neurologia
Descargar como PPT, PDF78 recomendaciones34,336 vistas

El documento proporciona una guía detallada para realizar un examen neurológico completo. Incluye instrucciones para evaluar la conciencia, facies, actitud, marcha, función motora, sensibilidad, reflejos y signos meníngeos. El examen cubre pruebas como la exploración del estado de conciencia, examen de la marcha, pruebas de los reflejos patológicos y la evaluación de la sensibilidad somática y profunda.





















































































































































neurologia
- 1. EXAMEN NEUROLOGICO 1. CONCIENCIA 2. FACIES 3. ACTITUD 4. BIPEDESTACION Y ROMBERG 5. MARCHA 6. FUNCION MOTORA Mov. Pasivo Mov. Reflejo Mov. Activo Mov. Automático. FUNCION SENSITIVA COORDINACION SIGNOS MENINGEOS NERVIOS CRANEALES F.N.S. : Lenguaje, praxia y gnosia PSIQUISMO
- 2. EXAMEN NEUROLOGICO CONCIENCIA .- Es el conocimiento de si mismo y del medio que lo rodea LUCIDEZ .- Orientación en tiempo, espacio y persona ESTRUCTURAS ANATOMICAS CORTEZA CEREBRAL SARA
- 3. S.A.R.A Figure .- Brainstem reticular activating system and its ascending projections to the thalamus and cerebral hemispheres
- 4. COMPROMISO DE CONCIENCIA GRADOS : EMBOTAMIENTO .- Despierto, desorientado parcialmente en T y E. SOMNOLENCIA .- Desorientación parcial en T yE, con tendencia al sueño, despierta con facilidad. SOPOR .- Desorientación en T,E y P. Necesita estímulo enérgico para despertar COMA .- Estado de inconciencia, indica disfunción encefálica grave
- 5. EXPLORACION DEL ESTADO DE CONCIENCIA Determinar si el paciente está despierto o dormido . Si está despierto determinar: Orientado en Tiempo : Preguntar fecha actual(día, mes,año) Orientado en Espacio : Preguntar donde se encuentra, dirección de domicilio Orientado en persona : Nombre, edad, fecha de nacimiento. Si está dormido determinar si solo necesita: Solicitud verbal para despertar u órdenes reiteradas Si despierta y tiende a la somnolencia al dejar de estimular, se realizará gestos de amenaza
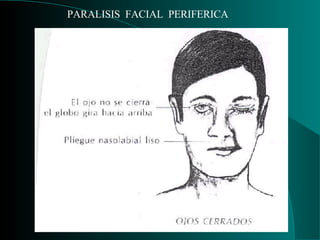
- 6. EXAMEN DE LA FACIES INSPECCION : Simetría facial Expresión facial Se evaluará el estado estático y la actividad motora
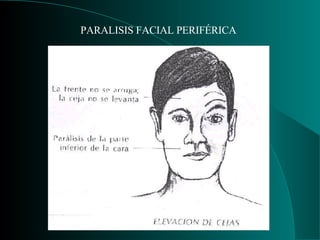
- 9. PARALISIS FACIAL PERIFERICA
- 12. ACTITUD Posición adoptada por el cuerpo humano. Puede ser local o general. LOCALES : Parálisis del plexo braquial, mano en garra (N. Cubital), mano del predicador (cubital y mediano). GENERALES : Opistótonos, emprostótonos, pleurotótonos, posición en gatillo de fusil, actitud hemipléjica, paraparética, etc.
