Systemic mycoses
Download as PPTX, PDF4 likes2,143 views

1. The document describes four systemic mycoses caused by dimorphic fungi: histoplasmosis, blastomycosis, coccidioidomycosis, and paracoccidioidomycosis. 2. It provides details on the causative agents, pathogenesis, clinical manifestations, laboratory diagnosis including histopathology, culture, and serology, and treatment recommendations for each fungal infection. 3. Key diagnostic methods include histopathological staining of tissue samples to identify characteristic fungal structures, culture of samples to demonstrate the dimorphic nature of the fungi, and serological tests to detect antibodies.




























Systemic mycoses
- 1. Systemic mycoses - DR. ANKUR KUMAR
- 2. Systemic mycoses Disease Causative agent 1. Histoplasmosis Histoplasma capsulatum 2. Blastomycosis Blastomyces dermatitidis 3. Coccidioidomycosis Cocddioides immitis 4. Paracoccidioidomycosis Paracoccidioides brasiliensis
- 3. HISTOPLASMOSIS • Systemic granulomatous disease caused by a dimorphic fungus, Histoplasma capsulatum. • Species name is misnomer as it is not capsulated. • Also known as Darling's disease (because they was first reported by Samuel Darling in1905 )
- 4. HISTOPLASMOSIS- Pathogenesis • Transmitted by- inhalation of spores (i.e. microconidia) which usually circulate in the air after the contaminated soil is disturbed. • Spores enter into the lungs engulfed inside the alveolar macrophages transform into yeast forms . • Yeasts survive within the phagolysosome of the macrophage by producing alkaline substances (bicarbonate and ammonia).
- 5. HISTOPLASMOSIS- Clinical Manifestations • Pulmonary hlstoplasmosis: Most common form. Acute form presents with mild flu like illness, pulmonary infiltrates in chest X-ray with hilar or mediastinal lymphadenopadiy. Chronic cavitary histoplasmosis may be seen in smokers with underlying structural lung disease. • Mucocutaneous histoplasmosis Skin and oral mucosal lesions may develop secondary to pulmonary infection. Oral lesions are particularly seen in Indian patients. • Disseminated histoplasmosis: Develops if CMI is very low (e.g. untreated HIV infected people or following organ transplantation). Common sites affected- bone marrow, spleen, liver, eyes and adrenal glands
- 6. HISTOPLASMOSIS- Laboratory Diagnosis • Specimens: Sputum, aspirate from bone marrow & lymph node, blood and biopsies from skin & mucosa. • Direct microscopy: Histopathological staining (PAS, Giemsa or GMS stain) – Shows tiny oval yeast cells (2-4 µm size) with narrow based budding within macrophages with an underlying granulomatous response.
- 7. HISTOPLASMOSIS- Laboratory Diagnosis • Culture: Gold standard method of diagnosis. Media- SDA, blood agar and BHI agar Incubated simultaneously at 25°C and 37°C. At 25°C: Mycelial phase Produces white to buff brown colonies, consist of 2 types of conidia or spores: 1) Tuberculate macroconidia- typical thick walls and finger-like projections which is a characteristic feature 2) Microconidia are smaller, thin, and smooth-walled. At 37°C: Gets converted into yeast form (creamy white colonies), which is best developed in special media like Kelley's media.
- 8. HISTOPLASMOSIS- Laboratory Diagnosis • Serology: Antibodies in serum - detected by CFT and imununodiffusion test. Antibodies appear after 1 month of infection; hence are more useful in chronic stage (often negative in early course and in disseminated stage). False positive result may occur due to past infection or cross infection with blastomyces. • Skin test: May be done to demonstrate delayed type hypersensitivity response to histoplasmin antigen, which indicates prior exposure
- 9. Histoplasma capsulatum (schematic diagram) A. Yeast form; B. Mycelial form; C. 2-4 µm yeast cells with narrow based budding (Giemsa stain) D. Mold form, septate thin hyphae with tuberculate macroconidia (arrows showing)
- 10. HISTOPLASMOSIS- TREATMENT • Liposomal amphotericin B Is the antifungal agent of choice in acute pulmonary and disseminated histoplasmosis. • ltraconazole Recommended for chronic cavitary pulmonary histoplasmosis.
