78. The Solution New strategies have involved a player previously ignored in cardiac care… EMS! Local cardiology groups and hospitals have committed to involving EMS in improving time to PCI! This has a direct measurable effect on mortality!!! Only if the system works and EMS does its part!
- 79. Key to this is Pre-Hospital Cardiac Triage And accurate 12 lead interpretation! DON’T TELL ANYONE, BUT EMS HAS BEEN DOING 12 LEADS FOR ALMOST 40 YEARS!!!
- 80. First field 12 lead Seattle Medic One Circa 1969
- 81. WHY 12 leads? 12 leads are the KEY to open the DOOR to PCI!!!!! PARAMEDICS ARE THE KEYMASTERS WHO IS THE GATEKEEPER? ER Docs Cardiologist Bean Counters!!! TRUE STORY: EMS has 1 chance to impress and right now that chance is slipping away…
- 82. The KEYMASTER and the GATEKEEPER? 12 Leads!!!!
- 83. Time to Treatment in PCI (Nallamothu 2007 NEJM 357:1631) What this means: Beyond a D2B ≤90 Minutes… Every 15-minutes of Delay Mortality
- 84. Why the big push for PCI????? Better Outcomes, Lower Mortality, Less Complications
- 85. D2B Alliance Goal “ To achieve a door-to-balloon (D2B) time of 90 minutes for at least 75% of non-transfer primary PCI patients with ST-elevation myocardial infarction (STEMI) in all participating hospitals performing primary PCI” National baseline about 50% rate D2B 90 with out systems approach
- 86. NEW CONCEPT IN PCI No longer just Door to Balloon (D2B)…. Now EMS to Balloon (E2B)….
- 87. Understanding the Intervals Onset of symptoms of STEMI 9-1-1 EMS dispatch EMS on-scene Call 9-1-1 Call fast ACP S2B: S/S Onset to Balloon E2B: EMS to Balloon C2B: Call to Balloon D2B: Door to Balloon Hospital B A L L O O N R2R: Recognition (12 lead) to Re-perfusion
- 88. Isn't just doing PH 12 leads enough? In a nutshell: NO Implementation of PH 12 leads by itself did not significantly impact D2B times. PH 12 leads only shown to make a difference in a SYSTEMS/PROTOCOL driven approach Otherwise the 12 leads gather dust Fortunately SARMC/SLRC are interested in a SYSTEM
- 89. Pre-hospital Cardiac Triage Similar to nation’s current trauma systems: sick pts = special care at specialty centers with specialty team activation
- 90. 30-30-30 Goal E2B≤90 Conceptual Framework < 30 minutes for Emergency Med Services (EMS) < 30 minutes for the Emergency Department (ED) < 30 minutes for the Cardiac Cath Lab (CCL)
- 91. ACP approach for Transport of Patients With STEMI and Initial Reperfusion Treatment EMS Transport <20 min Onset of symptoms of STEMI 9-1-1 EMS dispatch EMS on-scene Mandatory 12-lead ECGs TRANSMIT 12-leads 1 minute PCI capable Not PCI capable Code STEMI and Rapid CCT Transfer STEMI Triage Hospital Destination Guidelines TIME LOST!!! CCT Required BEST PRACTICES : Golden hr = E2B/D2B within 1st 60 min Total ischemic time for E2B/D2B GOAL: within 120 min Call 9-1-1 Call fast Patient EMS E2B <90 min?: EMS Treat and transport to PCI Capable hospital Dispatch ????? Time 10 min ACP SLRMC SARMC SLMMC SAEMC VAMC WVMC MMC Code STEMI and Direct to PCI Med STAT- ED MD triage t PCI ASA? EMS PH 12 lead transmission
- 92. CODE STEMI is the “Level 1 Trauma” of the Cardiac World “Medical Stat” is the Level II and Level III
- 93. SO WHERE IS ACP? 2/2008 review for prior 6 months Total Charts Reviewed: 88 CODE STEMI charts reviewed: 28 Other Chest Pain/DX of AMI charts (No Code STEMI called): 60 3 charts out the 60 showed STEMI on EMS12 lead Results: Fail to recognize/report rate: 2.6% Of Code STEMI Called STEMI continued at hospital: 21 (75%) STEMI cancelled: 7 (25%) False Negative Rate -2.6% False Positive rate: -25% Goal is 5%
- 94. CAN WE DO BETTER? (and what happens if we don’t???????)