- 16. EXAMEN DE LA BIPEDESTACIÓN BIPEDESTACIÓN .- Es la posición de pie. Normalmente es estable Se examina con el paciente de pie, en actitud de firmes, observando si es: ESTABLE.- INESTABLE .- Pulsiones unilaterales, multidireccionales. ROMBERG Evalúa sensibilidad profunda. Romberg es positivo cuando el paciente cae. Romberg sensibilizado.- Eleva un pie o un pie delante de otro.
- 20. EXPLORACION DE LA MARCHA EXAMEN : Camine normalmente Sobre punta de pies Sobre talones Con los pies uno detrás del otro TIPOS DE MARCHA : Marcha parética Marcha espástica Marcha atáxica Marcha tabética Marcha cerebelosa Marcha vestibular Astasia abasia
- 23. FUNCION MOTORA Evalúa : Movimiento activo Movimiento pasivo Movimiento reflejo Movimiento automático
- 24. MOVIMIENTO ACTIVO Es el desplazamiento de una parte o de todo el cuerpo en el que interviene la voluntad. ALTERACIONES : Parálisis o plejía .- Es la pérdida del movimiento voluntario ocasionado por lesión de la motoneurona central o periférica. Paresia .- Grado menor de parálisis, consistente en disminución del movimiento voluntario Impotencia muscular .- Déficit motor dependiente de causa extra neurológica. Ejm. Alteraciones musculoesqueléticas, inflamatorias, traumáticas.
- 25. EXPLORACION DEL MOVIMIENTO ACTIVO El objetivo es reconocer si el paciente puede realizar movimientos sugeridos. Se observará las siguientes características: Velocidad .- Observar lentitud o rapidez de los movimientos Amplitud .- Registrar los movimientos anormales extensos o reducidos. Destreza .- Habilidad con que se ejecuta un movimiento. Se examinará mediante la oposición del dedo pulgar a los demás dedos. Energía .- Fuerza muscular. Se explora oponiendo resistencia al movimiento que el paciente ejecuta. Maniobras especiales que exploran la resistencia contra la gravedad: Prueba de Juramento Maniobra de Mingazini Maniobra de Barré
- 28. MOVIMIENTO PASIVO TONO MUSCULAR .- Estado de semicontracción permanente, involuntario, no fatigante, de carácter reflejo, encaminado a conservar una actitud
- 29. EXPLORACION DEL TONO MUSCULAR Extensibilidad .- Explora la amplitud a nivel de las articulaciones. Pasividad .- Explora el grado de resistencia al movimiento pasivo. Se explora mediante el sacudido de manos cogidas por las muñecas.
- 30. MOVIMIENTO REFLEJO REFLEJO Respuesta estereotipada, motriz o secretora, independiente de la voluntad, provocada inmediatamente ante la aplicación de un estímulo sobre un determinado tipo de receptor
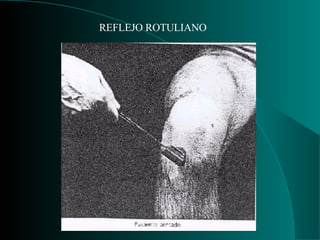
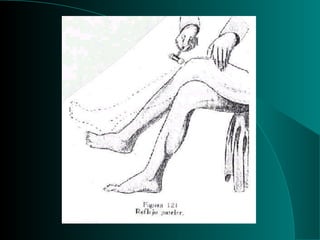
- 31. EXPLORACION DEL MOVIMIENTO REFLEJO REFLEJOS OSTEOTENDINOSOS O PROFUNDOS . Contracciones musculares involuntarias, inmediatas y breves, que se producen al percutir un tendón con un martillo de reflejos, en un punto determinado. Se buscarán los siguientes reflejos: Reflejos orbicular de los párpados, maseterino, bicipital, tricipital, rotuliano, aquiliano. REFLEJOS CUTANEOMUCOSOS O SUPERFICIALES.- Exploran una región determinada de la piel o mucosa correspondiente. Usar la yema de los dedos, un lápiz, un alfiler o el mango de un martillo de reflejos. Ejm. Reflejo corneal, cutaneoabdominal, cremasteriano,plantar.
