Awake Craniotomy Anaesthesia.pptx

1) Awake craniotomy is a technique used for brain tumor excision from eloquent areas of the brain to allow for brain mapping during surgery while the patient is awake. 2) The anesthesiologist's role includes extensive preoperative psychological preparation of the patient, administration of sedation and analgesia during surgery to maintain the patient's comfort and cooperation during brain mapping, and careful titration of medications to avoid complications. 3) There are two main anesthetic approaches for awake craniotomy - monitored anesthesia care with sedation or asleep-awake-asleep general anesthesia. Both have benefits and risks depending on factors like surgery duration and patient characteristics. Careful planning and execution of the anesthetic technique











































Awake Craniotomy Anaesthesia.pptx
- 1. DR UNNIKRISHNAN P MD,DA,PDCC,MBA ASSISTANT PROFESSOR DEPT OF ANESTHESIA SCTIMST, TRIVANDRUM ANESTHETIC CHALLENGES IN AWAKE CRANIOTOMY
- 2. Is the population becoming more sensitive? • Not sure; but the BRAIN IS STILL REMAINING INSENSITIVE !!!
- 3. What’s the fun if everyone tells the same? Awake Craniotomy Craniotomy with Intraoperative awakening
- 4. Why Awake Craniotomy ? • Is a technique used for brain tumour excision from eloquent cortex, epilepsy surgery, and deep brain stimulation surgery • Why a tumour in the eloquent area needs the patient to be awake during surgery? • fMRI, DTI • MEP, SSEP ? Spinal; I want GA
- 5. How it goes?
- 6. As an anesthesiologist, what you are going to do preoperatively? • Patients selected, on the basis of history and characteristics, the likely extent and duration of brain mapping required, and the likely ease of excision of the tumour • Significant burden of anxiety for the patient • Prepare the patient psychologically; explain the procedure • Simulate their positioning on the operating table, mapping tests, and honestly discuss possible negative feelings (dry mouth, pain during manipulations), as well as suggested ways to correct them
- 7. Premedication • Patients must take their usual steroid, anti-epileptic*, or anti-hypertensive medication, or anti aspiration prophylaxis (if indicated) • Seizures (2.9 to 54%) mostly during cortical mapping • Risk factors: h/o preoperative seizures and the mastery of the mapping technique • Antibiotics, pre-incision • Nausea & vomiting will increase ICP; give antiemetics • Paracetamol intraoperatively
- 8. There should not be any communication gap between the two: • Position / Table* • Patient cooperation • Comorbidities • MAC or AAA • Local anesthesia • Timings of drug administration • Closure
- 9. First impression is the best impression • The sedation and analgesia profile during the first phase of awake craniotomy (i.e., scalp incision, bone flap removal, dura opening) plays the crucial role in the quality of intraoperative emergence
- 10. The position • The patient position is dictated by the location of the lesion. • This is usually a lateral or supine position, but with occipital lesions and testing the visual cortex, a sitting position may be used
- 12. Actively involve in the positioning of the patient • The ability to communicate with the patient and access to the patient should be maintained at all times. Sterile drapes shouldn’t encroach on patients face
- 13. Monitors • Arterial line* • Capnography* • Depth of anesthesia monitors* • Urinary catheterization*
- 14. Scalp Block and it should not hurt the patient… is your first step
- 15. Stuff for Junior Residents • What % of lignocaine solution do you use to infiltrate brain parenchyma?
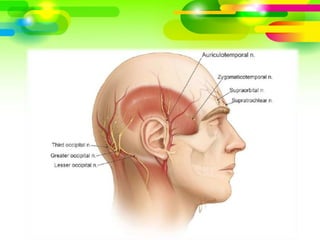
- 16. Scalp Block: The Do’s • Bilateral scalp block before pinning of the head in Mayfield Pins • Communicate it with the neurosurgeon (Temporalis fascia, dura mater infiltration) • Analgesia even up to 6-8 hours • Bupivacaine, levobupivacaine or ropivacaine • Chlorhexidine or betadine, sterile gloves and a 23 G needle, the local anaesthetic is infiltrated into the following sites:
- 19. Our technique should ensure # • Patient is awake, co-operative and comfortable during the mapping phase • Acquisition of reliable neurophysiological monitoring signals • A soft and slack brain during resection. • Hemodynamic stability especially during painful phases (skull pin placement, the craniotomy itself and dural opening).