- 11. BLASTOMYCOSIS • Also known as North American blastomycosis or Gilchrist's disease or Chicago disease • Is a fungal infection of humans and other animals also- dogs and cats, caused, Blastomyces dermatitidis.
- 12. BLASTOMYCOSIS- Pathogenesis • Transmitted by Inhalation of the conidia of B. dermatitidis. Spores enter into the lungs, and are engulfed by alveolar macrophages, where they get converted into yeast phase. This yeast expresses a 120-kDa glycoprotein called BAD-I (B. dermatitidis adhesin-1) which is an essential virulence factor and also a major inducer of cellular and humoral immune responses.
- 13. BLASTOMYCOSIS- Clinlcal Manifestations • Acute pulmonary blastomycosis - Most common form. • Extrapulmonary manifestations Skin involvement - Most common extrapulmonary form; characterized by either verrucous (more common) or ulcerative type of skin lesions. Osteomyelitis may develop along with contiguous soft tissue abscesses and draining sinuses. Prostate and epididymis involvement in men. Central nervous system (CNS) involvement has been reported in - 40% of AIDS patients. Brain abscess is the usual presentation, followed by cranial or spinal epidural abscess and meningitis.
- 14. BLASTOMYCOSIS- Laboratory Diagnosis • Antibody detection: lmmunodiffusion test specific for B. dermatitidis has been developed against yeast phase antigens such as antigen-A, BAD- I and ASWS antigen (alkali soluble water soluble). • Antigen detection assay- detect Blastomyces antigen in urine (more sensitive) and in serum is commercially available. • Molecular methods- DNA probe hybridization and real time PCR
- 15. BLASTOMYCOSIS- Laboratory Diagnosis • Histopathological staining of the tissue biopsy specimens reveals thick-walled round yeast cells of 8- 15 µm size with single broad-based budding (figure of 8 appearance) • Culture media - SDA, blood agar and BH I. At 250C- Mycelia form containing hyphae with small pear-shaped conidia are produced; At 370C- mold to yeast conversion takes place. • Skin test: done to demonstrate delayed type hypersensitivity to blastomycin antigen.
- 16. Blastomyces A. Schematic (Mycelial and yeast form); B. Histopathological stain (arrow shows) broad based budding yeast cells (figure o f 8 appearance)
- 17. BLASTOMYCOSIS- TREATMENT • Liposomal amphotericin B is the antifungal agent of choice in most of the cases. • ltraconazole in immunocompetent patients with mild pulmonary or non CNS extrapulmonary blastomycosis
- 18. COCCIDIOIDOMYCOSIS • Also called desert rheumatism or Valley fever or California fever • Is a systemic fungal disease caused by a dimorphic soil dwelling fungus- Coccidioides (C. immitis and C. posadasii).
- 19. COCCIDIOIDOMYCOSIS -Pathogenesis • Transmitted by inhalation of arthroconidia. • In lungs, they enlarge, become rounded, and develop internal septations to form large sac like structures of size up 10-200 µm called spherules- encompass numerous endospores. • Spherules may rupture and release packets of endospores that can disseminate and develop into new spherules. • If spherules returned to artificial media or soil, they revert back to the mycelial stage.
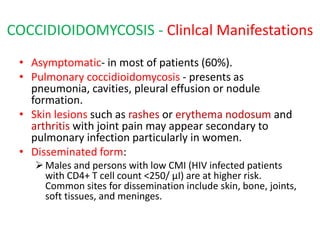
- 20. COCCIDIOIDOMYCOSIS - Clinlcal Manifestations • Asymptomatic- in most of patients (60%). • Pulmonary coccidioidomycosis - presents as pneumonia, cavities, pleural effusion or nodule formation. • Skin lesions such as rashes or erythema nodosum and arthritis with joint pain may appear secondary to pulmonary infection particularly in women. • Disseminated form: Males and persons with low CMI (HIV infected patients with CD4+ T cell count <250/ µI) are at higher risk. Common sites for dissemination include skin, bone, joints, soft tissues, and meninges.