- 50. REFLEJOS PATOLOGICOS SIGNO DE BABINSKI .- Inversión del reflejo plantar. Si es discreto buscar sucedáneos: OPPENHEIM .- Presionar la cara interna de la tibia de arriba hacia abajo. SCHAFER .- Comprimir el tendón de Aquiles GORDON .- Comprimir las masas musculares de la pantorrilla. CHADDOCK .- Frotar la piel de maleolo externo
- 51. REFLEJOS PATOLOGICOS SIGNO DE HOFFMAN .- La percusión del pulpejo del dedo medio de la mano del lado afectado provoca la flexión del pulgar de dicha mano. R. PALMOMENTONIANO .- La excitación de la eminencia hipotenar con el dedo produce la contracción de los músculos del mentón. Traduce lesión de la corteza pre frontal homolateral. R. DE SUCCION .- Al estimular la mucosa labial se produce movimientos de succión. CLONUS DEL PIE .- Serie de sacudidas rápidas del pie obtenidas por dorsiflexión forzada y rápida del mismo, mientras la pierna es sostenida por la otra mano del examinador colocada bajo el hueco poplíteo. Un clono que decae rápidamente puede ser normal.
- 60. MOVIMIENTO AUTOMATICO Movimiento realizado sin el concurso de la voluntad y la vigilancia de la conciencia, lo que permite ahorrar energía. Los más frecuentes son: MIOCLONIAS.- Contracciones musculares bruscas y rápidas que producen desplazamientos principalmente en extremidades inferiores TEMBLOR CEEBELOSO. TEMBLOR PARKINSONIANO, etc.
- 61. OFTALMOPLEJIA INTERNUCLEAR Figure. - Eye movements in internuclear ophthalmoplegia (INO) resulting from a lesion of the medial longitudinal fasciculus bilaterally.
- 62. ATAXIA SENSORIAL Figure .- Principal sites of spinal cord disease (shading) in disorders producing sensory ataxia.
- 63. OFTALMOPLEJIA POR LESIÓN PONTINA Figure .- One-and-a-half syndrome. This results from a pontine lesion (shaded area) involving the paramedian pontine recticular formation (lateral gaze center) and medial longitudinal fasciculus, and sometimes also the abducens (VI) nucleus, and affecting the neuronal pathways indicated by dotted lines. Attempted gaze away from the lesion ( A ) activates the uninvolved right lateral gaze center and abducens (VI) nucleus; the right lateral rectus muscle contracts and the right eye abducts normally. Involvement of the medial longitudinal fasciculus interrupts the pathway to the left oculomotor (III) nucleus, and the left eye fails to adduct. On attempted gaze toward the lesion ( B ), the left lateral gaze center cannot be activated, and the eyes do not move. There is a complete (bilateral) gaze palsy in one direction (toward the lesion) and one-half (unilateral) gaze palsy in the other direction (away from the lesion), accounting for the name of the syndrome.
- 64. PUNCIÓN LUMBAR Figure 11–1. Lateral decubitus position for lumbar puncture.
- 65. FISIOPATOLOGIA DEL REFLEJO PUPILAR Figure. - Anatomic basis of the pupillary light reflex. The afferent visual pathways from the retina to the pretectal nuclei of the midbrain are represented by dashed lines and the efferent pupilloconstrictor pathways from the midbrain to the retinas by solid lines. Note that illumination of one eye results in bilateral pupillary constriction.
- 66. TIPOS DE RESPIRACION EN EL COMA Figure .- Ventilatory patterns in coma. Cheyne-Stokes respiration and central hyperventilation are seen with metabolic disturbances and with structural lesions at a variety of sites in the brain. They are therefore not useful for anatomic localization of disorders producing coma. Ataxic and gasping ventilatory patterns are most commonly seen with pontomedullary lesions.
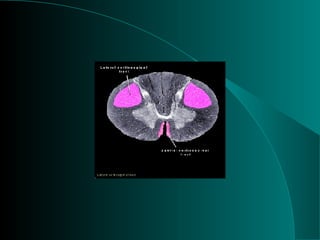
- 67. SINDROME DE WALLENBERG Figure .- Lateral medullary infarction (Wallenberg's syndrome) showing the area of infarction (shaded), anatomic structures affected.