- 20. Which is the best approach? • There is no recognized consensus on the best anaesthetic approach • It depends on the surgeon, pathology, length of surgery, and patient factors • Most neuroanaesthetists have usually developed a preferred technique and believe their own approach to be the safest and the best MAC AAA
- 21. Monitored Anesthesia Care (MAC) • Anesthesia Technique
- 22. Fine titration… ↓sedative load, spontaneous ventilation Avoid sharp asleep to awake transition ↓hypo/hyper active delirium , ↑ mapping reliability Sedation deepened during painful events Stopped during mapping & resection Restarted for closure
- 23. Problems • If the level of sedation is not titrated correctly: • Risks of airway obstruction which can lead to hypercapnia, hypoxia, and increased intracranial pressure with a ‘tight’ brain, or • A patient who is not adequately sedated will be uncomfortable and anxious
- 24. Dexmedetomidine is it the Most Suitable Drug (MSD) in awake surgeries ??!! • Calm, cool patient! • Anxiolysis-Analgesic-Opioid sparing* • No effect on ICP • Less respiratory depression less hypercapnia • Easily arousable despite sedation • Less nausea & vomiting • Loading dose of 0.5–1.0 ug/kg over 20 min f/b an infusion rate of 0.2–0.7 ug/kg/h + P’mol ± fentanyl • Can start start scalp block, towards the end of the LD
- 25. Dexmedetomidine : Issues • ?lack of suppression of preoperative epileptic activity by dexmedetomidine ?seizure incidence more • Significant variability in dose requirement among patients • Effects may not exactly get reflected in the BIS • It does accumulate to some extent: longer durations of infusion will result in a slower return to normal function • Bradycardia • Hypotension • Hypertension
- 26. Propofol + Opioid Moderate Sedation • Propofol infusion & Fentanyl increments (India) • TCI with Propofol & Remifentanil an excellent choice • Precise dosing very important: hypercapnia • Titrate according to BIS • TCI: Use Propofol Schnider model @ 2-4 ug/mL target concentration. Remifentanil @ 0.8-1 ng/mL
- 27. Volatile situation • Inhalational anesthetics are not optimal due to higher chances of a potential elevation of ICP, a higher risk of nausea and vomiting and emergence delirium • May not give an ideal situation for mapping • It seems rational to REDUCE RELIANCE ON OPIOIDS at preawake and awake phases due to potential somnolence on emergence and decreased quality of cooperation on the part of the patient
- 28. Asleep-Awake-Asleep (AAA) • Anesthesia Technique
- 29. AAA Advantages • Better comfort for the patient and surgical team during the preawake phase • Reliable protection of the patient from painful sensations • Protection from hypoventilation and opportunity to control brain swelling via hyperventilation • Protection from postoperative recollections about the awake phase • Prevents intraoperative movements by the patient GA/airway Drugs stopped NC Testing GA restarted
- 30. Drugs for GA • Propofol infusion (TCI/MCI) & Fentanyl increments • TCI with Propofol & Remifentanil an excellent choice • Volatile agent + Remifentanil • Titrate according to BIS • LMA/ ProSeal LMA/iGel/ Endotracheal tube • Controlled ventilation, ±NMBA.
- 31. A great teaching tool; cuts down the work load
- 32. We overcame all the hardships for this! • Currently, the gold standard technique for mapping involves direct cortical electrical stimulation while the patient is awake and able to attempt to perform a relevant task, to determine if the stimulus disrupts execution of the task. • A calm, quiet environment is required during this • Pain from the pins or discomfort from the prolonged immobility, agitation or nausea, and vomiting. • It is important to pick it and address it effectively as it can lead to poor surgical conditions
- 33. Mapping • The Broca’s area (for speech production and language processing) and the Wernicke’s area (for language comprehension),the motor and sensory cortex. • Any alteration of speech, language, and motor function by stimulation is communicated to the surgeon. • Resection takes place once the cortex has been functionally mapped by this process.