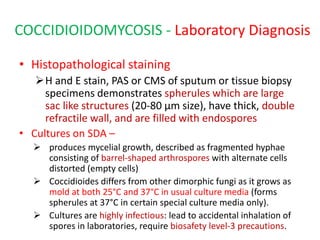
- 21. COCCIDIOIDOMYCOSIS - Laboratory Diagnosis • Histopathological staining H and E stain, PAS or CMS of sputum or tissue biopsy specimens demonstrates spherules which are large sac like structures (20-80 µm size), have thick, double refractile wall, and are filled with endospores • Cultures on SDA – produces mycelial growth, described as fragmented hyphae consisting of barrel-shaped arthrospores with alternate cells distorted (empty cells) Coccidioides differs from other dimorphic fungi as it grows as mold at both 25°C and 37°C in usual culture media (forms spherules at 37°C in certain special culture media only). Cultures are highly infectious: lead to accidental inhalation of spores in laboratories, require biosafety level-3 precautions.
- 22. COCCIDIOIDOMYCOSIS - Laboratory Diagnosis • Serology: Antibodies are detected by immunodiffusion test and CFT. • Skin test: It is done by fungal extaracts (coccidioidin or spherulin); produces at least a 5 mm induration within 48 hours after injection (delayed hypersensitivity reaction) indicates past infection.
- 23. Cocddioides A. Spherules (schematic); B. Hyphae with arthroconidia (schematic); C. Spherules (PAS staining); D. Hyphae with arthroconidia (LPCB mount)
- 24. TREATMENT- Coccidioidomycosis • Itraconazole -drug of choice except for diffuse pneumonia with pulmonary sequelae where amphotericin B is recommended.
- 25. PARACOCCIDIOIDOMYCOSIS • Also known as South American blastomycosis, Lutz-Splendore-de Almeida disease • Is a systemic disease caused by the dimorphic fungus Paracoccidioides brasiliensis.
- 26. Pathogenesis and clinical Manifestations • Transmission- by inhalation of spores, • Transform into the yeast phase in lungs. • Occurs as two major forms. 1. Acute form (or juvenile type): affects young adults under 30 years age. less common variety, but more severe form, manifests as disseminated infection involving multiple viscera and is refractory to t/t. 2. Chronic form (or adult form): accounts for 90% of cases predominantly affects older men. results from reactivation of quiescenct lung lesions. less severe form, manifested as progressive pulmonary disease affecting lower lobes, with fibrosis. Skin, oral mucosal lesions and cervical lymphadenopathy
- 27. PARACOCCIDIOIDOMYCOSIS-Laboratory Diagnosis • Histopathological staining - of pus, tissue biopsies or sputum reveals round thick-walled yeasts, which multiple narrow- necked buds attached circumferencially giving rise to Mickeiy mouse or pilot wheel appearance. • Culture on SDA yields mycelial form at 250C converts in to yeast phase at 370C when grown in BHI agar supplemented with blood and glutamine. • Serology: Antibodies are detected by immunodiffusion, and by ELISA, using gp43 antigen of P. brasiliensis. • Skin test: demonstrates delayed hypersensitivity response against paracoccidioidin antigen.
- 28. Paracoccidioidomycosis A. Schematic representation of mycelial and yeast forms; B. Methenamine silver staining shows yeast from (pilot wheel appearance)
- 29. TREATMENT- Paracoccidioidomycosis • ltraconazole - is the treatment of choice except for the seriously ill patients where Amphotericin B is recommended. Sulfonamides are effective, but the response is slow with frequent relapses.
- 30. THANK YOU