- 68. SIGNOS NEUROLOGICOS EN EL COMA Figure 10–2. Neurologic signs in coma with downward transtentorial herniation. In the early diencephalic phase, the pupils are small (about 2 mm in diameter) and reactive, reflex eye movements are intact, and the motor response to pain is purposeful or semipurposeful (localizing) and often asymmetric. The late diencephalic phase is associated with similar findings, except that painful stimulation results in decorticate (flexor) posturing, which may also be asymmetric. With midbrain involvement, the pupils are fixed and midsized (about 5 mm in diameter), reflex adduction of the eyes is impaired, and pain elicits decerebrate (extensor) posturing. Progression to involve the pons or medulla also produces fixed, midsized pupils, but these are accompanied by loss of reflex abduction as well as adduction of the eyes and by no motor response or only leg flexion upon painful stimulation. Note that although a lesion restricted to the pons produces pinpoint pupils as a result of the destruction of descending sympathetic (pupillodilator) pathways, downward herniation to the pontine level is associated with midsized pupils. This happens because herniation also interrupts parasympathetic (pupilloconstrictor) fibers in the oculomotor (III) nerve.
- 70. VIA VESTIBULAR PERIFERICA Y CENTRAL Figure 3–1. Peripheral and central vestibular pathways. The vestibular nerve terminates in the vestibular nucleus of the brainstem and in midline cerebellar structures that also project to the vestibular nucleus. From here, bilateral pathways in the medial longitudinal fasciculus ascend to the abducens and oculomotor nuclei and descend to the spinal cord.
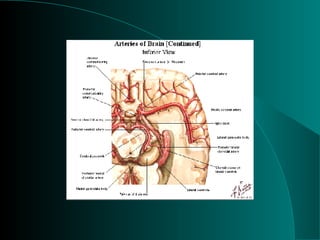
- 71. MALFORMACION ARTERIOVENOSA Figure 34-23 Left temporal arteriovenous malformation (AVM), demonstrated by MRI (above), and angiography (below). The patient was a 59-year-old woman with longstanding complaints of headache.
- 72. HEMORRAGIA INTRACEREBRAL Figure 34-19 An unenhanced CT scan showing the typical picture of a massive primary (hypertensive) hemorrhage in the basal ganglia. The third ventricle and ipsilateral lateral ventricle are compressed and displaced by the expanding mass (12 h after onset of stroke).
- 73. INFARTO CEREBRAL Figure 34-17 Massive ischemic infarct of left cerebral hemisphere in the distribution of the middle cerebral artery. CT scans taken 24 h (left) and 72 h (right) following the onset of neurologic symptoms. The second scan demonstrates marked swelling of the infarcted tissue and displacement of central structures.
- 74. HEMORRAGIA SUBARACNOIDEA Figure 34-22 Subarachnoid hemorrhage due to rupture of a basilar artery aneurysm. Left. Axial CT scan image at the level of the lateral ventricles showing widespread blood in the subarachnoid spaces and layering within the ventricles with resultant hydrocephalus. Right. At the level of the basal cisterns blood can be seen surrounding the brainstem, in the anterior sylvian fissures and the anterior interhemispheric fissure. The temporal horns of the lateral ventricles are again enlarged, reflecting acute hydrocephalus.
- 75. HEMORRAGIA TALAM Figure .- CT scan of a left thalamic hemorrhage that caused hemiplegia and hemisensory loss in a hypertensive patient.