- 95. So what's the big deal? False Positives: (calling Code STEMI inappropriately) ? $$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$$ Urgent and “less emergent” PCI are bumped for the “code STEMI Cardiologist taken away from PCI and other duties WHOLE SYSTEM GETS ACTIVATED If 12 lead is not received, activation continues anyway
- 96. So what's the big deal? False Negatives: (No Code STEMI Called) MD does not see 12 lead, it sits and gathers dust. Consistently exceeding D2B >90 min Increased mortality
- 97. 3 layers of Safety Net Cognitive Detection The paramedic and his 12 lead is a beautiful thing Automated Detection “*** ACUTE AMI *****” Emergency Department Screening MD review to prevent false positives and to pick up on STEMI mimics that still need urgent care
- 98. 3 Levels of Notification CODE STEMI Medical STAT Business as Usual Routine Radio report
- 99. Proposed ACP protocol to reduce E2B Obtain and Transmit 12 lead Inclusionary Criteria Suspicion for ACS S/S AND ST Elevation 2mm in 2+ contiguous Leads Exclusionary Criteria NO QRS greater than 0.11 OR NO LBBB Inclusionary Criteria Automatic Detection : “Acute MI” Paramedic Discretion Suspicion for ACS S/S AND (Any of the following): Global ST Changes N-STEMI ST Elevation in 1 mm in Inferior Leads ST Depression or Inverted Ts in contiguous leads Questionable Reciprocal Changes Presumed New LBBB Inverted T-Waves or ST depression in 2+ contiguous leads Hyper-acute T waves present in 2+ contiguous leads. Exclusionary Criteria NONE CODE STEMI Medical STAT PH ECG Eval Radio Report Radio Report
- 100. Medical State Medical State can also be used on other time sensitive emergencies… Respiratory Failure with CPAP Field ETT placed “RT at bedside” “MD at bedside”
- 101. Closing Thoughts “ However, it is becoming increasingly clear that the emergency medical services (EMS) have an important role in STEMI patient care, and that a three-way partnership involving EMS, EM departments, and the CCL has substantial potential to increase access to PCI for STEMI and simultaneously reduce door-toballoon times.” Tom Bouthillet, FF/NREMT–P STEMISystems, Issue 2, May 2007
- 102. STEMI, Medical SAT, or Other? Click for answer
- 103. STEMI, Medical SAT, or Other? 26 y/o male presenting to EMS after arrest for probation violation. He is in booking, suddenly complains of chest discomfort. EMS is notified. Smokes a pack a week approx for 3 years No other history No reported drug use/abuse
- 104. STEMI, Medical SAT, or Other?
- 105. STEMI, Medical SAT, or Other? Click for answer
- 106. STEMI, Medical SAT, or Other? Click for answer
- 107. STEMI, Medical SAT, or Other?
- 108. STEMI, Medical SAT, or Other?
- 109. STEMI, Medical SAT, or Other?
- 110. STEMI, Medical SAT, or Other?
- 111. STEMI, Medical SAT, or Other? 45 y/o male with chest pain, nausea, vomiting, and dizziness while in bed. B/P 80/40 HR regular and tachycardic Has not been to a doctor since he was in the army 20 years previous Notably obese. Smokes
- 112. On final unrelated thought A recent review showed that less than 5% of patients who received NTG SL by ACP received NTG Paste in follow up. The benefits of NTG paste are significant You don’t have to do a full 3 doses to initiate it. Please consider it in the future.
- 113. Now for Hands on… Entering Names Right sided and posterior 12 lead placement Transmission of 12 leads Scenarios?