- 34. The climax… • The last phase of an awake craniotomy (haemostasis, dural, skull and skin closure) can be uncomfortable • Particularly during skin closure • Patient might have been lying immobile for some time, with resultant musculoskeletal discomfort • Scalp block start to wean
- 35. Challenging act! • Induction of GA at this stage requires experience and expertize • LMA insertion is often preferred - as tracheal intubation is challenging in these patients who are usually in a right lateral position, with the head clamped, and in an unfavourable position for laryngoscopy. • If MAC, can restart dexmedetomidine/ propofol • When surgery finishes, the pins removed and the patient woken up. • If remifentanil has been used, it can be run at low infusion rates to aid a ‘smooth’ wake-up and avoidance of coughing
- 36. How the literature compares both? • Eseonu CI et al, World Neurosurg 2017 :Similar; reduced duration in the MAC group • Sz Dilmen et al, J Clin Neurosci 2017 : seizures, agitation, PaCO2, non-critical desaturation, brain edema and c/o pain were more in MAC group • Elbakry et al, Minerva Anes 2017 : Dexmedetomidine MAC vs Propofol MAC, similar • Seuro et al, JNSA 2018 : MAC vs AAA Similar; lower incidence of respiratory and hemodynamics complications in the dexmedetomidine groups.
- 37. Goettel et al, BJA 2016 • Dexmedetomidine vs propofol remifentanil conscious sedation • fentanyl bolus the assigned drug regimen started Scalp Block Before and after mapping, sedation was titrated to MOAA/S score of 2–4 • In the propofol-remifentanil group, propofol was stopped, and remifentanil infusion rate decreased, 10 min before mapping. • In the dexmedetomidine group, the infusion rate was decreased to 0.1–0.4 mcg/kg/h 10 min before mapping. • Similar; DEX- lesser HR, more seizures. P-R: more adverse respiratory events
- 38. So which one is better? • If the overall procedure >4 hours AAA. MAC if <4 hours. • Once we get remifentanil….more options • TCI MAC and TCI AAA • For MAC, Dexmedetomidine Vs Propofol-Remifentanil TCI….
- 39. COMPLICATIONS How will you manage the..
- 40. Painful Facts • Despite the scalp block, complaints of pain during surgery are common. • Are sensations associated with manipulations of the skull-base structures or perivascular tractions. Local analgesics cannot resolve this • opioids can reduce the reliability of brain mapping. • The main solution to this problem may be a change in surgical approach: transcortical access to underlying tissues, avoiding traction of vessels, and skull-base structures
- 41. Seizures • treated by irrigating the brain tissue with ice-cold saline. • low doses of propofol • no benefits of prophylaxis with phenytoin or valproate • ? levetiracetam superior • If these fails: benzodiazepines, anti-epileptic drugs, or re-sedation with airway control • An emergency plan for airway control: LMA • Others: patient intolerance of the procedure, often because of the urinary catheter or prolonged positioning and intra-operative seizures. • Conversion rate to GA is less
- 42. Post Operative Care • Usually returns to ICU; in some centres to NS ward • Analgesia; scalp block may ↓ requirements • Close neurological monitoring especially in the first 6 h after operating; haematomas may require an urgent repeat craniotomy & evacuation • Most patients are in hospital for 1–2 days after operation • DAYCARE : Selection based on stringent inclusion and exclusion criteria, routine postoperative imaging for haematomas and access to advice after discharge
- 43. Claimed Advantages • Increased lesion removal • Minimize the damage to eloquent cortex • Shorter hospitalization time • Reduced cost of care • Decreased incidence of postoperative complications such as nausea and vomiting
- 44. Outcome • ? the frequency of new-onset postoperative neurological deficits after awake craniotomy is no less than that for surgery ↓GA • The cause is ischemic injury of the subcortical structures (internal capsule, etc.) or anatomical damage of the subcortical pathways. • Are often due to mistakes in mapping methodology, excessive sedation, or fatigue of the patient at the awake stage.
- 45. How to fix? • It seems that the most effective way to avoid these complications is to use a transcortical approach to deep structures, which prevents vascular traction and reduces risk of ischemic injury. • Such an approach can prevent fatigue and pain because sensitive tissues around the vessels and leptomeninges remain intact
- 46. THANK