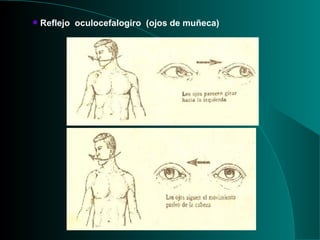
- 76. Reflejo oculocefalogiro (ojos de muñeca)
- 77. SENSIBILIDAD
- 78. EXAMEN DE LA FUNCION SENSITIVA SENSIBILIDAD .- Función del S.N. A través del cual el hombre reacciona frente a las excitaciones internas y del muindo exterior que los rodea. CLASIFICACIÓN : 1 .- S. General o Somática: Sensibilidad Superficial.- Tacto grosero : Fascículo espinotalámico ventral Termoalgesia : Fascículo espinotalámico dorsal. Sensibilidad Profunda.- Propiocepción conciente : Fascículo de Goll y de Burdach. Propiocepción inconciente : Fascículos espinocerebelosos 2.- S. Especial o de los Sentidos
- 81. PROPIOCEPCION: TACTO Y PRESION
- 83. EXPLORACION DE LA SENSIBILIDAD Sensibilidad Superficial: Tactil grosera .- Con algodón o pincel, desde el cuello hasta los pies y en forma comparativa. Termoalgesia .- Se utiliza 2 frascos con agua helada y caliente y 2 alfileres. Sensibilidad Profunda: S. Dolorosa profunda.- Proporciona información visceral, a través de compresión de testículos y / o pezones. Barognosia .- Capacidad para percibir el peso de los cuerpos. Barestesia .- Presión ejercida sobre una parte del cuerpo. Palestesia .- Sensibilidad del periostio a estímulos vibratorios. Se utiliza el diapasón. Topognosia .- Sentido de lugar. Hylopgnosia .- Consistencia de los cuerpos. Dermolexia .- Identificar letras o números trazados sobre la piel. Morfognosia .- Características y forma de los cuerpos. Batiestesia .- Sentido de las actitudes segmentarias. Estereognosia .- Capacidad para reconocer objetos. Requiere de la hylopgnosia y de la morfognosia.
- 84. ALTERACIONES DE LA SENSIBILIDAD Hipoestesia .- Disminución de todas las formas de sensibilidad. Anestesia .- Pérdida total de la sensibilidad. Hipoalgesia .- Disminución de la sensibilidad Analgesia .- Pérdida de la sensibilidad dolorosa. Anestesia disociada .- Pérdida de una forma de sensibilidad con preservación de otra. Disociación Siringomiélica.- Pérdida de la termoalgesia con conservación de tactil y profunda. Disociación Tabética.- Pérdida de la sensibilidad tactil y profunda con preservación de la termoalgesia.
- 85. COORDINACION
- 86. EXAMEN DE LA COORDINACIÓN COORDINACION .- Acción conjunta y armoniosa de las partes y perfecta sincronización de las funciones- EXPLORACION DE LA COORDINACION METRIA .- Prueba indice - nariz; Talón – rodilla y otras CRONOMETRÍA .- Prueba de steward- Holmes o de rebote DIADOCOCINESIA .- Prueba de las marionetas, o pálma y dorso. SINERGIA .- Asociación armonica de los movimientos elementales simultáneos. Observar la marcha. REGULARIDAD DEL MOVIMIENTO .- Prueba del vaso con agua. Observar si aparece temblor, el cual es intencional.
- 88. PRUEBA TALON – RODILLA
- 91. SIGNOS MENINGEOS 1.- Rigidez de nuca 2.- Kerning 3.- Brudzinski
- 92. SIGNO DE KERNING
- 93. SIGNO DE KERNING
- 97. EXPLORACION DE LA OLFACION Con sustancias aromáticas: 1.- Alcohol 2.- Tabaco 3.- Café . Examen fosa nasal por separado Huele o no huele olor agradable o no Identificar el olor
- 98. ALTERACIONES DE LA OLFACION ANOSMIA .- Pérdida del sentido del olfato HIPOSMIA .- Disminución del sentido del olfato HIPEROSMIA .- Sensación de olores se hacen fuertes CACOSMIA .- Percepción de malos olores. PAROSMIA .- Distorsión del sentido del olfato> Cortical ALUCINACIONES OLFATORIAS .- Percepciòn de olores sin que exista estímulo.
- 99. EXPLORACION DEL NERVIO OPTICO AGUDEZA VISUAL Tabla de Jaeger: a 30 cm. de distancia. Tabla de Snellen: a 6 metros de distancia VISION DE COLORES ¨Prueba de las madejas de lana de Holmgren Prueba de las madejas de Ishihara CAMPOS VISUALES Campimetría de confrontación. FONDO DE OJO Observar bordes y color de la papila óptica y color de la mácula
- 100. CAMPOS VISUALES
- 101. CAMPOS VISUALES Figure . Normal limits of the visual field
- 102. FONDO DE OJO Figure .- The normal fundus. The diagram shows landmarks corresponding to the photograph. (Photo by Diane Beeston; reproduced with permission, from Vaughan D, Asbury T, Riordan-Eva P: General Ophthalmology, 15th ed. Appleton & Lange, 1992.)
- 103. PAPILEDEMA Figure 4–11. Appearance of the fundus in papilledema. A: In early papilledema, the superior and inferior margins of the optic disk are blurred by the thickened layer of nerve fibers entering the disk. B: Swollen nerve fibers (white patches) and hemorrhages can be seen. C: In fully developed papilledema, the optic disk is swollen, elevated, and congested, and the retinal veins are markedly dilated. D: In chronic atrophic papilledema, the optic disk is pale and slightly elevated, and its margins are blurred. The white areas surrounding the macula are reflected light from the vitreoretinal interface. The inferior temporal nerve fiber bundles are partially atrophic (arrows) . (Photos courtesy of WF Hoyt.)
- 104. EXPLORACION DE LOS OCULOMOTORES ( III, IV, VI ) Examen de pupilas Forma, tamaño Reflejo motor y consensual Examen posición palpebral Examen posición de los globos oculares : PPM Examen movimiento de los globos oculares : Ducciones : Ojo por ojo, 6 posiciones cardinales de la mirada. Versiones .- Con los 2 ojos: 9 posiciones de la mirada
- 105. EXAMEN DE LA PUPILA FORMA .- Circular. Contorno irregular: Discoria TAMAÑO .- Diámetro normal: 2 – 4 mm, relacionado con intensidad de luz. Depende: Motor ocular común. Simpático cervical ALTERACIONES ANISOCORIA .- Desigualdad de las pupilas MIOSIS .- Disminución del tamaño: 2 tipos: 1 .- Espasmódica : Excitación del III par 2.- Paralìtica : Lesión del simpático cervical. MIDRIASIS .- Aumento de tamaño: 2 tipos: 1.- Espasmódica : Excitación del Simpático cervical 2.- Paralítica : Lesión del III par
- 106. OFTALMOPLEJIA III Figure 4–14. Clinical findings with oculomotor (III) nerve lesion. With the ptotic lid passively elevated, the affected ( right ) eye is abducted. On attempted downgaze, the unaffected superior oblique muscle, which is innervated by the trochlear (IV) nerve, causes the eye to turn inward.
- 107. OFTALMOPLEJIA VI PAR Figure 4–16. Clinical findings with abducens (VI) nerve lesion. The affected (right) eye is adducted at rest ( A ) and cannot be abducted ( B ).
- 108. DISTRIBUCION DEL NERVIO TRIGEMINO
- 109. EXPLORACION DEL NERVIO TRIGEMINO ( V ) Examen del componente sensitivo Sensibilidad superficial: Oftalmico, maxilar superior, maxilar inferior. Examen del componente motor. Palpar los maseteros y temporales cuando se comprimen las arcadas dentarias. Movimientos de deglución. Reflejos Reflejo corneal : Estimular la cornea Reflejo estornutatorio : Estimular las fosas nasales. Reflejo nauseoso : Estimular el velo del paladar
- 110. EXPLORACION DEL FACIAL ( VII ) Inspección: Simetría facial Examen componente motor. Gestos de : Arrugar la frente. Mover comisura labial Silbar, Soplar. Examen sensibilidad del pabellón auricular. Examen del gusto, ( 2/3 anteriores de la lengua ) Acido, dulce, salado. 5. Reflejo corneal y palpebral
- 112. EXPLORACION DE LA AUDICION ( VIII ) Examen de la percepción del sonido. a) Por trasmisión aérea : Palabra hablada o cuchicheada Por trasmisión ósea Examen con diapasón: Prueba de Weber Prueba de Rinne Prueba de Schwabach.
- 113. EXAMEN RAMA VESTIBULAR ( VIII ) Anamnesi s : Vértigos objetivos Examen : Observar si hay nistagmus Bipedestación con ojos cerrados Lateralización del eje corporal Desviación de la marcha con ojos cerrados: Estrella de Babinski y Weil
- 114. EXPLORACION DEL IX y X 1.- Examen del gusto.- ( 1/3 posterior de la lengua) Sabor amargo 2.- Examen de la deglución. 3.- Examen del velo del paladar 4.- Examen del reflejo nauseoso
- 116. EXPLORACION DEL NERVIO ESPINAL ( XI ) 1.- Examen de la voz 2.- Examen de las cuerdas vocales 3.- Examen de los músculos: Esternocleidomastoideo Trapecio
- 117. EXPLORACION DEL NERVIO GLOSOFARINGEO ( XII ) 1.- Inspección de la lengua Dentro y fuera de la cavidad oral Estado trófico de la hemilengua 2.- Examen del movimiento de la lengua
- 120. FUNCIONES NERVIOSAS SUPERIORES Son básicamente las siguientes: El lenguaje La praxia 3. La gnosia Lenguaje .- Función mental que permite al hombre comunicarse con sus semejantes y con el mismo. Área de Broca .- En relación con el lenguaje expresivo Área de Wernike .- En relación al lenguaje compresivo.
- 121. AREAS DEL LENGUAJE
- 122. AFASIA Trastorno en la expresión o en la comprensión de los símbolos verbales, independientemente del compromiso de los instrumentos periféricos de ejecución o de recepción. Afasia de Broca .- Alteración en el lenguaje expresivo: desde el mutismo o la emisión de sonidos inarticulado s y/o repetición AfasiadeWernicke .- Alteración en el lenguaje compresivo:
- 123. PRAXIA .Realización de actos que conllevan a un :fin determinado EXAMEN DE LA PRAXIA 1. Observar actos de la vida cotidiana, la actividad automática. 2. Observar el comportamiento de la persona al comando, ordenando en forma sistemática la ejecución de una orden.
- 124. GNOSIA Comprensión del mundo exterior. También se le define como el reconocimiento de los objetos. EXAMEN DE LA GNOSIA Gnosia Visual. o Reconocimiento de objetos o Identificación de colores Gnosia Auditiva. o Reconocimiento de objetos por el sonido o Reconocimiento de melodías Gnosia Perceptiva. o Estereognosia
- 151. ALTERACIONES MOTORAS o Las más frecuentes son las hemiplejías I hemiparesias: a. H. Global o DroDorcionaL-Cuando se afecta un hemicuerpo in toto. b. H. Predominante.- Cuando predomina en algunas de las extremidades. c. H. Comun.- Parálisis de miembros y par craneal son contralaterales. d. H. Alterna.- Parálisis de miembros es contralateral y el par craneal homolateral e. H. Cruciata.- Parálisis de un miembro superior es contralateral con respecto al otro inferior. f. H. Directa.- Parálisis es homolateral a la lesión.
- 154. SINDROMES MOTORES 1. Síndrome de la neurona motora central: o Parálisis o paresias o Conservación de algunos movimientos involuntarios(sincinesias) o Hipertonía piramidal: espasticidad o No hay atrofia muscular o No hay fibrilación muscular o Respuestas eléctricas normales (EMG) o ROT exaltados o Reflejos patológicos (Babinski y sucedáneo s) 2. Síndrome de la neurona Ileriférica: o Parálisis de distribución segmentaria o Ausencia de movimientos involuntario s o Hipotonía o flacidez o Presencia de atrofia muscular o Presencia de fasciculaciones musculares o Respuestas eléctricas de degeneración (EMG) o Abolición de reflejos o hiporreflexia. o No reflejos patológicos.
- 155. VIA SENSITIVA Figure 3–5. Pathway mediating proprioceptive sensation.